
Abstract
Objective:
To study the link between malaria and epilepsy in children in Parakou district.
Methods:
This case-control study included children 1-15 years of age with epilepsy. Each case of epilepsy was matched to 2 controls for age, sex and neighborhood of residence. The exposure variables were a history of malaria (number and type), family history of epilepsy and other past medical history. The odds ratios (OR) and their confidence interval were used to estimate association.
Results:
A total of 123 children including 41 children with epilepsy and 82 controls were included. The overall average number of malaria episodes per year in both groups combined was 1.8 ± 0.9 episodes. In the multivariate analysis, cerebral malaria (OR: 50.35 [5.28-480.30]), family history of epilepsy (OR: 12.17 [2.15-69.01]) and number of malaria episodes (OR: 13.27 [4.53-98.48]) were associated.
Conclusion:
This study supports the association between cerebral malaria and the onset of epilepsy.
Epilepsy, a common and serious neurological condition, is one of the most prevalent diseases in the world. The World Health Organization (WHO) estimates that about 50 million people are affected worldwide, 80% of them in developing countries. 1 The prevalence of this disease in low-income countries may attain 190 per 100,000 people. In the face of accelerated population growth in these countries, epilepsy represents a heavy health and socio-economic burden for which measures are urgently needed. 2
Malaria is one of the major infectious diseases in Africa. It is a major cause of death in children. Among the clinical expressions, neuro-malaria or cerebral malaria (CM) is one of the serious forms. 3,4 It is defined as a persistent coma at least 30 minutes after a seizure or correction of hypoglycaemia and the detection of asexual forms of Plasmodium falciparum in the peripheral blood, apart from any other cause of encephalopathy. 5 Its incidence in endemic areas in sub-Saharan Africa is 1.12 new cases per 1000 children per year with a mortality of 18.6%. 6 Cerebral malaria leads to significant neurocognitive sequelae, especially in children. These sequelae include epilepsy. Indeed several authors have reported the existence of an association between cerebral malaria and the occurrence of epilepsy. 7 In Parakou, cerebral malaria is common. A study conducted at the Centre hospitalier Universitaire Départemental (CHUD)/ Borgou, found a hospital admission rate of 21.4% in 2017. 8 The occurrence of cerebral malaria exposes the child to a risk of epilepsy. We aimed to determine the relationship between epilepsy and malaria in children aged 1 to 15 in the city of Parakou.
Methods
Type and period of study
This was a case-control study.
The data collection took place over the period from 1st August to 30 November 2018.
Setting
It took place in the city of Parakou located 425 km from Cotonou in northern Benin. It is the third largest city in Benin with a population of over 250,000. It has 2 hospitals. Two (2) neurologists and 7 pediatricians work there. It has 1 scanner unit and an electroencephalography unit.
Study population
It consisted of all children aged 1 to 15 years, with or without epilepsy and living in Parakou. With regard to cases, these were children with epilepsy (confirmed by a neurologist) aged 1 to 15 years and living in Parakou. Epilepsy was defined by the repetition of epileptic seizures in a child with no particular context and defined according to the International League Against Epilepsy. Only epileptics adhering to these criteria, confirmed by a neurologist were included in the study.
Subjects with no history of epilepsy and no paroxysmal symptom aged 1 to 15 years were used as controls. Each case of epilepsy was matched to 2 controls for age, sex and neighborhood of residence.
All subjects: aged from 1 to 15 years old who met the definition of case or control; resident in Parakou for at least 6 months; with no major cognitive impairment; whose parental consent had been obtained were included.
All subjects whose parents / guardians were unable to answer questions and / or whose medical records were not available were excluded.
Sampling
Sampling size
The sample size was calculated assuming that the odds ratio between cases and controls was 4 taking as risk of first species 0.05 and a risk of second species 10% (power of 90%). Two (2) controls per case with a malaria crisis incidence of 45% were obtained using the Epitable software of Epi-Info version 6.04, a minimum number of 41 cases and 82 controls.
Sampling Technique
We conducted an exhaustive recruitment of cases of epilepsy through a review of medical records (pediatrics, neurology departmental Parakou University Hospital and Saint Gerard medical center of Parakou) of patients to identify cases. All children with epilepsy (1-15 years old) with their parents were contacted and invited to participate in the study. These cases was then matched to the controls.
The controls were children recruited from the place of residence (same residential area) by a random selection from children meeting the inclusion and matching criteria.
Collection of data
Observation, the interview and documentary review were used to collect the data in the children from the parents / guardians in their living environment. In the health centers, we used the consultation and hospitalization registers to identify the cases. A survey sheet was used to collect the information data on previous episodes of malaria (form and number of episodes), treatments received, and children’s past medical history were collected from hospital records and from parents through an interview or through health records.
