
Abstract
Atypically developing children including those born preterm or who have autism spectrum disorder can display difficulties with evaluating rewarding stimuli, which may result from impaired maturation of reward and cognitive control brain regions. During functional magnetic resonance imaging, 58 typically and atypically developing children (6-12 years) participated in a set-shifting task that included the presentation of monetary reward stimuli. In typically developing children, reward stimuli were associated with age-related increases in activation in cognitive control centers, with weaker changes in reward regions. In atypically developing children, no age-related changes were evident. Maturational disturbances in the frontostriatal regions during atypical development may underlie task-based differences in activation.
Frontostriatal circuitry is crucial for the development of reward centers, which are essential for learning and social interaction. Atypical development of frontostriatal pathways is commonly seen in children born preterm and those with autism spectrum disorder and may underlie social communication difficulties and deficits in evaluating rewarding stimuli.
In typical development, reward centers mature in later childhood and may underpin risk-taking behavior in early adolescence. 1-3 Cognitive control centers that mediate activity in reward systems develop later in adolescence.
Reward processing has been studied using functional magnetic resonance imaging (MRI) and recruits several brain regions such as the anterior cingulate cortex, ventromedial prefrontal cortex, orbitofrontal cortex, ventral striatum, amygdala, and portions of the midbrain. 4-6 Age-related linear increases in activation have been reported during reward anticipation in children (aged 10-25 years) and adults in the ventral striatum, dorsal caudate, putamen, insula, anterior cingulate cortex, and orbitofrontal cortex. 7 Little is known about the early development of reward processing systems in typical development; however, a functional MRI study included children as young as 8 years and reported age-related changes in the anterior cingulate cortex, ventromedial prefrontal cortex, and ventral striatum in response to reward stimuli. 3 Whether these patterns of activation are present at early ages remains to be determined.
Alterations in the development of reward-based processes can lead to overactivity in the reward system, which has been suggested to underlie restricted and repetitive behaviors in children with autism spectrum disorder. 8-10 Some social deficits seen in children with autism spectrum disorder may be attributed to altered brain reward circuitry in that it impairs their ability to assign value to social exchanges (ie, reduction in time spent on attending to faces, speech, etc). 11-14 Supporting evidence of alterations in the neural processing of social and reward-type stimuli in autism spectrum disorder has come from functional MRI studies reporting hypoactivation within the mesocorticolimbic circuitry in response to both social and monetary rewards in school-age children, adolescents, and adults with autism spectrum disorder, 8,13,15-18 indicating little developmental change with age in this population.
Affective and behavioral disturbances prevalent in children with autism spectrum disorder are also seen in children born very preterm, 19 and premature birth is a risk factor for the development of autism. 20,21 Although the underlying pathology remains unknown, it is hypothesized that a combination of perinatal and postnatal factors can lead to the disruption of the frontal lobe and striatal development in preterm-born children, which can result in some autism spectrum disorder behavioral phenotypes. Structural imaging studies have related alterations in affective behavioral processing to emotion and reward-related brain regions and their underlying white matter fiber pathways in children and adolescents born preterm. 22,23 Furthermore, behavioral studies with infants 24 and young children (2-3 years) born preterm have reported that they are impaired in their ability to associate value with stimuli perceived as rewarding by typically developing children. In a study with young children born preterm examining executive functioning, using a delayed alternation task demonstrated that preterm-born children chose unrewarded stimuli more so than term-born children, indicating that the preterm-born children were impaired in their ability to learn reward associations. 25 However, information on how preterm-born children process reward information during childhood remains unknown.
