
Abstract
Patients affected by inborn errors of metabolism can develop catastrophic epilepsies ineligible for resective surgery. Few reports concerning vagal nerve stimulation in patients with epileptic encephalopathy in the context of metabolic diseases have been published in the literature. Drug-resistant epilepsies in metabolic disease could be a specific target for vagal nerve stimulation, although the efficacy of this technique in these patients still needs to be proved. The authors report our experience in treating refractory epilepsy with vagal nerve stimulation in 2 patients affected by inborn errors of metabolism. The first patient is a 23-year-old patient affected by glutaric aciduria type II, the other one is a 16-month-old child with nonketotic hyperglycinemia. Vagal nerve stimulation reduced seizures up to 50% in the first case and up to 90% in the second one.
The authors describe 2 patients affected by different metabolic diseases, who developed drug-resistant epilepsy, treated with vagal nerve stimulation: The first patient was affected by deficiency of fatty acid β-oxidation (glutaric aciduria type II), and the other one presented with deficit in glycine metabolism (nonketotic hyperglycinemia).
Glutaric Aciduria Type II
Glutaric aciduria type II or multiple acyl-CoA dehydrogenase deficiency is an autosomal recessive disease due to a deficiency of electron transfer flavoprotein genes (ETFA and ETFB) or electron transfer flavoprotein dehydrogenase gene. The disease mainly impairs the activity of acyl-CoA dehydrogenases in fatty acid β-oxidation.
Glutaric aciduria type II can occur in neonatal, juvenile, adolescent, and adult form. The first one is the most severe form: The complete deficiency causes severe metabolic acidosis without ketosis, coma, hypoglycemia, hyperammonemia, hypotonia, cardiomyopathy, and sometimes congenital malformations such as polycystic kidneys and dysmorphic facies. 1
Nonketotic Hyperglycinemia
Nonketotic hyperglycinemia is an autosomal recessive inborn error of metabolism of amino acid caused by a lack in glycine cleavage system presenting with increased levels of glycine in blood, urine, and cerebrospinal fluid. The onset is usually neonatal or during early infancy, and the common symptoms are severe hypotonia, erratic seizures—mainly myoclonic—and lethargy. The natural history of the disease leads to severe mental retardation and drug-resistant epileptic encephalopathy. The electroencephalogram (EEG) shows a characteristic pattern called “bursts suppression.” Epilepsy in children with nonketotic hyperglycinemia is frequently intractable. 2 –4
Although vagal nerve stimulation is effective against drug-resistant epilepsies, only few reports deal with the treatment of epileptic encephalopathies in patients with inborn errors of metabolism. Prasad and colleagues 5 reported a girl affected by methylenetetrahydrofolate reductase deficiency who underwent vagal nerve implantation with questionable benefit. Tsao 6 demonstrated the vagal nerve stimulation efficacy in reducing frequency and duration of seizures in 2 children with refractory epilepsy associated with nonketotic hyperglycinemia.
Arthur and colleagues 7 retrospectively investigated the outcome in 5 children affected by mitochondrial electron transport chain deficiencies, who underwent vagal nerve stimulation, concluding that vagal nerve stimulation cannot be an effective method to control seizures in these patients. No case of vagal nerve stimulation in patients with glutaric aciduria type II is reported in the literature.
Methods
Among the patients followed at the Centre for Rare Metabolic Diseases of our Hospital, 2 patients were selected because of drug-resistant epilepsy. Several video-EEG recordings were performed before and after the vagal nerve stimulation implant to study the bioelectrical activity and its changes during the follow-up. After parental consent, patients underwent vagal nerve stimulation (Cyberonics Model 103, Cyberonic Inc, Houston, TX, USA) implantation. Surgery was performed as a standard procedure, under general anesthesia. The parents filled a daily diary in reporting frequency and intensity of seizures. All the data were collected to score the outcomes, comparing the pre- and postimplant period, using McHugh et al scale. 8 This scale evaluates both the frequency of the seizures and the intensity of the postictal period, compared to the preimplant baseline, and all stimulation parameters (current, cycle, and impedance) were recorded every outpatient visit.
All procedures were in accordance with the ethical standards of the Committee on Human Experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Written informed consent was obtained from the patient, if the case, and parents, before included in the study. The authors did not request the approbation of our ethics statement because this was not needed.
