
Abstract
Objective:
Tuberous sclerosis complex is expressed throughout the body, resulting in a range of clinical manifestations that can be challenging to manage.
Results:
The authors report a patient who presented at age 3.5 years with several suspected seizures and was diagnosed with tuberous sclerosis complex following the discovery of numerous bilateral cortical tubers and subependymal nodules on magnetic resonance imaging. Interdisciplinary, comprehensive care was recommended; this included ongoing surveillance to monitor for the development of tuberous sclerosis complex–associated conditions. Approximately 2 years later, the patient began exhibiting aggressive and self-injurious behavior, and a subependymal giant cell astrocytoma was discovered. After everolimus was initiated, he demonstrated less aggression, had ceased self-injurious behavior, and subependymal giant cell astrocytoma growth stabilized.
Conclusions:
This case highlights the importance of a multidisciplinary approach to care in tuberous sclerosis complex, which ensures the early detection and appropriate treatment of clinical manifestations that may arise during the course of the patient’s life.
Tuberous sclerosis complex is a genetic disorder that affects approximately 1:6000 people; it is characterized by growth of nonmalignant tumors that occur in multiple organ systems, including the brain, kidneys, lungs, skin, eyes, and heart. 1 These clinical manifestations generally appear at different points throughout a patient’s lifetime (Figure 1).
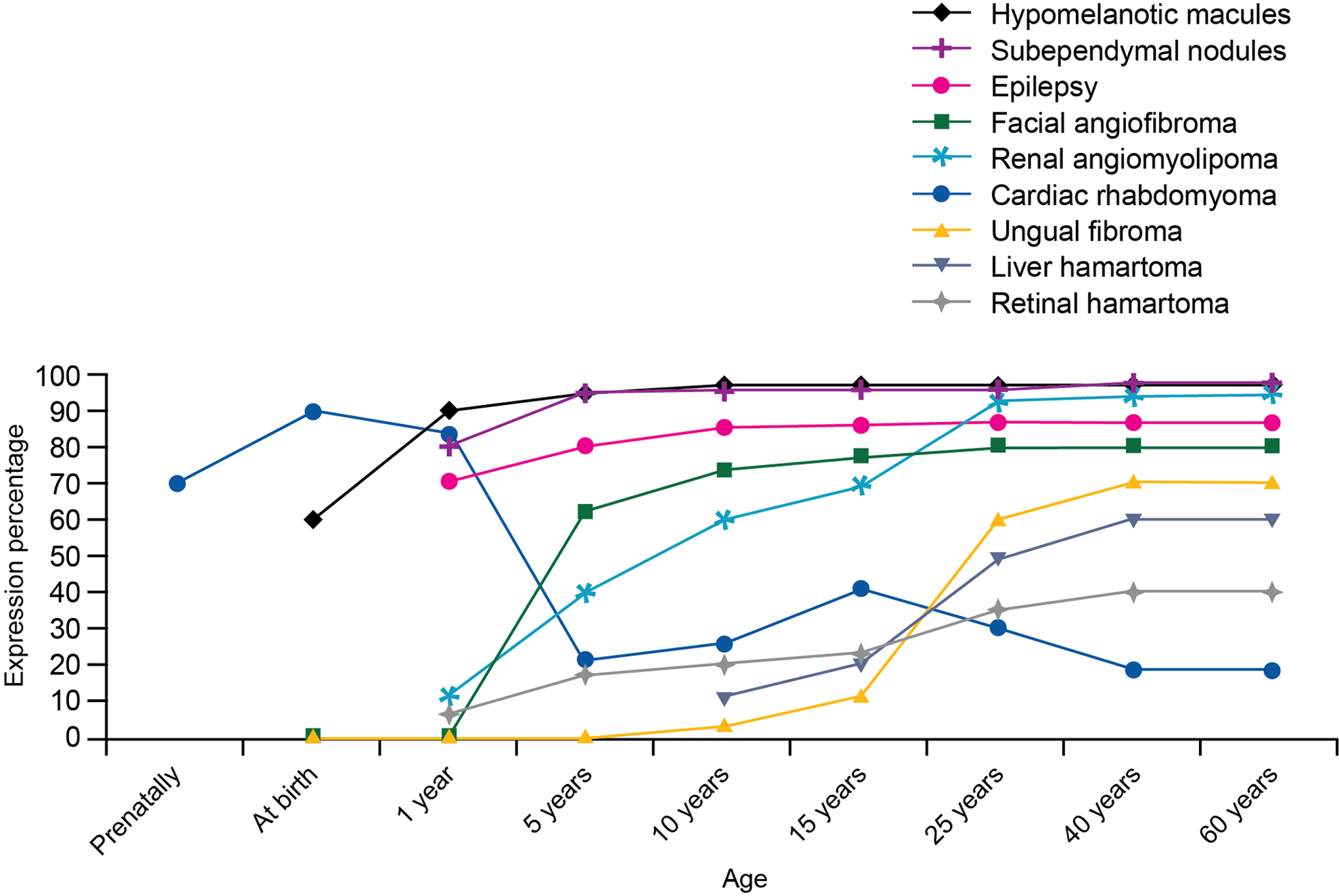
Prevalence of clinical manifestations throughout a patient’s lifetime. Reprinted from Curatolo et al. Copyright 2008 with permission from Elsevier. 1