Although evidence from functional and structural neuroimaging studies has suggested abnormalities within the reward system in atypically developing children and adolescents, it is unclear how these regions mature functionally, especially in relation to cognitive control centers. The present functional MRI study addressed the development of reward and cognitive control brain regions during typical and atypical development. The participant groups included typically developing children (6-12 years) and atypically developing children (with autism spectrum disorder or born preterm) of comparable ages. Data were combined from children with autism spectrum disorder and those born preterm, as both populations exhibit deficits in reward processing that may be associated with impaired frontal–striatal development. The data from the atypically developing group were contrasted with those obtained from the typically developing group for better understanding of the development of reward-related processes. Children participated in a set-shifting task where they received positive feedback in the form of monetary reward stimuli. It was hypothesized that atypically developing children, both children with autism spectrum disorder and those born preterm, would demonstrate hypoactivation in reward centers including the medial prefrontal cortex and striatum throughout childhood, accompanied by little developmental change in cognitive control regions such as the anterior cingulate cortex and lateral prefrontal cortex.
Methods
Participants
Twenty-six children diagnosed with autism spectrum disorder were recruited through the Autism Research Unit at The Hospital for Sick Children (Toronto, Canada) and diagnosed by clinician experts supported by a research reliable Autism Diagnostic Observation Schedule–Generic 26 and Autism Diagnostic Interview–Revised. 27 The children with autism were all verbal and high functioning (IQ > 80) and were all born at term. Although the children with autism spectrum disorder were term-born, specific birth data were not collected.
Thirty-one preterm-born children were recruited through the neonatal follow-up clinic at The Hospital for Sick Children. All children were born at <32/40 weeks’ gestational age (mean = 27.4 weeks) and had no significant brain injury detected or significant medical difficulties during the neonatal period. The Autism Diagnostic Observation Schedule and Autism Diagnostic Interview–Revised were not administered to the children born preterm.
A total of 34 typically developing children were recruited for the study (19 males, 15 females; mean age: 9.57 ± 1.87 years; range = 6.39-12.75 years). Children were screened for developmental delay and were all term-born (>37 weeks’ gestation).
Any children with learning disabilities or neurological or medical disorders (other than autism spectrum disorder) were not included; none of the children were taking medication and had sensory and/or motor dysfunction or standard contraindications for MRI. The study was approved by the research ethics board of Hospital for Sick Children, and written informed consent was obtained from parents and informed assent from the children.
Behavioral Assessments
Cognitive ability (IQ) was measured using the Full-4 Wechsler Abbreviated Scale of Intelligence 28 for all participants except 1 from the autism spectrum disorder group who had received a recent assessment using the Wechsler Intelligence Scale for Children IV.
Experimental Task
Prior to the scanning session, participants were familiarized with the experimental task and stimuli. Children performed several practice trial sets until they demonstrated that they understood the task. The stimulation protocol required a 2-alternative forced choice between compound stimuli of 2 dimensions (dimension 1: color of clown fish, dimension 2: type of aquatic plant; Figure 1A). Colorful fish and plant stimuli were designed to engage the children to ensure adequate task performance.

A, Before each scanning run, participants were shown all possible targets, each lasting 1 second. B, Stimulation protocol. A fixation cross was presented for 20 seconds followed by an explicit instructional cue that was presented for 1 second. A trial stimulus followed the cue, which showed 2 compound stimuli on either side of the screen. The task was to select which image included the target stimulus by pressing a button with either their right or left index finger, corresponding with the left or right side of the screen. Trials were repeated 3 to 4 times, until a new target stimulus was presented (set shift). After each trial, the participant was given feedback on whether they were correct or incorrect, by means of a gold coin (correct) or an X (incorrect). The participants were periodically informed on the total gold coins accumulated in their piggy bank, which was used as the primary reward stimulus.
The participants viewed the stimuli through magnetic resonance-compatible liquid crystal display (LCD) goggles. Children’s responses were recorded via 2 keypads, placed under the right and left index fingers, respectively, and connected to a computer running Presentation software (Neurobehavioral Systems, Berkeley, California).
