
Abstract
This study presents a case of a 15-year-old boy who had a right vertebral artery dissection with distal embolization from repeated trauma from an occipital bony spicule. The authors hypothesize that this bony spicule was contacting the left vertebral artery during head rotation, resulting in trauma to the vessel and formation of emboli which then showered distally, causing strokes in the posterior circulation of the brain. This specific phenomenon has previously been reported three times, only one of which was in pediatric literature. It is important for individuals to be aware of this rare anatomic cause of vertebral artery dissection in patients presenting with an odd constellation of symptoms related to strokes from vertebro-basilar system. Treatment options including early intervention with intravascular coil embolization are also discussed.
Background
Vertebral artery dissection is a rare phenomenon in the pediatric population, and most reported cases involve overt traumatic injury. We present the case of a 15-year-old male presenting with a constellation of neurologic symptoms suggesting strokes in the vertebrobasilar system. The patient was ultimately found to have an anomalous occipital condyle bony spicule, and the authors hypothesize that this bony anomaly repeatedly traumatized his left vertebral artery, resulting in vertebral artery dissection and distal embolization. To the authors’ knowledge, this is the second reported pediatric case of stroke symptoms and vertebral artery dissection in the setting of an occipital bony spicule.
Case Report
History and Presentation
This 15-year-old male had experienced symptoms for 3 weeks prior to admission, which were initially limited to persistent bilateral frontal headaches. Two weeks before presentation, he began to complain of peripheral vision loss in his left eye, which at one point became bilateral then returned again to just left-sided visual field deficits. His symptoms again worsened in the 4 days leading up to admission, when he began to complain of increased headache severity, along with new ataxia, left-sided hemiparesthesias, and worsening vision loss. His speech became rambling and incoherent, and he was generally sleepy. On the day he was admitted, all of his symptoms were at their peak severity.
Physical Examination and Evaluation
Upon admission, the patient was sleepy but alert and oriented. His eye examination revealed decreased peripheral vision bilaterally and a lack of convergence. He reported left-sided facial numbness, and he demonstrated difficulty with finger-nose pointing and heel-to-shin on his left side. Strength was decreased in the left upper and lower extremities. Magnetic resonance imaging (MRI) revealed multiple areas of ischemic infarction throughout the posterior circulation of the brain. The lesions were seen in the left lobe of the cerebellum, the right and left occipital lobes, and thalamus bilaterally. They appeared to be of various ages, which suggested a stepwise and stuttering course of infarction. Selected MRI images are presented in Figure 1. The MRI also revealed an abnormal bony process off the left occipital condyle that appeared to be in contact with a small left vertebral artery. It was felt that the bony spicule was likely traumatizing the left vertebral artery resulting in emboli showering to areas of the brain in the posterior circulation and leading to infarctions. The MRI findings prompted magnetic resonance vascular studies with 3-dimensional reconstruction. These images showing the left vertebral artery and the occipital bony spicule are presented as Figure 2. Echocardiogram and coagulation studies were performed to rule out alternative causes of strokes, and these tests were all negative. The patient was immediately started on aspirin and placed in a cervical collar due to suspicion of vertebral artery dissection and distal embolization.

T2 weighted MRI images demonstrating ischemia in A, Right and left thalamic and subthalamic areas. B, Left cerebellar lobe. C, Right and left occipital lobes.