Results
Case Study 1
The patient had glutaric aciduria type II due to electron transfer flavoprotein α deficiency with neonatal onset. He had a normal growth and a normal psychomotor development until the age of 5 months, and he was treated with low-fat diet avoiding fasting and with riboflavin and carnitine intake as recommended in glutaric aciduria type II. Epilepsy occurred at the age of 5 months, presenting with drug-resistant epileptic spasms. Other seizures, both generalized and focal, occurred in the following years, and finally, he developed a first generalized status epilepticus at the age of 6 years. Despite several mono- and polytherapies (carbamazepine, vigabatrin, clobazam, phenobarbital, leviteracetam, nitrazepam, lacosamide, rufinamide, acetazolamide, and Hemp Oil), the seizures worsened over the years. Since the age of 15 years, the neurological status and quality of life worsened, and the patient showed progressive mental and motor impairment till spastic tetraparesis. He developed generalized seizures (Figure 1) occurring in clusters both in sleep and in awake, noise-provoked seizures, and clusters of spasms at the awakening. The postictal period became more severe. At the age of 23 years, he underwent implantation of vagal nerve stimulation. Vagal nerve stimulation was switched on 2 weeks after surgery, reaching the programmed setting in 8 weeks. The stimulation parameters were output current 1.25 mA and cycle 30 seconds ON 5 minutes OFF, and impedance was 3210 Ω.

Generalized tonic seizures during sleep.
The patient tolerated vagal nerve stimulation well, and no side effects occurred. At 1-year follow-up, the frequency of seizures decreased more than 50% (Mc Hugh score IIA), and the severity of the postictal period dropped off. Noise-provoked seizures and spasms were fully controlled by stimulation. The quality of life of the patient—and therefore of the parents—also improved, by the reset of a normal sleep–awake rhythm. Drug intake reduced from 4 to 1 (Carbamazepine 10 mg/kg/die).
Case Study 2
This child was affected by nonketotic hyperglycinemia and developed drug-resistant asymmetrical spasms and myoclonias with burst suppression EEG, immediately after birth. Treatment with sodium benzoate and dextromethorphan was started at the age of 10 days. Phenobarbital decreased the number of the seizures till to few brief asymmetrical spasms a day, 2 months along, and then, the frequency and intensity of the seizures increased until, at the age of 3 months, the patient developed status