Abstract
Background:
Osteochondritis dissecans (OCD) is a condition characterized by focal subchondral bone avascular necrosis, resulting in potential articular cartilage disruption1. While mechanical trauma (commonly associated with certain sports) is regularly implicated, emerging literature also suggests biological and hereditary risk factors may contribute to OCD development1. However, the increased likelihood of developing OCD lesions associated with these risk factors has yet to be quantified. Therefore, we sought to quantify the relative risk associated with potential biological and sports-related risk factors utilizing a large, population-based dataset.
Hypothesis:
Vitamin D deficiency, hGH deficiency, coagulopathies, and specific sports participation are associated with an increased risk of developing OCD.
Methods:
We performed a retrospective analysis using the TriNetX Analytics Network (US Collaborative Network), a national database of de-identified electronic health records from over 30 million patients under 25 years of age. Eight medical conditions were selected for analysis: hGH deficiency, vitamin D deficiency, vWF deficiency, primary thrombophilia, hemophilia A, ITP, Factor V Leiden, and nicotine dependence. We generated separate cohorts to compare patients with and without theoretical risk factors. Additionally, we created cohorts comparing specific sports participation. Relative risks were calculated for each risk factor.
Results:
Of the medical risk factors analyzed, Factor V Leiden had the highest relative risk of OCD development (RR: 3.136; 95% CI: 2.136 – 4.606). Hemophilia A patients demonstrated the second greatest risk (RR: 2.918; 95% CI: 1.729 – 4.926. All other risk factors (hypopituitarism, vitamin D deficiency, vWF deficiency, primary thrombophilia, and immune thrombocytopenic purpura) showed a significant but modest increased relative risk apart from nicotine dependence, which yielded a lower relative risk compared to controls (Figure 1).
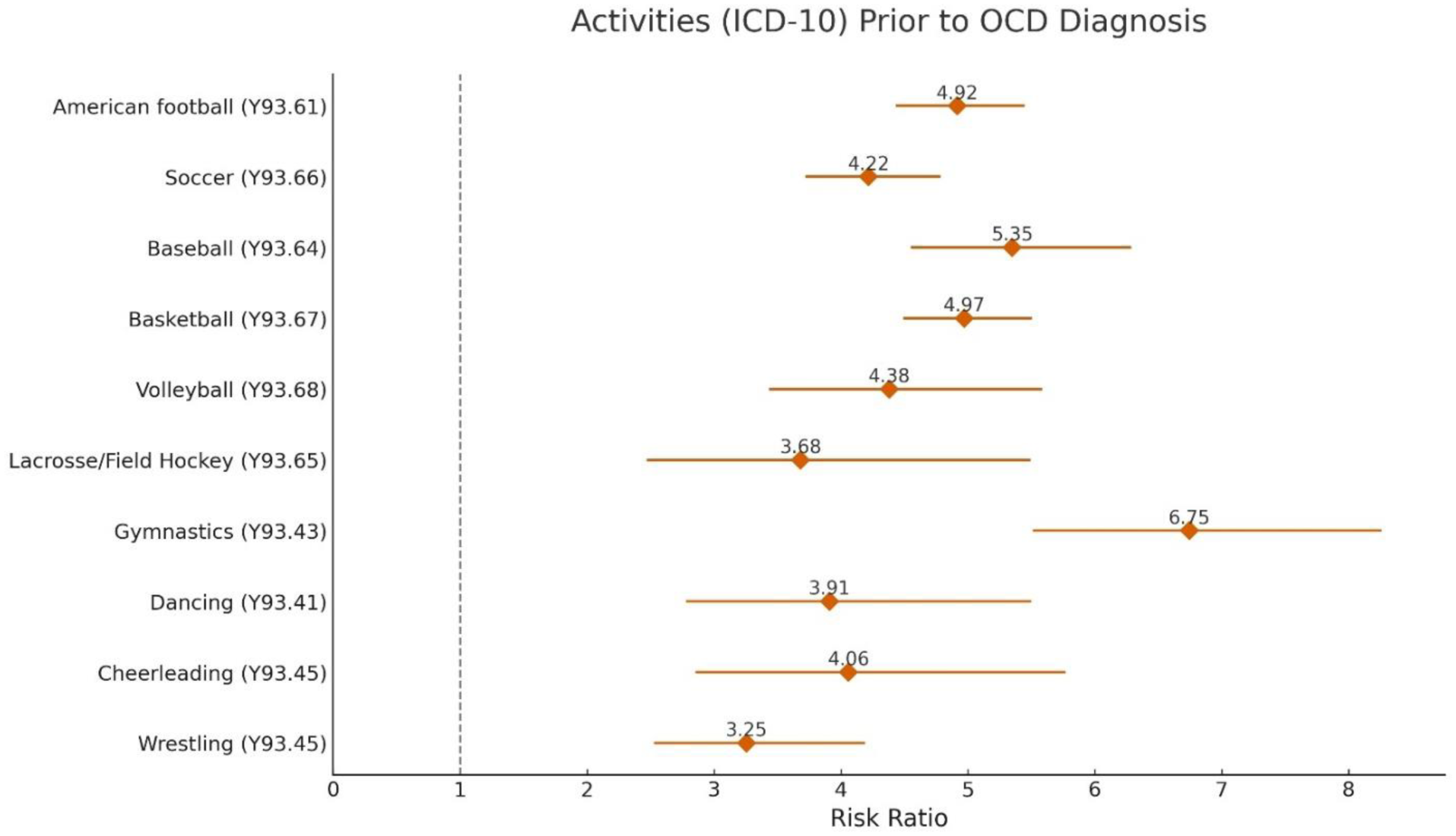
Of all sports, gymnastics exhibited the greatest risk for OCD development (RR: 6.747, 95% CI: 5.511 – 8.26) followed by baseball, basketball, and American football (Figure 2). Compared to non-sport participation controls, all sports analyzed demonstrated an increased risk for OCD development.
Conclusion:
To our knowledge, this is the first large-scale analysis to quantify the relative risk of developing OCD associated with participation in common youth sports. Several coagulopathic conditions that had not been previously identified specifically were associated with significantly increased risk. Interestingly, nicotine dependence was linked to a reduced risk of developing OCD lesions, although this finding may reflect athletes having a lower likelihood of nicotine use. This data could be utilized to develop activity and medical risk factor specific screening programs for at-risk youth.