Abstract
Background:
The Lower-Quarter Y-Balance Test (LQ-YBT) is used to evaluate dynamic stability after anterior cruciate ligament reconstruction (ACLR) [1,2]. However, limited evidence exists indicating whether LQ-YBT is associated with hip and knee isokinetic strength ratios in youth athletes following ACLR.
Hypothesis:
It was hypothesized that shorter anterior reach on LQ-YBT would be associated with lower isokinetic knee strength ratios, and shorter posteromedial reach would be associated with lower hip strength ratios. Secondarily, graft type would have an effect on both knee and hip strength ratios.
Methods:
Patients cleared to return to sport following ACLR were recruited and completed LQ-YBT and isokinetic strength testing of the hip and knee (Biodex). The knee strength ratio (hamstring to quadriceps, H:Q) was calculated by dividing concentric hamstring by quadriceps peak torque, normalized to body weight (Nm/kg), while the hip strength ratio (adductor to abductor, AD:AB) was calculated by dividing body-weight-normalized concentric adductor by abductor peak torque. Anterior, posteromedial, and posterolateral distances of the LQ-YBT were leg-length-normalized and expressed as a percent of leg-length (%LL). Limb-to-limb differences (cm) in each direction were calculated as the difference in distance of the dominant limb compared to the non-dominant limb. To determine the predictability of LQ-YBT measures in estimating H:Q and AD:AB ratios, two multiple linear regressions were performed.