epilepticus, which required admission to pediatric intensive care unit. After discharge, the frequency of seizures was stable for 6 months. At the age of 13 months, the seizures became more frequent and longer, despite levetiracetam in add-on to previous treatment. At that time, the authors suggested the parents for vagal nerve stimulation implant, obtaining their informed consent. At the age of 16 months, he developed a novel focal refractory status epilepticus (Figure 2), which required admission to the hospital. Implantation of vagal nerve stimulation was performed during this status epilepticus.
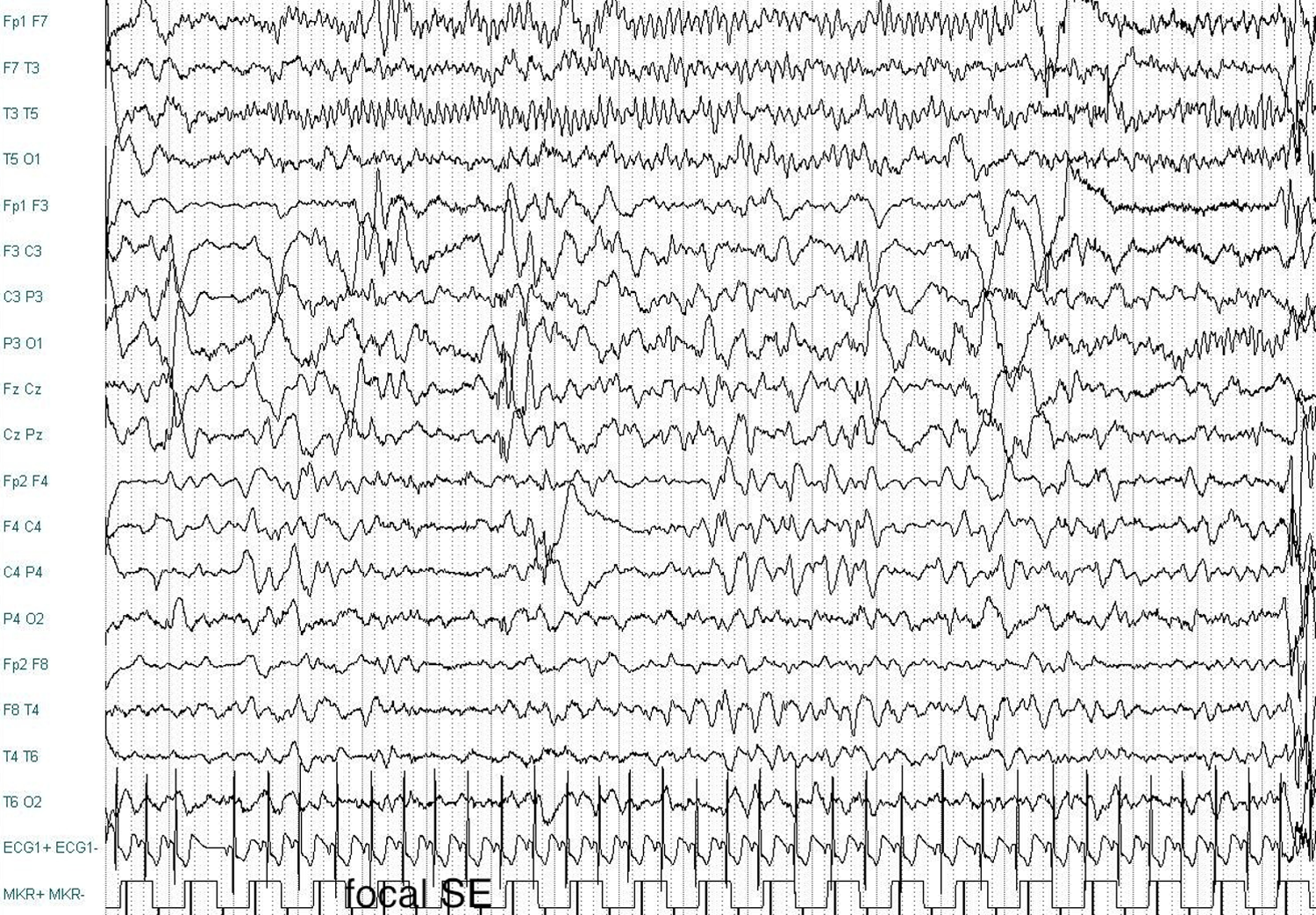
Focal status epilepticus in nonketotic hyperglycinemia.
Vagal nerve stimulation was switched on immediately after surgery, reaching the output current of 1 mA after 2 days; cycle was 30 seconds ON 5 minutes OFF, and impedance was 2489 Ω. The patient tolerated the stimulation, and no side effects occurred. After 5 days, the frequency of the seizure decreased to mean of 6 brief spasms in mean per day, and after 2 weeks, the baby was discharged home.
After 12 months follow-up, seizure frequency further dropped down more than 90%, comparing the preimplant time (McHugh score IA), and the child never developed new status epilepticus. Currently, the EEG does not reveal burst suppression pattern (Figure 3) and drugs dropped off (phenobarbital 1 mg/kg/die and levetiracetam 20 mg/kg/die).

Disappearence of burst suppression pattern after the vagal nerve stimulation implant.
Discussion
Epilepsy is not usually considered as a main symptom in the phenotype of glutaric aciduria type II. 4 Angle and Burton 9 reported the occurrence of life-threatening events in 3 patients with glutaric aciduria type II, occurring in 1 case with partial seizures. Our patient developed a catastrophic drug-resistant epilepsy, resulting in severe cognitive and neurological impairments. The vagal nerve stimulation implant at the age of 23 years obtained reduction in the frequency of seizures (McHugh class 2A) and improvement in the quality of life, due to the decrease in the major seizures during sleep and alertness and to the restriction of the postictal period. Although the correlation between age of the implant and effects of the vagal nerve stimulation is not thoroughly clarified, 10 moreover, it is well known that this time lapse can play an important role: In our case, the delay of 22 years from the onset of the epileptic encephalopathy might have impinged upon the results of vagal nerve stimulation.