The diagnostic criteria for malaria and cerebral malaria are those of the World Health Organization. Malaria was diagnosed from suggestive clinical signs with a thick or positive blood smear. Cerebral malaria was diagnosed on the basis of thick positive drop or asexual Plasmodium falciparum in blood smear with consciousness disorders (or coma) no followed convulsions, hypoglycemia and exclusion of other cause of this coma.
The difference of simple malaria and cerebral malaria was based only on the presence of neurological signs (loss of consciousness; convulsions…).
These data were indicated in the files of hospitalization or the medical notebook of the children.
Analysis and Data Processing
The data collected were recorded and processed with the software EPI INFO (version 7.2) and SPSS 21. The quantitative variables were expressed as mean with 1 standard deviation, and the qualitative variables expressed by simple count and in percentage. Frequencies Incidences and averages were compared by the Chi2 test. Epilepsy was operationalized in 2 modes: children with epilepsy (Epilepsy group) and children without epilepsy (non-epilepsy group) secondly. Then we proceeded to an individualization of the independent variables in 2 categories. A step-down logistic regression analysis was performed by simultaneously introducing all variables with p less than 0.05 in bivariate analysis. The adjusted odds ratios (ORs) were calculated to measure the strength, meaning, and stability of the association between each independent variable and epilepsy. For all these tests, of significance level was 5%.
Ethical Aspects
The protocol of the study was approved by a local committee of ethics in biomedical research of the University of Parakou. The authorizations of the academic and administrative authorities were obtained before the start of the study. Information on the purpose of study, importance, and scope of our study was provided to the participants. Then only the oral and informed consent of each parent was obtained since many of the parents had no level of instruction. Data was collected anonymously and confidentially.
Results
A total of 123 children including 41 cases of children with epilepsy and 82 controls were included in the study. The mean age for both groups was 10 ± 3.9 years; with a median of 11 years. The minimum age (min) was 2 years old and the maximum age (max) was 15 years old. The sex ratio (m / f) was 0.95 in both groups. In terms of educational attainment, 46.34% of the epilepsy group were not in school and none had completed secondary school, while, among the non-epilepsy group, only 7.32% were not in school and 21.95% had completed secondary school (Figure 1).
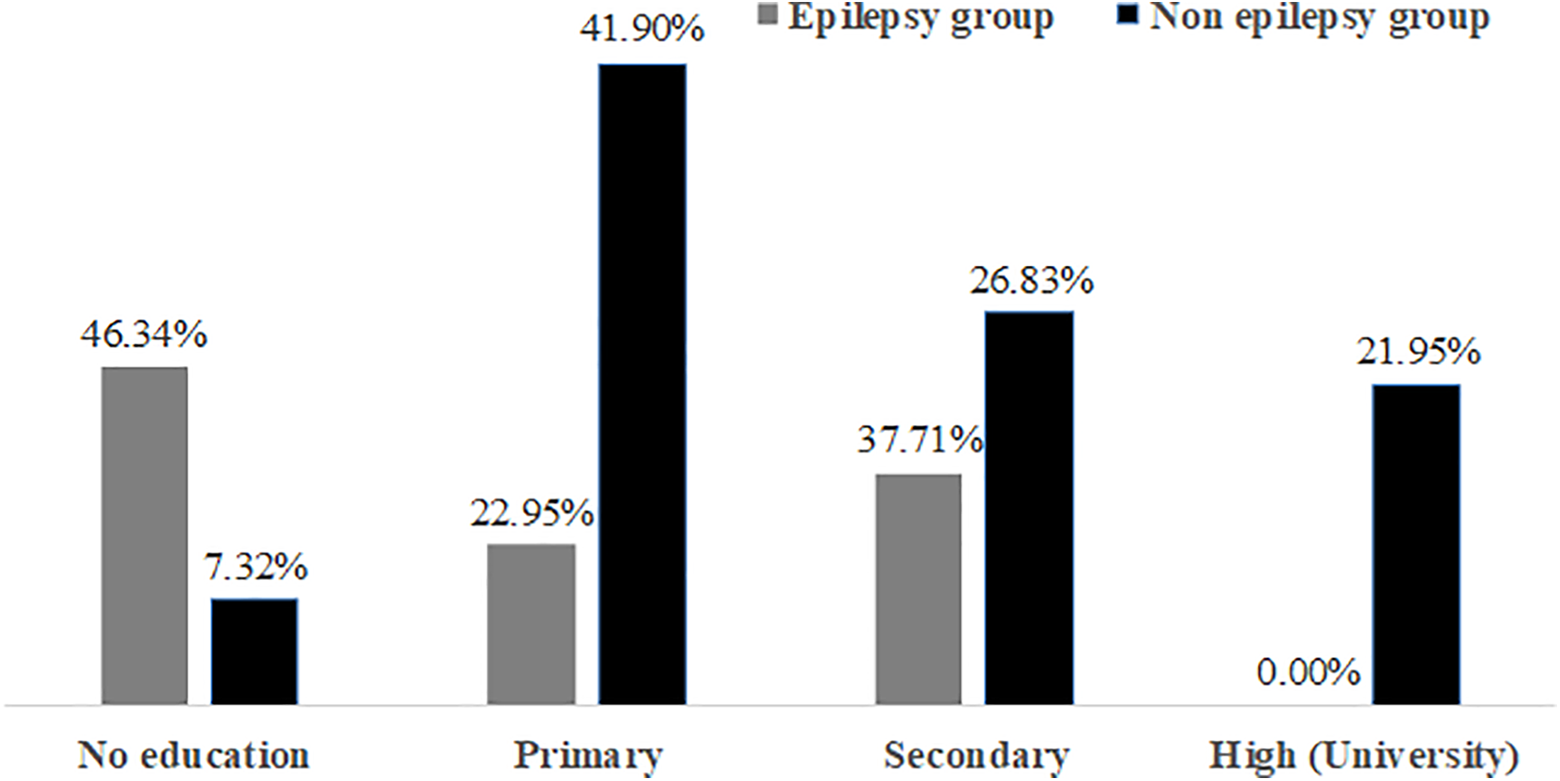
Distribution of the 2 groups according to the level of education of children in Parakou in 2018.
In our study, all 123 children in both groups had a history of simple malaria. However, the incidence of severe malaria differed in the 2 groups. While 70.73% of the epilepsy group had a history of severe malaria, only 14.63% of the non-epilepsy group had a history of severe malaria.