Tuberous sclerosis complex–related lesions in the brain include cortical tubers, subependymal nodules, and slow-growing tumors known as subependymal giant cell astrocytomas; these are considered major features of tuberous sclerosis complex according to consensus guidelines. 2 In addition to brain tumors, patients with tuberous sclerosis complex can also present with various neurologic manifestations, such as seizures, cognitive disability, autism spectrum disorder, and behavioral issues. 1,3,4
Herein, the authors present a pediatric case of tuberous sclerosis complex with complex behavioral issues and highlight their approach to the management of this patient.
Patient Case
On January 5, 2012, a 3.5-year-old male child with a history of developmental delays, expressive language disorder, and autism spectrum disorder presented to the authors' clinic for evaluation of several suspected seizure spells based on reports from his mother. A physical examination revealed hypopigmented skin lesions on the right axilla, upper back, back of the neck, and back of the left upper thigh. Given the developmental delays and skin lesions, magnetic resonance imaging (MRI) was scheduled to evaluate for potential seizure foci or evidence of other seizure etiologies. An electroencephalogram (EEG) and antiepileptic therapy were also recommended, but medical treatment was deferred.
On January 8, 2012, the child was admitted to the pediatric neurology service because of increased seizure frequency. Levetiracetam (20 mg/kg intravenous bolus, then 10 mg/kg orally twice a day) was initiated, and no further seizures were observed during hospitalization. A brain MRI revealed numerous cortical tubers in the bilateral frontal, parietal, temporal, and occipital lobes. Subependymal nodules were also observed in both lateral ventricles; the largest was at the level of the right foramen of Monro measuring 6 mm × 8 mm (Figure 2A and B). These findings were consistent with a diagnosis of tuberous sclerosis complex. At this time, cardiac evaluation (echocardiogram), renal ultrasound, and ophthalmology examination were unremarkable. Upon discharge, levetiracetam and vitamin B6 were prescribed.
