Abstract
Background:
Five distinct fracture patterns have been recently described for the combined or isolated action of the attachments of the medial ulnar collateral ligament (UCL) and flexor pronator mass (FPM) on the medial elbow (Figure 1). This study seeks to evaluate injury patterns associated with each of the distinct fracture patterns.
Hypothesis:
Injuries associated with the UCL would be more likely to be related to throwing or overhead mechanisms, whereas complex injuries would be more likely to be traumatic in nature.
Methods:
A retrospective review of patients <18.9 years was performed from 2012 to 2022. Patients presenting with a medial elbow injury were identified using ICD and CPT codes and were classified by an orthopedic attending. Patients with bilateral injuries, a previous fracture, chronic injuries, or underlying bone disease were excluded. Data collected included patient and injury characteristics. Bivariate statistical analysis was performed. Five distinct fracture patterns were identified – Type 1: UCL Bony avulsion, Type 2: Type 1 + ME attached, Type 3: Classic ME fracture through the physis, Type 4: Cortical sleeve or shell-like fragment, Type 5: Type 1 + ME as two separate unconnected fragments. (Figure 1).
Results:
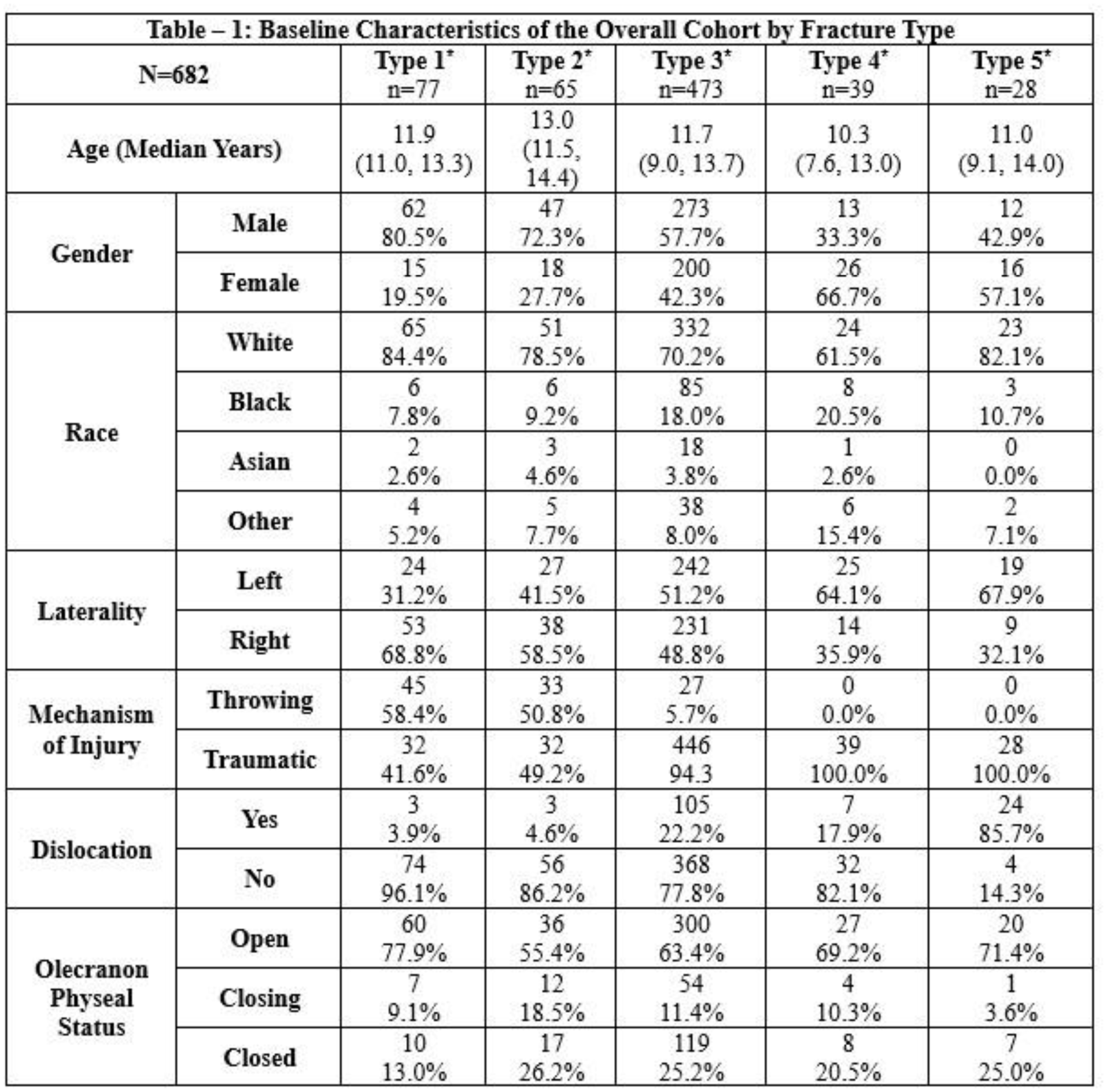
We identified 682 patients with a mean age of 11.5 years (3.3 – 18.1). Rate by type was I (11.3%), II (9.5%), III (69.4%), IV (5.7%), V (4.1%). With respect to age, Type IV injuries occurred in younger patients (median 10.3 years, IQR 7.6–13.0), while patients were generally older than 11 years in the other types (Table 1). Males had higher rates of Type I (80.5%) and II (72.3%) injuries. Throwing was the mechanism of injury in Type I and II in >50% of cases but was <5% in Type III, IV and V (p<0.001). Type II, IV and V were almost always traumatic injuries (>95%). Dislocation was more frequently seen in Type V (85.7%) compared to other types (19%) (p < 0.001).
Conclusion:
This large cohort confirmed five distinct fracture patterns that are identifiable on plain radiographs and are associated with specific injury mechanisms. Type I and II were preponderant to throwing-related injuries whereas Type III, IV and V were more frequently traumatic injuries and seen with dislocations. Future studies are needed to determine optimal management strategies for restoring medial elbow anatomy for individual patterns as well as for the anticipation of complications such as elbow stiffness or instability.