At the start of each scanning run, children were shown all possible targets (ie, yellow fish in front of a tall green plant; Figure 1A), each lasting 1 second, with a string of “X”s above to represent the text that would later appear to indicate the target. This was followed by a fixation cross for 20 seconds followed by an explicit instructional cue that was presented for 1 second. The instructional cue was an image of the target stimulus that depicted a particular exemplar from one of the dimensions (eg, blue fish). A trial stimulus followed the cue, which consisted of 2 compound stimuli (eg, left: blue fish in front of a plant; right: a red fish in front of a plant; Figure 1B), 1 on either side of the screen. The task was to indicate the compound stimulus (ie, blue fish in front of a plant) that included the target stimulus by pressing 1 of 2 buttons with their left or right index finger, which corresponded to the respective sides of the screen. During a set of trials, the fish and plant stimuli were be presented 3 to 4 times with the right or left location of the target varying randomly.
The relevant dimension of the target stimulus (eg, blue fish or tall green plants) always appeared in the foreground for a set of trials. The session comprised 3 scanning runs of 10 sets that contained 3 to 4 trials. Each trial lasted 3 seconds, including a blank screen buffer if the child responded before the 3 seconds had elapsed. If the child did not respond, the trial was considered incorrect.
Each trial was followed by feedback that informed the child whether the response was correct or incorrect, by means of a gold coin (correct) or an X (incorrect). Once the child responded consistently to the cue (3 or 4 consecutive correct responses), either an intradimensional or an extradimensional shift of the stimuli occurred; the intradimensional or extradimensional shifts were randomly assigned. An intradimensional shift involved a 1-dimensional change in the target stimulus (eg, from blue fish target to yellow fish target). An extradimensional shift meant a multidimensional change in the target stimulus (eg, from blue fish target to green plant target). Each time a shift occurred, the participant was shown a new cue, which gave them the new target stimulus. Participants were periodically given an update on the total accumulated number of gold coins in their “piggy bank” that was used as the primary reward stimulus in the analysis. The piggy bank was presented a maximum of 6 times during a single scanning run.
Magnetic Resonance Imaging Data Acquisition
Participants underwent functional neuroimaging at the research-dedicated MRI suite at The Hospital for Sick Children. Participants were scanned on a 1.5-T MRI scanner (GE Signa Excite, Waukesha, Wisconsin), using an 8-channel array head coil. Anatomical images were obtained using a 3-dimensional fast spoiled gradient echo (FSPGR) sequence, producing volumes of T1-weighted axial slices with voxels = 0.9375 mm × 0.9375 mm, slice thickness of 1.5 mm, repetition time (TR) = 9 milliseconds. Following the anatomical sequences, children completed 3 functional scanning runs using a 2-dimensional spiral in/out sequence, producing 183 volumes of T2*-weighted axial slices, with voxels of 3.75 mm × 3.75 mm, a slice thickness of 5 mm, TR = 2 seconds, and lasted a total duration of 6 minutes.
Functional MRI Data Preprocessing and Statistical Analysis
Standard preprocessing included skull stripping the anatomical images followed by linear registration to a template in the standardized space of the Montreal Neurological Institute. 29 Three volumes at the beginning of each functional run were excluded from the analysis, allowing for the blood oxygen level dependent (BOLD) signal to achieve an equilibration state. Functional images were then motion and slice time corrected, aligned to individual anatomical images, and spatially smoothed at 10 mm FWHM (full width at half maximum) using a Gaussian blurring kernel and scaled to percentage change.
Postprocessing of functional MRI data was achieved using Analysis of Functional NeuroImages software (version 2011_12_21_1014). Data were analyzed using an event-related design, whereby each time period that contained the reward stimulus (piggy bank) was modeled as a regressor. The event-related protocol was operationalized to be the piggy bank time image shown 3 to 6 times within the scanning run (variable depending on task performance; maximum of 6 piggy banks × 3 scanning runs = 18 stimuli). All other events (including unsuccessful trials) were modeled as baseline in the analysis.
