Abstract
Background:
Numerous medial patellofemoral ligament reconstruction (MPFLR) techniques exist for patients with patellofemoral instability (PFI). Iatrogenic patella fracture from tunnel drilling remains a rare, but serious, complication from standard reconstruction techniques, especially in skeletally immature patients. This has prompted the search for alternative patellar fixation methods. We sought to evaluate outcomes of a modification of the allograft basket-weave technique originally described by Kodkani that utilizes all soft tissue fixation for a two-limbed, anatomic MPFL/MQTFL reconstruction in patients with PFI (Figure 1).
Objectives:
The modified basket-weave technique is a safe, effective, and versatile option for MPFLR in pediatric and adolescent patients with PFI.
Methods:
A retrospective review was performed identifying a consecutive series of pediatric and adolescent patients (<21 years old) treated at a single tertiary-care institution for PFI with MPFLR using the modified basket-weave technique along with any additional indicated procedures. Patient demographics, clinical presentation, patellofemoral radiographic measures (Tibial Tubercle-Trochlear Groove [TT-TG], Canton Dechamp Index [CDI], and trochlear morphology), and surgical management and early postoperative outcomes were recorded. Descriptive statistics were performed of the cohort.
Results:
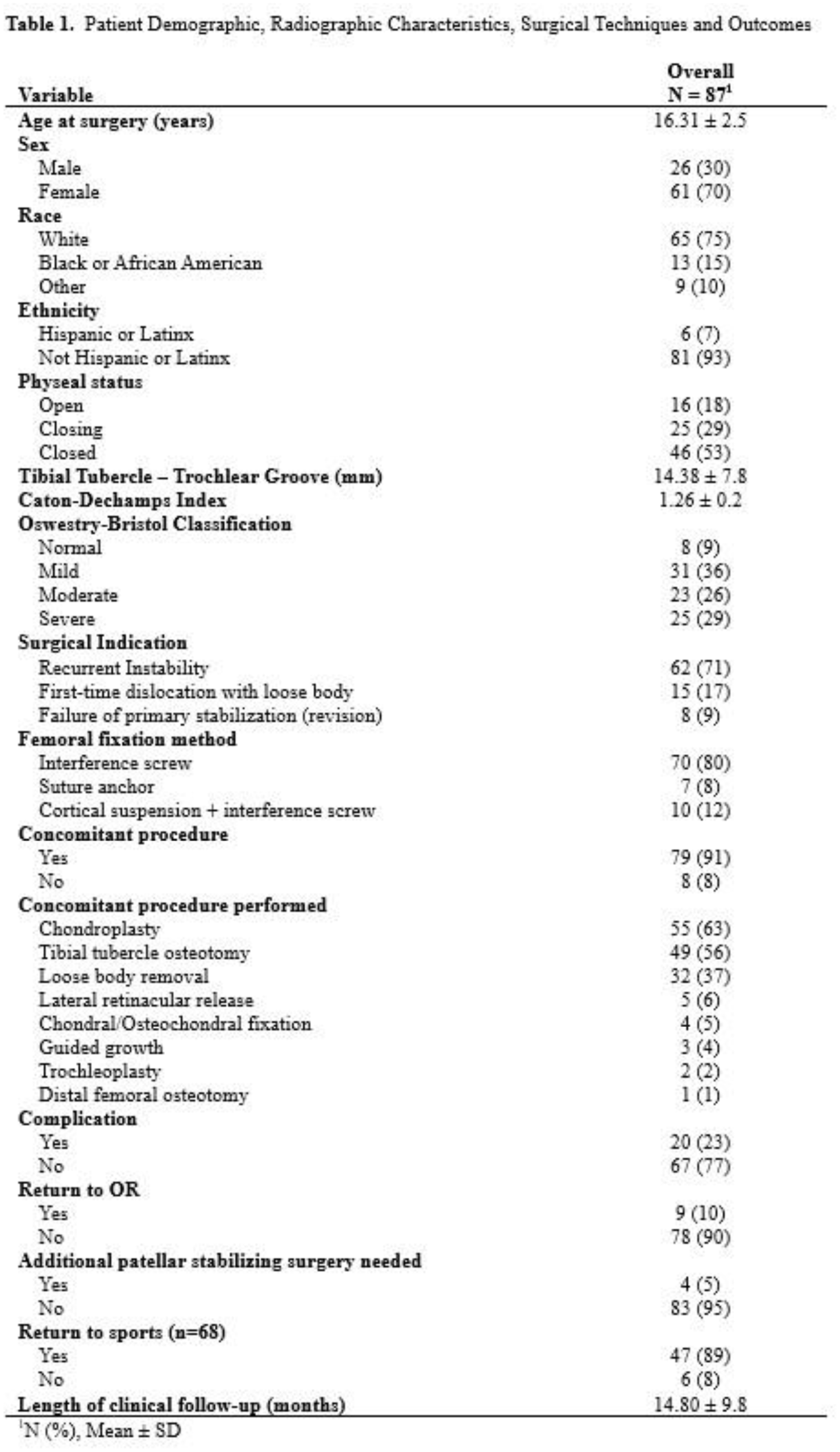
Study criteria identified 87 patients (16.31 ± 2.5 years, 70% female). Most underwent primary stabilization for recurrent PFI (71%); while 9% underwent revision MPFLR. The cohort had a mean TT-TG distance of 14.38 mm and CDI of 1.26, and 55% of patients had moderate or severe trochlear dysplasia. Femoral sided graft fixation was performed most commonly with interference screws (80%). Concomitant procedures were performed in 91% of patients, most commonly tibial tubercle osteotomy (56%). Complications observed included postoperative stiffness (n=5) and infection (n=2); however, only 5 of these patients returned to the OR for treatment. 10 patients experienced postoperative instability symptoms of any kind, but only four (5%) required revision stabilization procedures. No patellar sided graft failures, fractures, or symptomatic patellar fixation sites were observed.
Conclusion:
This large consecutive series of the modified basket-weave MPFLR technique demonstrates comparable early outcomes to other MPFLR techniques. No patellar-sided complications were observed in this cohort. This technique is also versatile and can be utilized in a variety of primary and revision patellar stabilization settings as prior patellar implants do not complicate its use. Basketweave patellar MPFLR is a safe and viable option for the surgical treatment of patellar instability in pediatric patients.