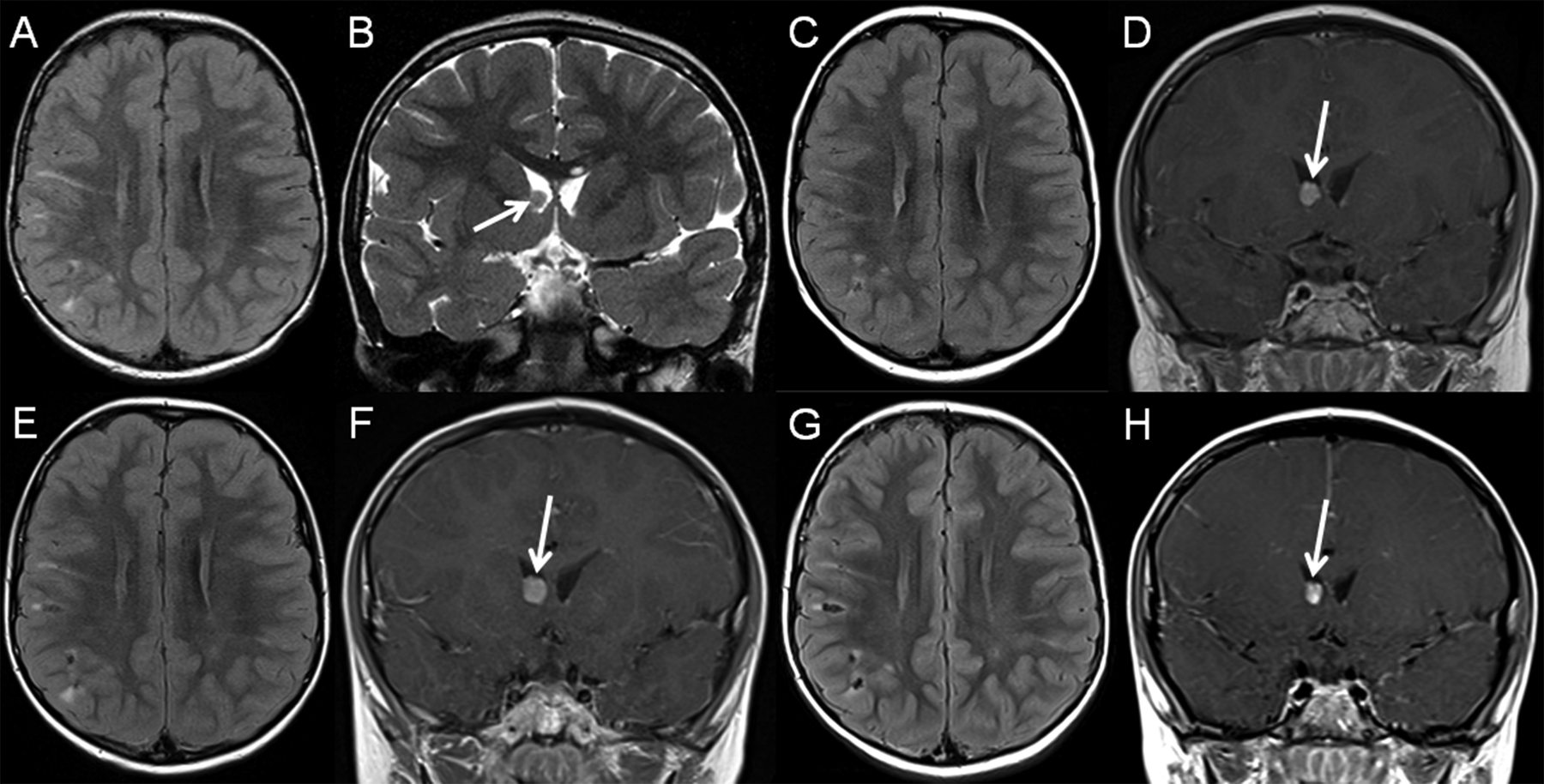
A, C, E, G, Axial fluid attenuation inversion recovery (FLAIR). B, A coronal T2-weighted image. D, F, and H, contrast-enhanced coronal T1-weighted magnetic resonance (MR) images. At the age of 3.6 years, multiple cortical/subcortical FLAIR hyperintense tubers within the bilateral frontal and parietal lobes (A) as well as a well-circumscribed, T2-isointense subependymal nodule at the level of right foramen Monro (B, arrow) are seen. At the age of 5.1 years, some of the tubers show calcifications (FLAIR hypointense, C) and there is an increase in size of the enhancing subependymal giant cell astrocytoma subependymal giant cell astrocytoma (SEGA) at the level of right foramen Monro (D, arrow). At the age of 6.1 years, unchanged cortical/subcortical tubers (E) and mild increase in size of the SEGA (F, arrow) are noted. At the age of 6.8 years, stable cortical/subcortical tubers (G) and stabilization of the SEGA (H, arrow) are seen.