Regressors were convolved with a canonical hemodynamic response function and modeled using a gamma variate function. A general linear model was computed, and the overall model fit was assessed using an F statistic. An analysis of covariance was used for the group by age analysis. For each subject, a general linear model was computed, and the overall model fit was assessed using an F statistic. Group activations (random-effects analysis) were thresholded at P < .001 (uncorrected for multiple comparisons) using a cluster size of 5 voxels. Coordinates of loci of activation are given in Montreal Neurological Institute space. 29
Results
Participants
Of the 57 children with autism spectrum disorder and children born preterm tested, 29 of them successfully completed all 3 scanning runs (16 autism spectrum disorder, 13 preterm-born, 21 males, and 8 females, with a mean age of 9.66 ± 1.91 years; age range = 6-12 years; Table 1). Eleven children were unable to complete the task or lie still in the scanner for the functional MRI experiment, and data from a further 17 children were removed due to excessive head motion (>2 mm) during the scans.
Demographic and Clinical Characteristics of the Participant Sample.
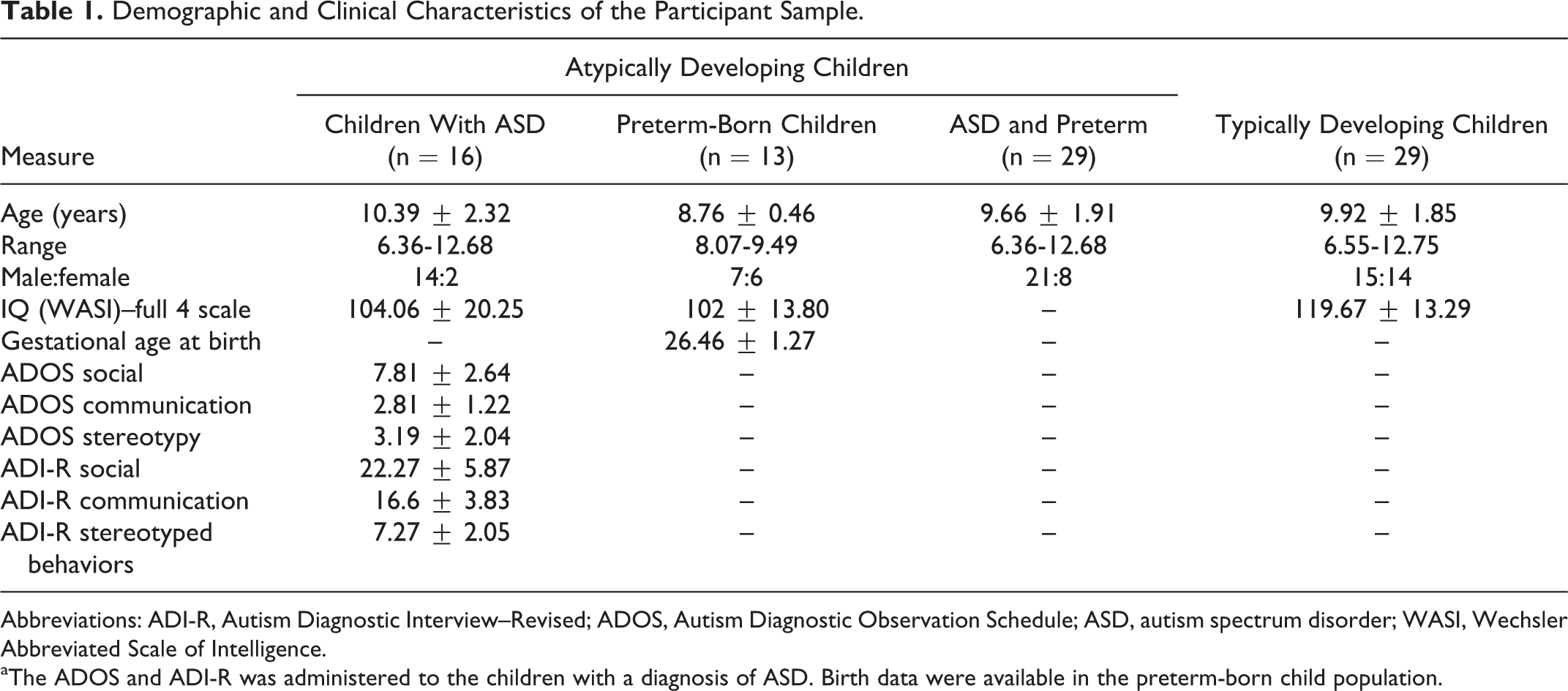
Abbreviations: ADI-R, Autism Diagnostic Interview–Revised; ADOS, Autism Diagnostic Observation Schedule; ASD, autism spectrum disorder; WASI, Wechsler Abbreviated Scale of Intelligence.