The average number of malaria episodes per year in both groups was 1.8 ± 0.9 episodes; with a median of 2 episodes. The minimum (min) was 1 episode and the maximum (max) 4 episodes. The average number of episodes of malaria per year of children with epilepsy was 2.5 ± 0.9 episodes. The average number of malaria episodes per year of the no epilepsy group was 1.45 ± 0.6 episode (p-value = 0.0001).
The mean age of onset of the first malaria attack for the 2 groups combined was 20 ± 14.05 months; with a median of 12 months. The minimum age (min) was 2 months and the maximum age (max) was 84 months. The mean age of onset of the first case of malaria in epilepsy group was 15.43 ± 10.74 months. The average age of onset of the first case of malaria in control group was 23.50 ± 14.77 months with p = 0.002. Episodes of convulsions occurred in 41.6% of children with epilepsy while none of the children without epilepsy had had convulsions
The factors associated with the occurrence of epilepsy in children with malaria were a family history of epilepsy p = 0.001, parental education level p = 0.035, the number of episodes of malaria per year p = 0.001, severe malaria with p = 0.001 and complicated forms such as cerebral malaria p = 0.001, anemia p = 0.004 and hemolysis p = 0.003 (Table 1). But in the multivariate analysis the family history of epilepsy (OR), a cerebral malaria (OR) and a significant number of episodes of malaria were associated with epilepsy. These data are summarized in Table 2.
Factors Associated With the Occurrence of Epilepsy in Children With Malaria in Parakou in 2018.

Factors Associated to Epilepsy in Children With Malaria in Parakou in 2018 Using Multiple Logistic Regression.

OR: odds ratio.
Discussion
The aim of this study was to study the relationship between epilepsy and malaria. To do this an observational study of the analytical type is appropriate. The interest of the case-control study is to study very quickly the association between a disease and several exposure factors at the same time. The choice of community cases and controls from the consultation registers (case) makes it possible to ensure the correct definition of cases that are confirmed epileptic patients and monitored by a neurologist. This choice is guided by the desire to avoid confounding bias related to hospital cases that may not be epileptic due to lack of hindsight. Our methodology could quantify this association. This type of study made it possible to simultaneously study the relationship between several exposures and epilepsy. We collected the children’s history from the diaries, the parents’ statements and the hospital and clinical records. This could introduce information biases related to the quality of the data collected.
In our study, the average age for both groups was 10 ± 3.9 years. The average age obtained is similar to that reported by Ngoungou et al in a study in Gabon that returned to an average age of 11.4 (± 6.3) years. 9 It should be noted that the majority, that is to say more than 50% of the population in Sub-Saharan Africa (SSA) is under 15 10 and female as in Nigeria. 11 A study by Kaputu-Kalala-Malu C et al on protracted convulsions in children in sub-Saharan Africa shows a male-to-female sex ratio of 1.02 in favor of males. 12 This could be explained by differences in populations and methods of study.