At a 2-month follow-up, interdisciplinary, comprehensive care, guided by the developmental pediatrician, was recommended to monitor for the development or progression of tuberous sclerosis complex–associated conditions through regularly scheduled surveillance. The pediatrician was to guide referrals for a range of evaluations/consultations, including ophthalmology, radiology, EEGs, dermatology, neurology, neurodevelopmental disabilities specialist, speech/language, occupational therapy, psychology, and social work. Continued management of epilepsy and neurodevelopmental intervention with ongoing monitoring were also recommended.
In July 2013 (aged 5 years), MRI revealed growth of the right subependymal nodule to 7 mm × 10 mm in cross-sectional dimensions, but without ventriculomegaly (Figure 2C and D). Upon routine follow-up 1 year later (August 2014), MRI revealed slow growth of the right subependymal nodule, which was then classified as a subependymal giant cell astrocytoma (7 mm × 11 mm in cross-sectional dimensions; Figure 2E and F). Tubers remained stable over time. At the August 2014 visit, our patient (now aged 6.1 years) had been seizure-free for over 2 years, and his seizures were controlled. Oxcarbazepine and then lamotrigine were added to levetiracetam prior to this period as a result of ongoing seizures. An EEG that included sleep assessment was normal. His tuberous sclerosis complex diagnosis had been confirmed by genetic testing (TSC1 novel frameshift mutation), and neuropsychological evaluation confirmed a diagnosis of tuberous sclerosis complex–related autism. Renal, cardiac, and ophthalmologic follow-up evaluations did not reveal any tuberous sclerosis complex–related manifestations, although liver angiomyolipoma was discovered by abdominal MRI in July 2014. A dermatologic evaluation in April 2014 identified the presence of ungual/periungual fibromas (later diagnosed as verrucae vulgaris) and new hypopigmented macules on the upper right chest and lower back.
In March 2014 (aged 5.8 years), it was noted that the patient had been exhibiting aggressive and self-injurious behavior (ie, lip picking) at home and noncompliance in school since late 2013, along with increased difficulty sleeping and increased anxiety. He had been taking clonidine (∼9 months) and fluoxetine (∼6 months). Daytime clonidine had been switched to guanfacine, with an eventual dose increase in response to noncompliant behavior; he had previously been taking methylphenidate stimulant therapy, but an amphetamine alternative (dextroamphetamine) was suggested. Subsequently, in April 2014, the mother reported improvements in his behavior, with improvements on a rating scale in aggression (from 5 [moderate issues] at baseline to 1 [mild]) and noncompliance (from 8 [severe] to 2 [mild]).
Everolimus 2.5 mg/d was initiated in September 2014 (aged 6.2 years) to treat the newly diagnosed subependymal giant cell astrocytoma, with monthly laboratory monitoring (at parental request) and repeat neuroimaging scheduled for 6 to 12 months. During the first few weeks of everolimus administration, the patient experienced mouth ulcers, which were successfully managed with 1 week of everolimus dose interruption. On follow-up in November 2014, the mother noted that he was happy, had a decreased incidence of aggression, and had ceased self-injurious behavior (ie, pressing head to objects) since starting everolimus; decreased anxiety and improved sleep were also noted. However, increased nighttime anxiety, sleep issues, mood swings, and recurrence of lip and toenail picking were noted at a follow-up visit in February 2015 (aged 6.7 years). During this time frame, the fluoxetine dose had been increased, which may have contributed to these issues; neurodevelopmental follow-up recommended a switch from fluoxetine to sertraline in April 2015. Additionally, everolimus dosing had been sporadic over this time because of immunosuppression and infections. However, all infections cleared and everolimus dose was therapeutic as of April 2015, and the child remained seizure-free. The most recent brain MRI showed no change in the subependymal giant cell astrocytoma compared with 8 months earlier (Figure 2G and H), abdominal MRI appeared normal, and liver angiomyolipoma was not visualized on ultrasound. At further follow-up, no self-injurious behavior was observed as of February 2016 (aged 7.7 years).
