Abstract
Background:
Patellar instability accounts for approximately 3% of knee injuries. Medial patellofemoral (MPFL) reconstruction, performed with either autograft or allograft tissue, is an important part of the treatment algorithm for patellar instability. While autograft may be associated with faster biologic remodeling allograft confers less donor site morbidity. Despite previous studies, there is not yet a consensus regarding the ideal graft type for MPFL reconstruction.
Objectives:
Graft type in MPFL reconstruction influences post-operative complication rates and patient-reported outcomes, with autograft associated with improved outcomes but potentially higher complication rates.
Methods:
Patients in this study were prospectively enrolled in the Justifying Patellar Instability Treatment by Early Results (JUPITER) multicenter study. Patients were included if they underwent an MPFL reconstruction and excluded if they underwent a concomitant boney or articular cartilage repair. Patients were stratified into cohorts based on MPFL reconstruction with autograft or allograft. Patient demographics and complications (subluxation/dislocation or reoperation) were reviewed and included. Patient reported outcome measures including the KOOS Jr., Pedi-FABS, IKDC Pedi score, BPII 2.0, and Kujala score were included at baseline, 1-, 2-, and 5 -years postoperatively. A P-value < 0.05 was statistically significant in all analyses.
Results:
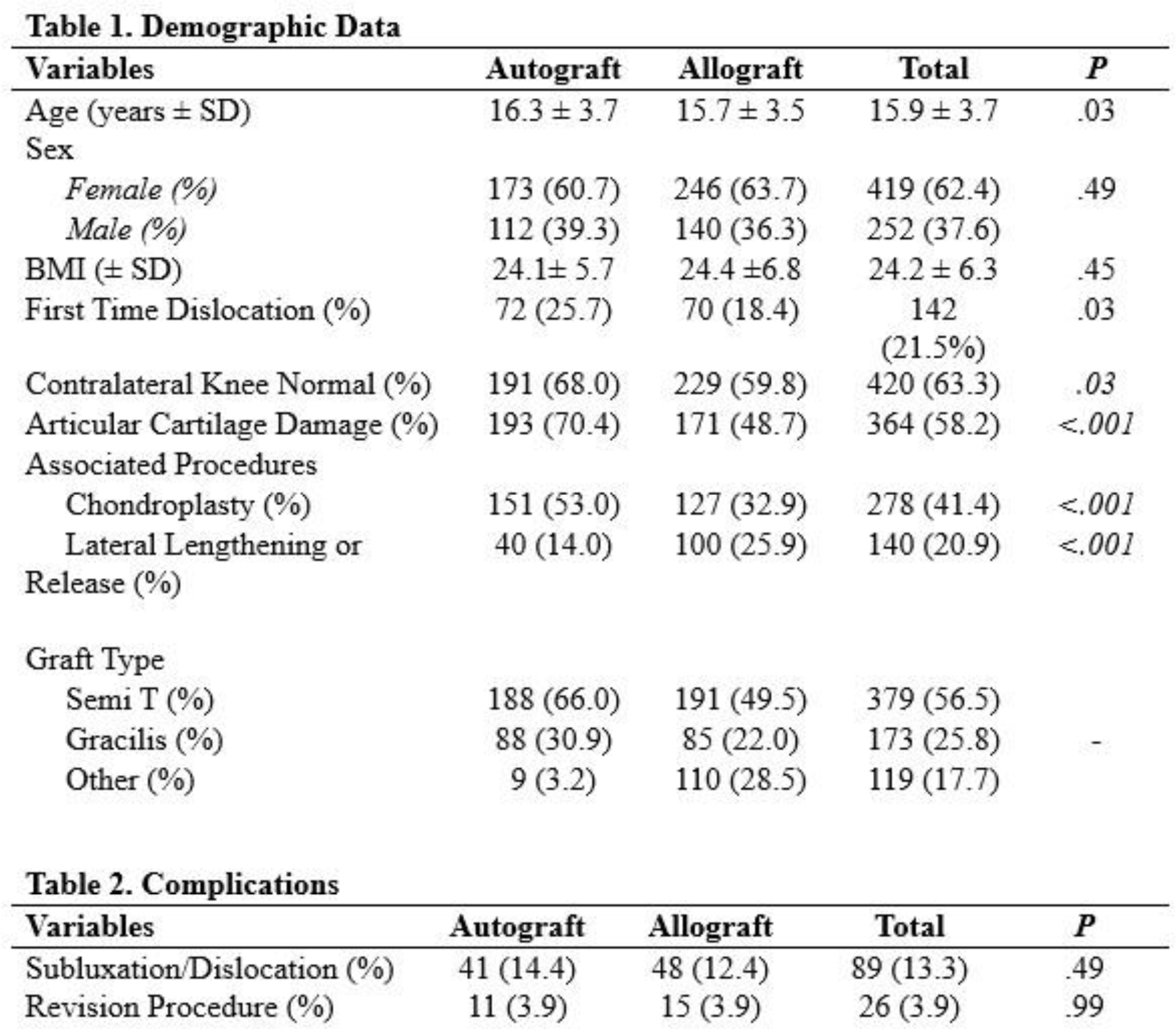
671 patients were included in this study, 285 autograft MPFL reconstructions and 386 allograft MPFL reconstructions. Autograft patients were significantly older (16.3 ± 3.7 vs. 15.7 ± 3.5, p=0.03), more likely to have first-time dislocation (25.7% vs. 18.4%, p=0.03), with higher rates of articular cartilage damage (70.4% vs. 48.7%, p<0.001) (Table 1). Autograft patients had a significantly higher rate of concomitant chondroplasty procedures (53.0% vs. 32.9%, p<0.001), while allograft patients had a higher rate of lateral lengthening (25.9% vs. 14.0%, p<0.001). The most common autografts were semi-tendinosis (n=188) and gracilis (n=88). The most common allografts were semi-tendinosis (n=191), gracilis (n=85), tibials anterior (n=90), and peroneus longus (n=19). There was no difference in subluxation/dislocation rates or reoperation rates between the groups (Table 2). Patients treated with an autograft MPFL reconstruction had significantly better patient reported outcomes at two years (Kujala and IKDC Pedi) and 5 years (Kujala, IKDC Pedi, and KOOS Jr.) (Table 3). There were no differences in complications rates when stratified by allograft or autograft type (Table 4).
Conclusion:
Patients in this study treated with an MPFL reconstruction experienced similar complication profiles, irrespective of graft type. Patients treated with an autograft MPFL reconstruction demonstrated higher performance on patient reported outcomes measures at 2- and 5- years postoperatively.