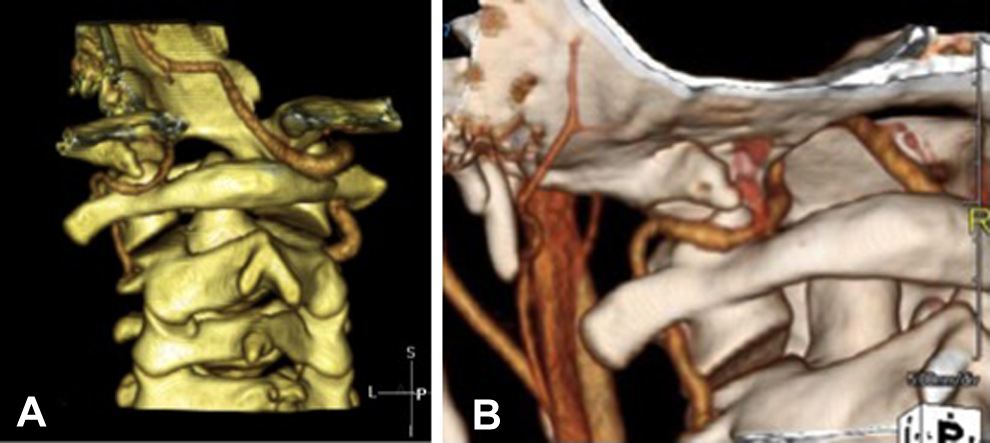
A, 3D reconstruction shows non-dominant left vertebral artery and patent right vertebral and basilar arteries. B, Close up 3D reconstruction of left vertebral artery. Occipital bony spicule is revealed in close proximity to left vertebral artery.
Hospital Course, Treatment, and Postoperative Course
Once it was decided that the bony spicule was most likely causing vertebral artery dissection and distal embolization, the decision was made to schedule diagnostic transfemoral angiography under general anesthesia with potential endovascular treatment to confirm the adequacy of collateral circulation. Preoperative angiography showing a nondominant left vertebral artery and a dominant right vertebral artery is pictured in Figure 3, along with postoperative angiography demonstrating sufficient collateral circulation. An alternative option could have been to attempt a conservative trial of anticoagulation and a cervical collar, but it was felt that the risk of further strokes outweighed the risk of the procedure. The patient underwent the endovascular occlusion of the left vertebral artery and tolerated the procedure without complication. The patient had no further strokes after his procedure. He returned to clinic 6 months after his procedure, and his only lingering deficit was homonymous hemianopia and mild blurring of his vision in his far right visual field.
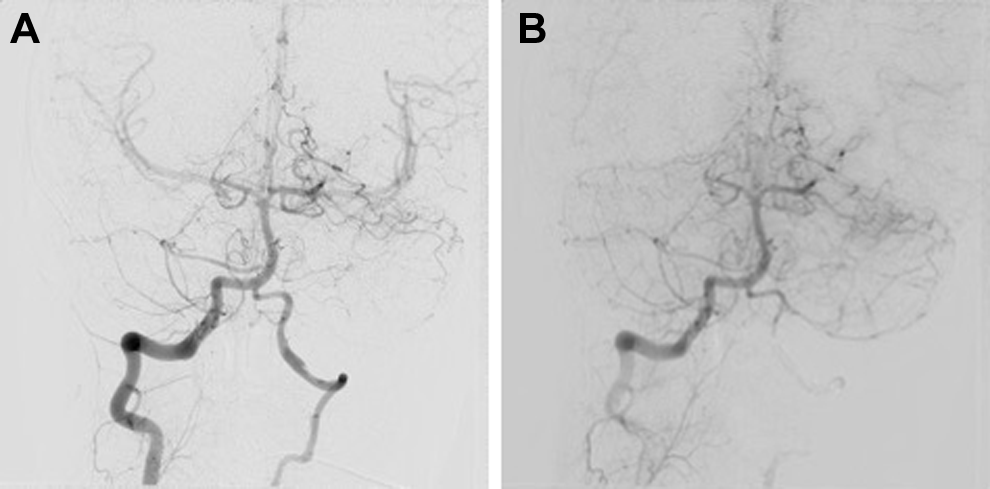
A, Pre-procedure angiography confirming patency and adequacy of collateral circulation. B, Post-embolization angiography confirming left vertebral artery occlusion and patency of right vertebral collateral circulation.