Results:
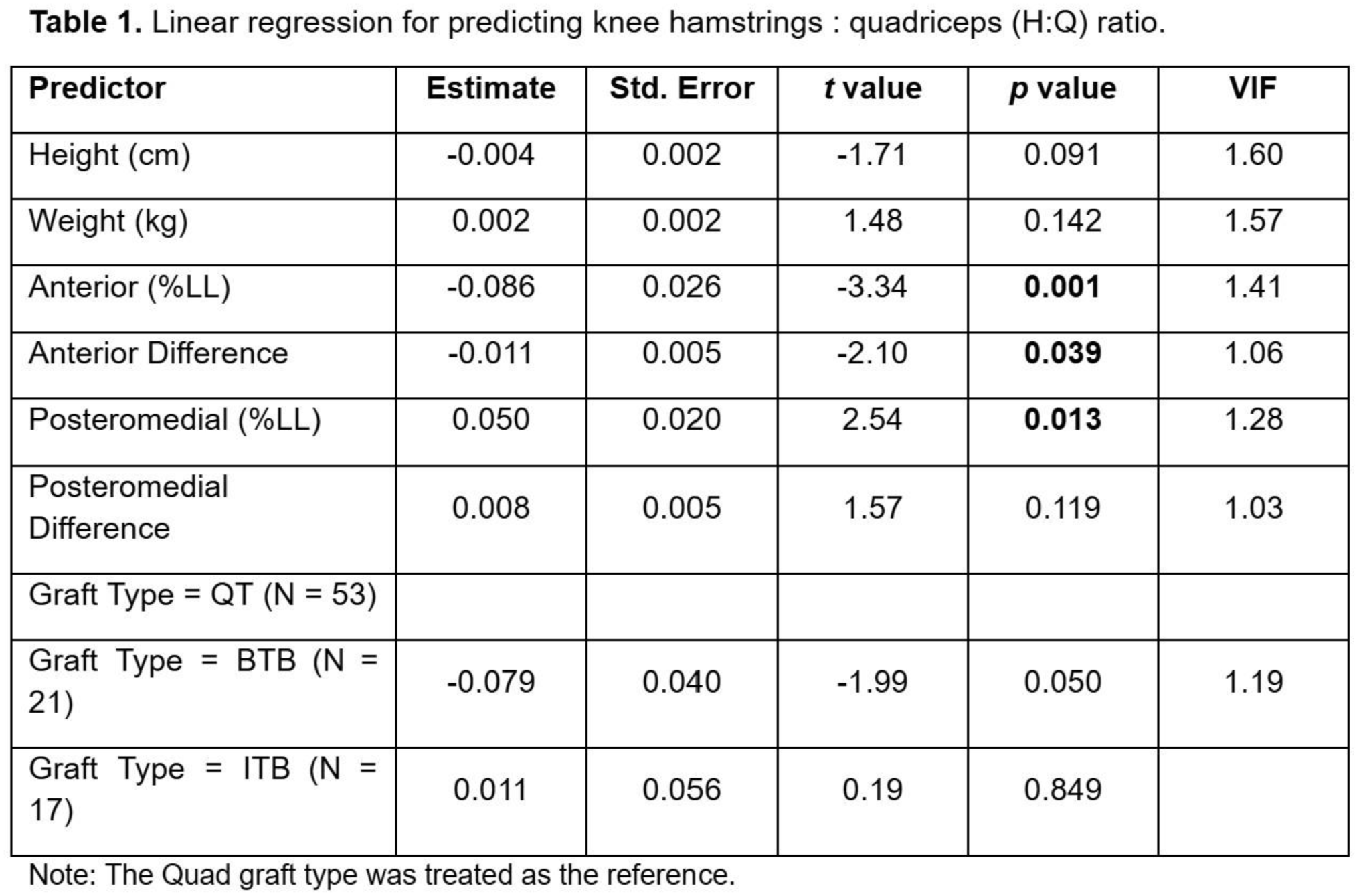
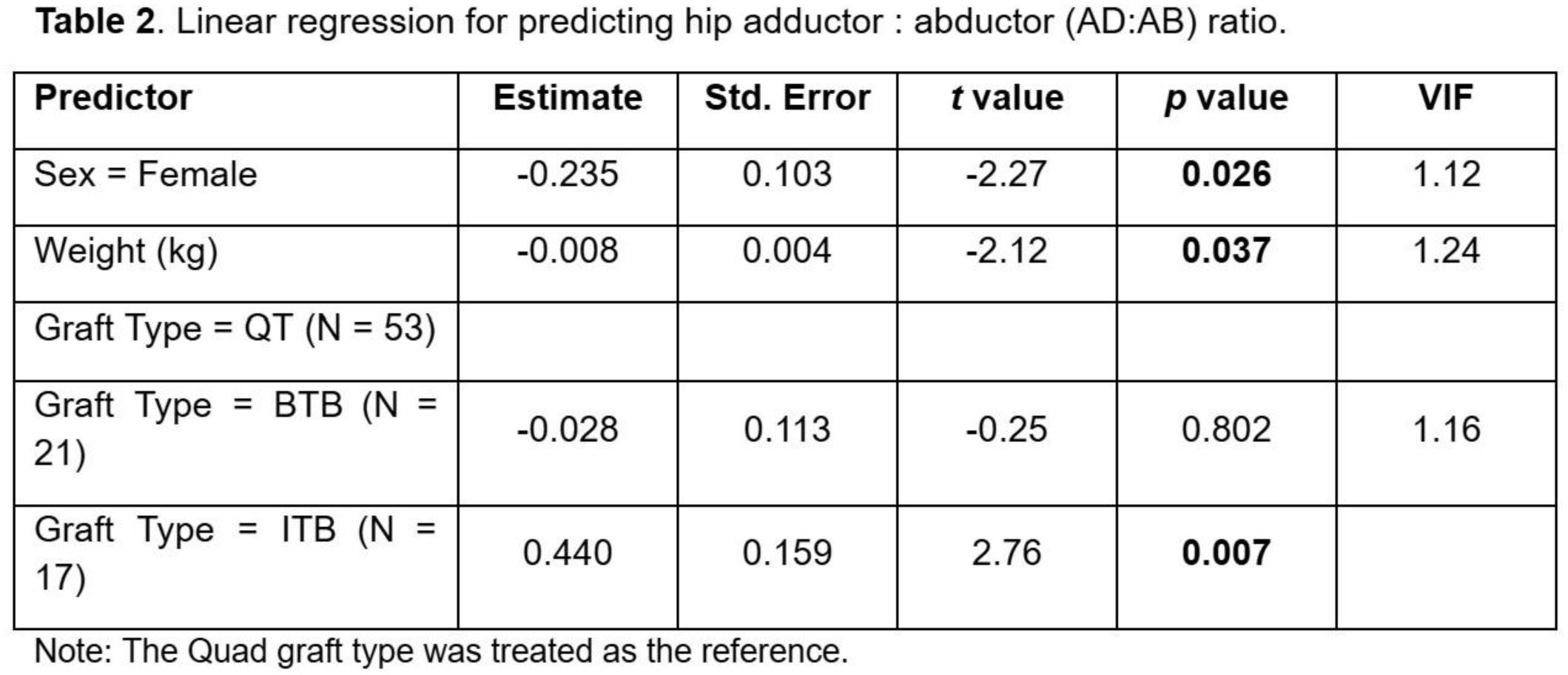
A total of 91 patients (51.2% female, 15.5±2.7 years, 64.3±15.4 kg, 164.8±10.1 cm, 58.7% quad graft) were included in the analysis. A one-unit increase in the anterior reach was associated with an 8.6% reduction in H:Q (p=0.001) Similarly, each unit increase in the corresponding limb-to-limb difference was significantly associated with 1.1% reduction in H:Q (p=0.039). A one-unit increase in the posteromedial reach was significantly associated with a 5.0% increase in H:Q (p=0.013) (Table 1). Additionally, female sex and a one-kilogram increase in body weight were associated with 23.5% (p=0.026) and 0.8% (p=0.037) reduced AD:AB ratios, respectively. In reference to the quadriceps tendon (QT) graft, having an ITB graft was associated with a greater AD:AB ratio compared to the QT graft (Table 2), regardless of age. No differences were found for the BTB graft type.
Conclusion:
LQ-YBT performance, particularly in the anterior and posteromedial directions, may reflect underlying strength imbalances at the knee and hip. These findings highlight the potential of the LQ-YBT as a clinical tool for identifying patients at risk of reinjury post-ACLR. Additionally, sex, body weight, and graft type should also be used to inform rehabilitation strategies for patients following ACLR.