Discussion
Tuberous sclerosis complex is a lifelong disorder associated with numerous clinical manifestations. As a result, the authors implement a multidisciplinary approach to the management of tuberous sclerosis complex, which is in line with consensus guideline recommendations for the diagnosis, surveillance, and management of tuberous sclerosis complex. 2,5 The authors recommend multidisciplinary follow-ups to monitor brain lesions, neurodevelopment, kidneys, lung, heart, and eyes, thus ensuring a comprehensive continuum of care. Table 1 outlines the recommended surveillance measures for a newly diagnosed patient with tuberous sclerosis complex, along with a summary of the results in the present case.
Surveillance Recommendations for Newly Diagnosed Patients With Tuberous Sclerosis Complex.a
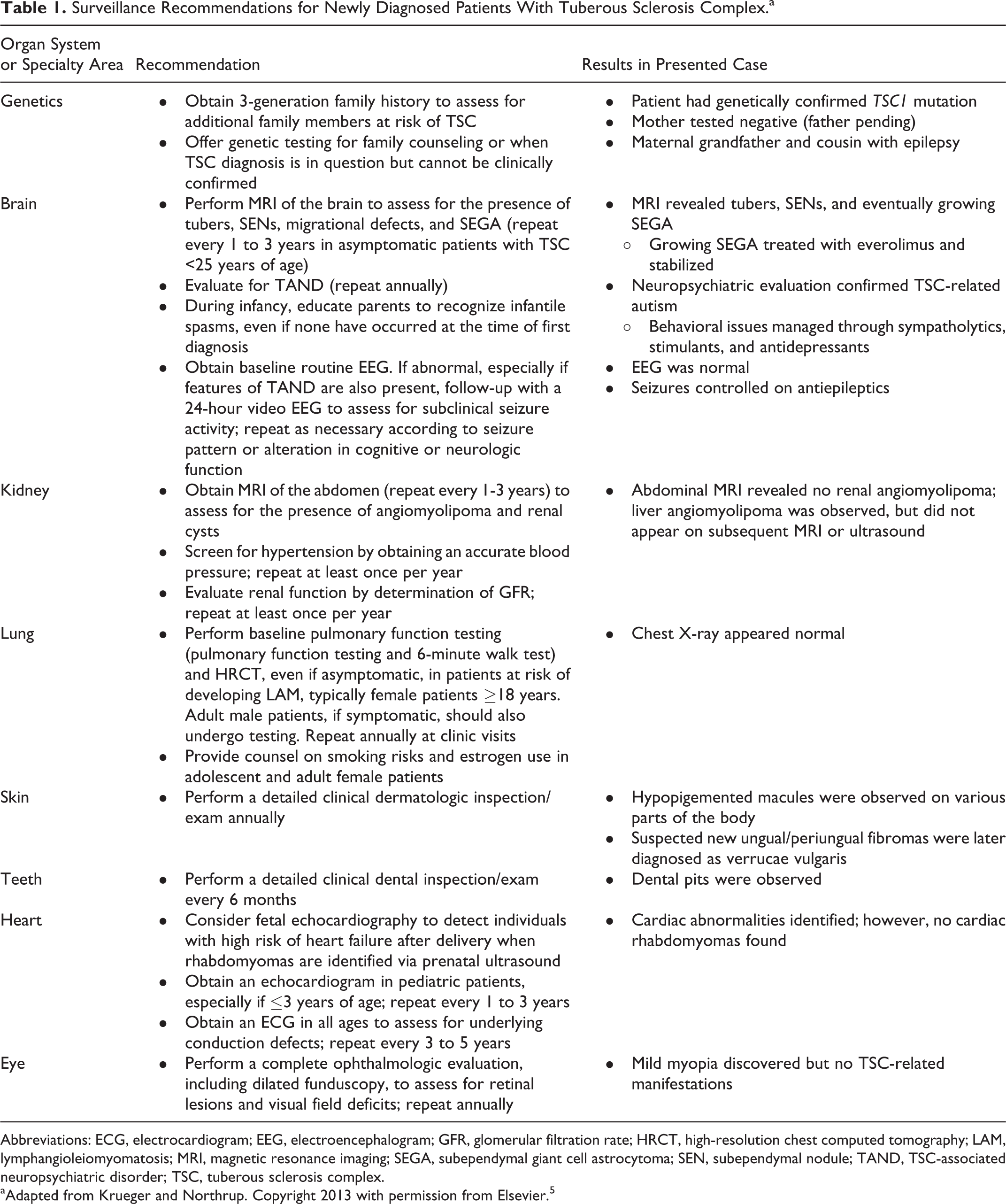
Abbreviations: ECG, electrocardiogram; EEG, electroencephalogram; GFR, glomerular filtration rate; HRCT, high-resolution chest computed tomography; LAM, lymphangioleiomyomatosis; MRI, magnetic resonance imaging; SEGA, subependymal giant cell astrocytoma; SEN, subependymal nodule; TAND, TSC-associated neuropsychiatric disorder; TSC, tuberous sclerosis complex.