Discussion
The authors believe that in the patient, the bony occipital abnormality was repeatedly traumatizing his left vertebral artery as the spicule struck and injured the artery during rotation and extension of the head. In adult patients, there are numerous reports of rotational vertebral artery occlusion. The syndrome was first defined in 1978 and was described as “bow hunter’s stroke” due to the appearance of symptoms during head turning, as in bow hunting. 1 Extracranial vertebral artery compression has been reported to be caused by neoplasm, osteophyte formation, fibrous band growth, and trauma. 2 In adults, rotational vertebral artery occlusion is likely to manifest with transient ischemia with head turning, whereas children are far more likely to present with strokes, usually from vertebral artery dissection. 3 In children, vessel trauma is more likely to result in endothelial injury that causes distal embolization in the posterior circulation. 3,4
Vertebral artery dissections in children have been attributed to various causes such as trauma, fractures, dislocations, or unknown causes. An important subset of these causes is anatomical abnormalities. The anatomical abnormalities usually belong in 1 of the 2 groups, either cervical or occipitocranial. Cervical pathology at the level of the atlas 5,6 or below 7,8 is much more common. Table 1 is a review of the literature concerning cervical bony abnormalities and associated vertebral artery dissection, along with the presenting symptomatology and treatment of these cases. Table 2 lists the reported cases of occipital bony abnormalities, including the present case. Occipital bony spicules have been implicated as probable causes of vertebral artery dissection in 3 other instances, 10-12 1 of which was in a pediatric patient. 10
Cervical Bony Abnormalities With VAD in the Literature With Age/Sex of Patient, Presenting Symptoms, and Treatment.

Abbreviations: M, male; VAD, vertebral artery dissection.
Occipital Bony Abnormalities Resulting in VAD in the Pediatric and Adult Patients With Age/Sex of Patients, Presenting Symptoms, and Treatment.

Abbreviations: M, male; VAD, vertebral artery dissection.
In the 3 previously published cases of vertebral artery dissection and distal embolization resultant from a bony occipital growth, the treatment was a trial of anticoagulation with or without the addition of a cervical collar. In every case, anticoagulation alone proved insufficient, necessitating the need for additional intervention. Every patient went on to experience further strokes. In the adult population experiencing vertebral artery dissection, the recommendations for treatment favor anticoagulation with warfarin and/or antiplatelet therapy with aspirin, with endovascular occlusion reserved for cases of persistent aneurysmal dilation. 9 Alternatively, Cornelius et al 13 proposed a treatment algorithm that suggests relative safety and limited morbidity with decompression of the vertebral artery. In this patient, the authors found early embolization to be a successful option, and other cases have also reported using the endovascular technique successfully, although this may represent a publication bias favoring presentation of positive outcomes. 5,11,14 Similarly, positive results have been achieved with different techniques such as surgical removal of bony growths, 12 surgical decompression of the vertebral artery, 5,15-17 or even a combination of decompression and bony growth removal. 18 In the authors’ opinion, in the setting of vertebral artery dissection and strokes in a pediatric patient caused by a bony occipital anomaly, endovascular management can reasonably be considered early if it is documented that the opposite vertebral artery is patent and able to sustain the vertebrobasilar circulation. This patient experienced a positive outcome without having to remove the spicule surgically. It is clear, however, that more intense and controlled study comparing management strategies is necessary before any recommendations can be made.
Conclusion
Vertebral artery dissection and distal embolization is an uncommon phenomenon, but it is not to be overlooked in the pediatric population. The presentation of headache, ataxia, mental status changes, and/or paresthesias should prompt a high index of suspicion for vertebral artery dissection, along with further evaluation with appropriate imaging. Magnetic resonance imaging, magnetic resonance angiogram, and 3-dimensional construction can be used to look for an anatomic anomaly including occipital bony spicules. In this case, the authors believe the potential harm from additional strokes outweighed the potential complications from an endovascular deconstructive procedure, and thus the authors intervened early with endovascular occlusion.
Footnotes
Author Contributions
TB drafted the manuscript. PL and WT critically revised the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.