aThe ADOS and ADI-R was administered to the children with a diagnosis of ASD. Birth data were available in the preterm-born child population.
Data from 29 typically developing children were selected to be age-matched to the atypically developing population. The final data set of typically developing children who successfully completed the task was obtained from 14 females and 15 males (mean age = 9.92 ± 1.85 years, range = 6.55-12.75 years ). Thus, the total data set included 58 children, 29 per group.
Behavioral Data
All participants included in the analyses completed the task with high accuracy, with no significant differences evident between groups (P = .52). The typically developing children correctly answered 92.7% of trials, and the autism spectrum disorder group also answered the majority of trials correctly (91%) as did the group of children born preterm (92%). Given that the behavioral performance was comparable between the experimental groups, and the hypotheses regarding the brain imaging was the same for atypically developing groups of children (autism spectrum disorder and preterm), the subsequent functional MRI data were combined for these participants.
Functional Neuroimaging Data
Typically developing children
Typically developing children showed age-related effects in response to the reward stimuli in a whole brain analysis in the right inferior frontal gyrus, right middle frontal gyrus, bilateral cingulate gyri, left insula, and putamen. The full list of clusters and corresponding Montreal Neurological Institute coordinates are shown in Table 2. Comparable results were found when controlling for IQ.
Within-Group Analysis: Age Effects Associated With Reward Stimuli in Typically Developing Children.

Abbreviations: L, left; R, right.
aWithin-group analysis (typically developing children): Age-related activation in response to viewing rewarding stimuli. Coordinates are listed in MNI space (Montreal Neurological Institute space, Collins et al 29 ). Medial–lateral (X), anterior–posterior (Y), and superior–inferior (Z) stereotaxic coordinates (mm) are relative to midline (positive values are right, anterior, and superior). Results are based on a random-effects analysis.
Atypically developing children
The whole brain analysis in the atypically developing children revealed a significant activation peak in the orbitofrontal cortex. Deactivations were found in the anterior cingulate cortex, middle cingulate cortex, and caudate; see Table 3 for a complete list of foci.
Within-Group Analysis: Age Effects Associated With Reward Stimuli in Atypically Developing Children.

Abbreviations: L, left; R, right.
aWithin-group analysis (atypically developing children): Age-related activation in response to viewing rewarding stimuli. Coordinates are listed in MNI space (Montreal Neurological Institute space, Collins et al 29 ). Medial–lateral (X), anterior–posterior (Y), and superior–inferior (Z) stereotaxic coordinates (mm) are relative to midline (positive values are right, anterior, and superior). Results are based on a random-effects analysis.
The ROI analyses (directed search) further verified these results, revealing activation in the orbitofrontal cortex and deactivations in the anterior cingulate cortex and middle frontal gyrus. The full list of clusters from the ROI analyses is shown in Table 3. Results remained similar when including IQ as a covariate.
Typically versus atypically developing children
The whole brain analysis found significant activation, greater in the typically developing children, in the right insula, bilateral cingulate and middle frontal gyri, right medial frontal gyrus, and left precentral gyrus. The full list of activation clusters for this analysis is shown in Table 4.
Between-Group Analysis: Age Effects Associated With Reward Stimuli Between Typically Versus Atypically Developing Children.

Abbreviations: L, left; R, right.