Drug-resistant epilepsy is a major feature in the phenotype of nonketotic hyperglycinemia. 11 The natural history of 65 patients with nonketotic hyperglycinemia scored a prevalence of 62 of 65 of epilepsy, and only 25 of 65 patients survived more than 3 years. There are different types of nonketotic hyperglycinemia, all without an effective therapy. Epilepsy in case of nonketotic hyperglycinemia occurs in the neonatal period usually in the form of early myoclonic encephalopathy, 3 a particular kind of severe newborn encephalopathy first described by Aicardi and Goutieres. 12 The natural history of early myoclonic encephalopathy during the lifetime of the patients with nonketotic hyperglycinemia or other diseases progresses to various forms of epileptic drug-resistant encephalopathies, and the quality of the cognitive and motor development can depend on frequency and intensity of seizures. 4 Few data in the literature suggest the efficacy of vagal nerve stimulation in case of refractory epilepsy in patients with disorders of amino acid metabolism. Tsao 6 reported 2 cases of patients having nonketotic hyperglycinemia with refractory epilepsy in whom implantation of vagal nerve stimulation reduced the frequency and severity of seizures. The first case was implanted at the age of 6 years, reducing the seizures frequency more than 75% few months after surgery. The second case, implanted at the age of 21 months, became seizure free, tapering all the anticonvulsant at the age of 3.5 years. The output current was 2 mA and 1.75 mA, respectively, with a Duty Cycle of 10%. In agreement with results of Tsao, our case suggests that, in patients with drug-resistant epilepsy due to nonketotic hyperglycinemia encephalopathy, vagal nerve stimulation might reduce frequency, duration, and severity of the seizures and, as a result, improve the quality of life. Unlike the cases by Tsao, the authors implanted our patient with nonketotic hyperglycinemia during a refractory status epilepticus, achieving a reduction down to 90% of the seizures frequency, few days after surgery. Vagal nerve stimulation implant can be useful to stop a status epilepticus and to prevent the recurrence of a new status epilepticus. 13,14
In our patient, epilepsy control endured over 12 months of follow-up without changing vagal nerve stimulation parameters, and the output current was lower than reported by Tsao 6 : This is in agreement with DeGiorgio and collegues 15 who, reviewing all parameters of stimulation in a sample of 154 patients, accomplished that high current does not correlate with better clinical results.
The mechanism of action of vagal nerve stimulation in human epilepsy remains unknown. Zabara 16 found that repetitive electrical stimulation of the canine cervical vagal nerve can inhibit strychnine-induced motor seizures and tremors induced by pentylenetetrazol, while Woodbury and collegues 17 reported that vagal nerve stimulation inhibition of chemically induced seizures in rats is due to activation of gamma aminobutyric acid (GABA) and glycine pathways in the brain stem and cerebral cortex. De Herdt and colleagues, 18 investigating cortical excitability during vagal nerve stimulation, verified the increased seizure threshold in an animal model for motor seizures.
These experimental findings confirm the efficacy of vagal nerve stimulation in motor partial seizures in animal models. Since no experimental data are available from humans, it can be speculated that vagal nerve stimulation might induce a fast-acting GABAergic or glycine-dependent mechanism, able to raise the cortical excitability threshold. A fast-acting mechanism like this might explain the precocious effect obtained by vagal nerve stimulation in epileptic status, independent of its origin. Further investigations are required in humans to confirm this suggestion.
Conclusion
Vagal nerve stimulation was effective to treat refractory epilepsy in patients with inborn errors of metabolism. Frequency, intensity, and severity of seizures decreased in a variable time, from few days to some months, together with an improvement in quality of life for children and their parents. Our patients well tolerated the vagal nerve stimulation, and no side effects occurred after surgery nor during follow-up. It is remarkable that no novel status epilepticus occurred after implant of vagal nerve stimulation. Our data suggest that vagal nerve stimulation might be successfully used in patients with epileptic encephalopathy affected by inborn errors of metabolism but need to be confirmed by further studies on a larger number of patients.
Footnotes
Acknowledgments
RP, SG, and MR gratefully thank Fondazione Pierfranco and Luisa Mariani of Milano for providing financial support for clinical assistance to metabolic patients. The neurosurgery and clinical work were completely done in San Gerardo Hospital. All the authors thank the technicians N. Zorzan and A. Cepele for their work.
Author Contributions
DG is the first author because he wrote the first draft of the manuscript, he cared for the patients, and analyzed the data. AL, AT, and LF were equal and essentially constituted the majority of the work by organizing neurosurgery. EPS is a mentor who equally provided the support and mentorship necessary for the success of the work. SG, MR, and RP took care of the patients in Metabolic Unit and supported the families. All the authors gave their contribution equally to clinical study and to reviewed this article.
Authors’ Note
All the authors declare the absence of previous similar or simultaneous publications, their inspections of the manuscript, their substantial contribution to the work, and their agreement to submission. Vagal nerve stimulation proved to be successful in 2 patients with epileptic encephalopathy due to inborn errors of metabolism.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Authors did not need funding because this is not a study but only a clinical report of two patient in which we performed vagal nerve stimulation for clinical necessity.
Ethical Approval
Written informed consent was obtained from all patients or their parents before surgery. We did not request the approbation of our ethics statement because this is not needed for clinical use.