Abstract
Background:
In skeletally immature patients, the modified MacIntosh anterior cruciate ligament (ACL) reconstruction (ACLR)—a combined intra- and extra-articular procedure utilizing iliotibial band autograft—is often utilized to minimize risk of physeal injury. This technique, incorporating a lateral extra-articular tenodesis (LET) by design, has an excellent track record with low re-rupture rates. However, some investigators have shown biomechanical evidence of supraphysiologic internal rotation (IR) constraint. It remains unclear, however, if such constraint also elevates lateral compartment pressures, conferring an increased risk of osteoarthritis. This study evaluated both rotational laxity and lateral compartment pressures in knees undergoing modified MacIntosh ACLR compared to the native state.
Objectives:
Contemporary modified MacIntosh ACLR decreases IR but does not lead to significantly elevated lateral compartment pressures compared to the ACL-intact state.
Methods:
This preliminary study evaluated three cadaveric adult knee specimens tested on a 6-degree-of-freedom robotic manipulator. Three states were tested: intact, ACL-transected, and modified Macintosh ACLR. The LET component of the ACLR was tensioned to 44N at 90° flexion and neutral rotation, and the intra-articular component was tensioned to 66N at 20° flexion as previously described. Laxity was assessed in three loading directions (134N anterior, 8Nm varus, and 5Nm IR). The maximum pressure at peak applied load and the center of pressure in the lateral compartment were measured using an intra-articular sensor during simulated pivot shift. Given the small sample size, difference ranges between states were reported with planned comprehensive comparative analyses with further testing.
Results:
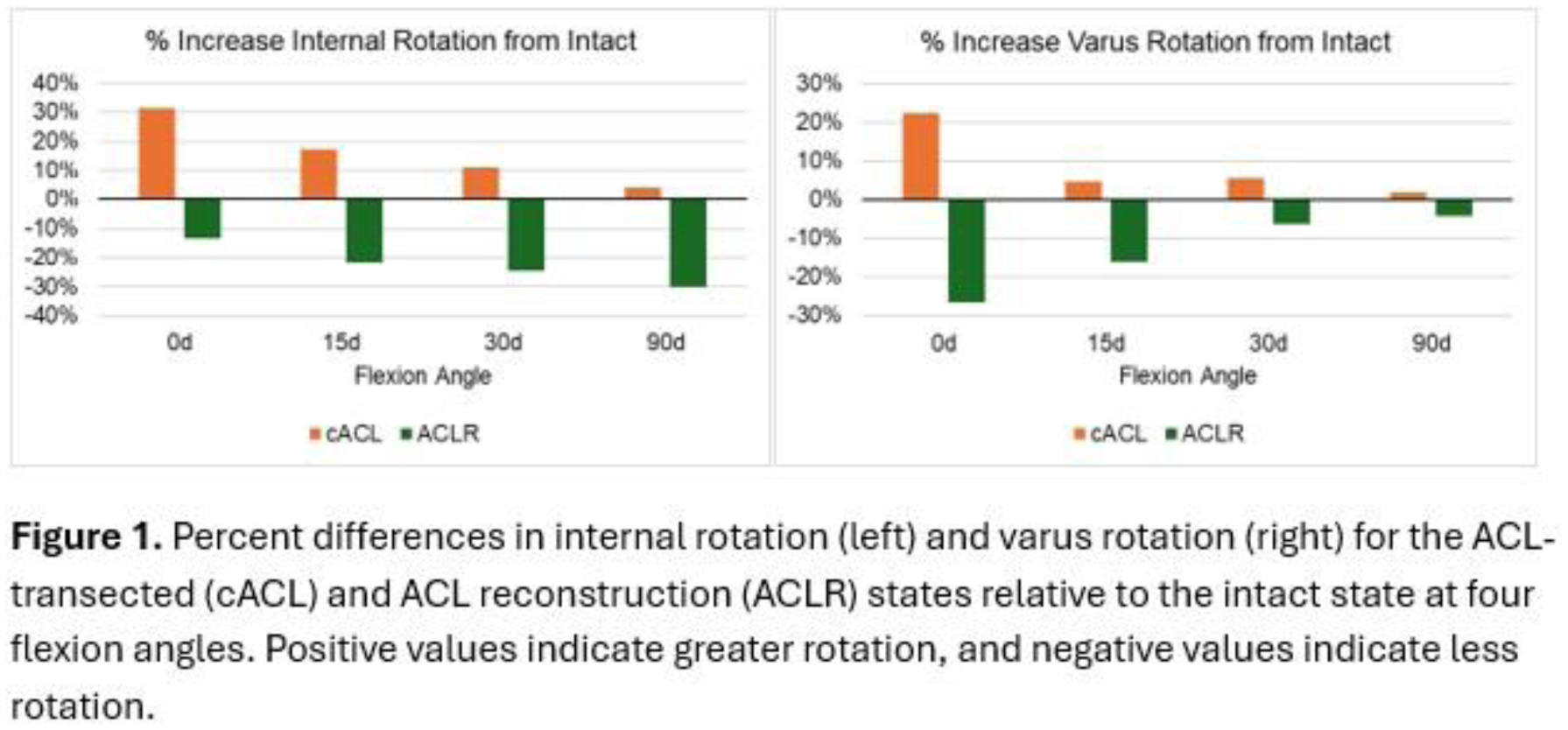
Anterior laxity at 30° was greater (3-15%) in the ACLR state compared to ACL-intact state. The largest reduction in IR laxity after ACLR was at 90° (26-38%) and the smallest at 0° (10-16%, Figure 1). The largest reduction in varus laxity after ACLR was at 0° (19-38%) and smallest at 90° (2-8%). During simulated pivot shift, peak lateral compartment pressure increased relative to intact by 0.8-1.1MPa and 0-0.4MPa for the ACL-transected and ACLR states, respectively (Figure 2). Relative to intact, the center of pressure shifted posteriorly by 1.3-3.9mm for the ACL-transected state and anteriorly by 0.5-4.0mm after ACLR.
Conclusion:
Compared to intact knees, modified Macintosh ACLR showed increased restraint to IR with increasing knee flexion and greater restraint to varus laxity in extension, like past biomechanical results after LET. Despite this apparent overconstraint, lateral compartment pressures were similar, suggesting no increased predisposition to osteoarthritis. Ongoing testing and inclusion of additional specimens will allow for more detailed comparative statistics.