Between-group analysis (typically vs atypically developing children): Age-related activation in response to viewing rewarding stimuli in the typically developing population relative to the atypically developing children. Coordinates are listed in MNI space (Montreal Neurological Institute space, Collins et al 29 ). Medial–lateral (X), anterior–posterior (Y), and superior–inferior (Z) stereotaxic coordinates (mm) are relative to midline (positive values are right, anterior, and superior). Results are based on a random-effects analysis.
A directed search in our a priori regions of interest (ROIs) verified significantly larger activations in the control children in the right anterior cingulate cortex and lateral middle frontal gyri. The ROI analysis of the striatum further revealed activation in the caudate. The full list of activation clusters for the ROI analysis is shown in Table 4.
The mean BOLD percentage signal change in response to the reward stimuli was extracted from the anterior cingulate cortex, medial prefrontal cortex, and lateral prefrontal cortex. The data extracted from the anterior cingulate cortex in the typically developing population showed a positive trend with age and revealed a peak in activation at 10 years of age (Figure 2). The activation extracted from the anterior cingulate cortex in the atypically developing population showed an opposite effect with BOLD signal decreased at older ages. In the lateral prefrontal cortex, the typically developing population exhibited a much greater increase in activation with age compared to the neurodevelopmental population (Figure 2). In the medial prefrontal cortex, a similar analysis that found trends of increased and decreased activation was associated with older ages in the typically and atypically developing population, respectively. Results did not change when IQ was included as a covariate.

A, A cluster of activation in the anterior cingulate cortex (ACC) peaked at ∼10 years of age in typically developing (TD) children (R 2 cubic = .112) in response to rewarding stimuli. Older atypically developing (ATD) children show a slight decrease in the ACC (R 2 cubic = .113). B, Cluster of activation in the lateral prefrontal cortex (PFC) showed a significant activation increase to reward at ∼10 years of age in TD children (R 2 linear = .12) in comparison to ATD children, who showed no age-related changes in activation (R 2 linear = .002).
Discussion
Using functional MRI, activation in brain regions involved in cognitive control and reward-based processing using monetary reward stimuli was examined in typically developing children, those with autism and those born preterm. Performance was comparable between groups; however, brain activation in response to reward stimuli differed significantly between typically and atypically developing children. In typically developing children, reward stimuli evoked increased activation in the medial prefrontal cortex, striatum, lateral prefrontal cortex, and dorsal anterior cingulate cortex, and was associated with older ages. In contrast, atypically developing children only showed activation in the orbitofrontal cortex. Activation in other reward and cognitive control centers was absent or showed no activation changes in atypically developing children across the age range. Comparable between-group behavioral performance accompanied by differential changes in activation in the prefrontal cortices suggests alterations in processing of reward stimuli.
Maturation of Cognitive Control Neural Systems
Recent functional MRI studies highlight nonlinear developmental changes in the activation of cognitive control regions. Many studies report age-related increases in frontal, parietal, temporal, striatal, and cerebellar cortices, which are thought to reflect age-related integration of control systems. 30,31
A developmental functional MRI study of sustained attention in a continuous performance task in a large sample of 70 children and adults (ages: 10-43 years) showed that progressively stronger recruitment of the ventrolateral prefrontal cortex, superior temporal, and inferior parietal cortices was evident with age, despite comparable task performance. 32 Another recent functional MRI developmental study using a go/no-go task found an increased engagement of the prefrontal cortex, striatum, and thalamus throughout adolescence (11-17 years) to adulthood (18-37 years). 33 Other studies have reported differential time courses of activation during cognitive control studies. 34 A meta-analysis of cognitive studies with children and adolescents (6-17 years) reported consistent activation of the inferior frontal cortex and the dorsolateral prefrontal cortex (DLPFC). However, the anterior insula was more active in adolescents relative to children, which the authors interpreted as reflecting increased cognitive control.