aAdapted from Krueger and Northrup. Copyright 2013 with permission from Elsevier. 5
Everolimus has been shown to have systemic effects such as reducing or preventing the growth of subependymal giant cell astrocytomas and renal angiomyolipomas, improving skin lesions, and reducing seizures in patients with tuberous sclerosis complex. 6-8 In this patient case, everolimus was initiated per guidelines 5 after the diagnosis of tuberous sclerosis complex–related subependymal giant cell astrocytoma. While no reduction in subependymal giant cell astrocytoma was observed, the growing subependymal giant cell astrocytoma stabilized, the child became seizure-free, and no additional tuberous sclerosis complex–related issues were observed after >3 years’ follow-up. Although kidney lesions were not observed, renal angiomyolipomas can develop later in patients’ lives, 9 underlining the importance of continuous monitoring. Early detection and effective treatment may prevent these lesions from growing, thus avoiding potential renal function impairments and chronic kidney disease.
The use of everolimus to treat tuberous sclerosis complex has also been reported to improve additional behavioral symptoms associated with the condition, including autistic behavior (social contact, language, and repetitive behavior), concentration, hyperactivity, depression, and seizures. 10,11 Interestingly, in the authors' patient example, some behavioral improvements were observed in the initial months after initiating everolimus, including reduced self-injurious behavior. The authors previously reported improvements in self-injurious behavior with everolimus and other medications in another case, which became variable after everolimus discontinuation. 3 These types of behaviors are typically treated with intensive inpatient or outpatient behavioral therapy, along with nonspecific pharmacologic agents. However, tolerability of pharmacologic agents, such as antipsychotics (eg, metabolic effects), α-2 adrenergic agonists (eg, sedation), antiepileptics (eg, insomnia), antidepressants (eg, fatigue), and stimulants (eg, decreased appetite), may be an issue in the pediatric setting. 12 Everolimus was generally well tolerated in this patient, with side effects manageable by dose interruption. However, although the authors' anecdotal experience, and that of others, indicates that everolimus may improve behavior in individual cases, 3,10 published data from open-label trials of everolimus and sirolimus in larger numbers of patients have not shown any statistically significant improvement in behavior scores. 13,14 Additional studies are, therefore, required to confirm these observations.
Conclusion
This case highlights the importance of vigilance in the follow-up care of patients with tuberous sclerosis complex. Tuberous sclerosis complex is a lifelong illness with different manifestations that can occur at different points in a patient’s lifetime. As a result, a multidisciplinary approach to care is required to ensure early detection and appropriate treatment, thus potentially improving long-term outcomes.
Footnotes
Authors’ Note
Medical writing and editorial assistance was provided by Traci Stuve, MA, and Maxwell Chang of ApotheCom (Yardley, Pennsylvania).
Author Contributions
TTG contributed in the study conception and design and the acquisition, analysis, and interpretation of data. TTG also contributed to drafting and critical revision of the manuscript and gave final approval to submit. AP contributed to data analysis and interpretation, critically revised the manuscript, and gave final approval for manuscript submission. Both authors agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TTG served as a principal site investigator for a Novartis study (EXIST-3); funding was provided to her institution only.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Medical writing and editorial assistance was funded by Novartis Pharmaceuticals Corporation.
Ethical Approval
The institutional review board at Johns Hopkins School of Medicine approved this work.