Previous results suggest that activity in cognitive control regions may become more specialized and integrated during adolescence. Extending these results, in the current study, atypically developing children demonstrated increased activation in the frontal and parietal regions. Weaker activation increases were noted in the striatum and the medial prefrontal cortex. However, the cingulate cortex showed a peak at ∼10 years of age followed by a slight decrease in activation at older ages, suggesting some task-specific specialization of function of the cingulate in middle childhood.
In the atypically developing population, brain regions subserving cognitive control functions showed a lack of increased activation at older ages. Other developmental functional MRI studies with children having autism spectrum disorder have also reported unchanged age-dependent activation during recognition of emotions in others 35 or during an inhibition task. 36 Additionally, studies of cognitive control with preterm-born children and young adults reported decreases in BOLD signal in task-relevant brain regions. 37,38 Findings are believed to be reflective of delayed or impaired maturation of frontostriatal systems 39-41 in these populations.
Development of Reward Systems and Modulation by Motivation Control
The orbitofrontal cortex, medial prefrontal cortex, and ventral striatum are crucial for reward-related decision-making processes. However, developmental changes in reward systems have been reported inconsistently in the functional MRI literature. Enhanced orbitofrontal cortex activation was reported in children aged 9 to 11 years and adolescents aged 13 to 17 years relative to adults aged 23 to 29 years, 2 despite no between-group differences in performance. The ventral striatum, however, demonstrated heightened activity in adolescents only, relative to adults and children during reward outcome. 1,2 The authors have suggested that the activation in the striatum in adolescents may reflect an increased sensitivity to rewards in adolescence, related to their higher risk-taking behaviors. 1-3
These findings are further supported by evidence suggesting that reward incentives enhance brain activity in typically developing adolescents compared to children and adults. 42 Activity was modulated by the magnitude of the reward in adolescents only in the inferior parietal cortex, basal ganglia, and ventral striatum. In the current study, weak positive changes were seen in reward-processing brain regions in typically developing controls in preadolescence. However, increased activation at older ages was only seen in the orbitofrontal cortex in the atypically developing population. The orbitofrontal cortex has been implicated in motivational aspects of reward processing, especially in relation to saliency and magnitude of reward. 43,44 Furthermore, in the context of reward paradigms, the orbitofrontal cortex is thought to signal executive functions and to inform goal-directed behavior through its connections with the basal ganglia. 45 Atypically developing children may recruit the orbitofrontal cortex progressively with age in reward-based tasks indexing greater difficulty with assessing saliency of the reward stimuli. Future studies with larger samples are required to validate the role of the orbitofrontal cortex in reward processes. Furthermore, research is needed to better understand sex-based differences in the developmental time courses of activation in central reward regions.
Conclusions
During development, forming reward representations is key to adaptive behavior and learning. Atypically developing children are often impaired in these abilities. In this study, functional activation in reward and cognitive control centers was examined in response to rewarding stimuli in typically and atypically developing children (aged 6-12 years). While performance was comparable between groups, increases and decreases in activation differed significantly, particularly in the frontal lobes. In comparison to typically developing children, children with atypical development showed little activation changes except in the orbitofrontal, which is involved in motivational aspects of reward processing. Activation changes in the orbitofrontal cortex in atypically developing children may indicate a reliance on motivational systems to perform the task. The lack of activation changes at older ages in other reward and cognitive control centers seen in atypically developing children may reflect disturbances in functional maturation of these prefrontal regions, consistent with the frequent deficits in social and reward situations in these children. 8,19
Footnotes
Acknowledgments
The authors would like to thank Ben Morgan for aiding in the processing of the data and Wayne Lee for MRI technical and analysis support. The authors also sincerely thank the children and their families who participated in this study.
Author Contributions
EGD, ML, and SC analyzed the data. EGD, ML, SC, JS, and MJT wrote the manuscript. KMF and MJT designed the task. KMF acquired the data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Canadian Institutes of Health Research provided the funding for this research (MOP-81161 to MJT).
Ethical Approval
Written informed consent was obtained from parents and informed assent from the children.