In our study, 46.34% of children with epilepsy were not attending school compared to 7.32% of controls. This could be explained by the fact that epilepsy has a significant social impact in that it affects the quality of life of the child. In the African context, epilepsy has a deleterious impact on schooling and the professional development of children who suffer because it is a stigmatizing condition. Epilepsy is considered to be of mysterious origin. According to a study carried out in Nigeria, more than 20% of children leave school because of epilepsy and more than 39.5% of those who reach university level show poor performance compared to non-epileptic patients as a corollary of difficulties of schooling. 13
The average number of malaria episodes per year in both groups was 1.8 ± 0.9 episodes; epileptic children had up to 4 episodes of malaria a year. In both groups, 100% of epileptic patients, like non-epileptic subjects, had had simple malaria. Severe malaria was observed in 29 (70.73%) of epilepsy group and in 12 (14.63%) of no epilepsy group. As for cerebral malaria, 31.71% of children with epilepsy had suffered against 2.44% controls. Similarly, convulsions were present in severe malaria in 41.46% of children with epilepsy against zero in the controls. In the study by Ngoungou et al in Gabon, of the 296 children with epilepsy, 26 (8.78%) had cerebral malaria, while of the 296 without epilepsy, 10 (3.38%) had cerebral malaria. 9 These results are consistent with ours. cerebral malaria is associated with neurological manifestations that can lead in the long term to neurocognitive sequelae including epilepsy. 14 Ngoungou had reported that exposure to cerebral malaria multiplied by 3.9 the risk of epilepsy; these results are similar to ours (OR = 3.34). Similarly, the existence of other signs of severity, such as anemia and hemolysis, increased the risk of epilepsy in our study. In general, children with severe malaria were 4 times more likely to have epilepsy. Thus we can say that malaria is a serious condition that especially in its neurological form that gives rise to a risk of epilepsy of 3.34 in our context.
At the end of our study, a statistically significant relationship was noted between severe malaria and the occurrence of epilepsy. This result corroborates that of Ngoungou who also found a statistically significant relationship between cerebral malaria and epilepsy with a p-value = 0.002. 15 A case-control study cannot induce causal conclusions. However, consistent studies exist to suspect this causality. 9,10 The results of the studies by Preux et al in 2002 and those of Carter et al in 2004 in Kenya found a relationship between malaria and epilepsy. 16 Although epilepsy is not the most common neurological sequelae of severe malaria, the large number of cases of severe malaria in sub-Saharan Africa suggests that it could contribute significantly to the burden of epilepsy in this sub-Saharan Africa continent.
Many risk factors can explain the occurrence of epilepsy. As with many diseases, the goal remains prevention, which must be based on the identification of risk. In sub-Saharan Africa, malaria is one of those parasitic diseases whose role in the occurrence of epilepsy has often been mentioned without being the subject of real research. 17 In our study, other factors were associated with the occurrence of epilepsy in children with malaria. These were parents’ educational level (p = 0.003), the number of malaria episodes per year (p = 0.000) and the age of onset of malaria (p = 0.003). Severe malaria is more common in children 18 ; among those who survive, even if they do not have clear sequelae, at least 10% of them still have neurological abnormalities when they leave hospital. The majority of these neurological sequelae apparently disappear some time later, but some persist and have a long-term impact on the psychomotor and intellectual development of the child. 19 Epilepsy is a neurological sequel that must be taken into account in patients who have suffered from severe malaria. In Gabon, Ngoungou et al found an association between epilepsy and cerebral malaria, although the cases in this study were hospitalized children and controls recruited from hospital. 20 Other studies reported the relationship between cerebral malaria and sequelae epilepsy 21,22
In routine clinical practice, the use of the fundoscopic 23 exam and admission EEG 24 can aid in the diagnosis of cerebral malaria. Recently, however, we have been using the measurement of the diameter of the optic nerve on ultrasound for the diagnosis of intracranial hypertension in cerebral malaria. 8 In addition, cerebral malaria associated with retinopathy is highly predictive of the occurrence of epilepsy and severe neurological sequelae. 25 This tool should make it possible to predict children at risk of developing epilepsy at a later date and thus optimize management.
Conclusion
Epilepsy seems to be significantly associated with malaria, especially in its severe forms, particularly cerebral malaria. Intensive control and appropriate management of this parasitosis could reduce the burden of epilepsy in malaria-endemic countries.
Footnotes
Author Contributions
T. Adoukonou and F Agbeille and C Bokossa conducted data analysis and wrote the first draft of article. All authors reviewed the manuscript and approved the final manuscript Agbeille, E Dovoedo, C Bokossa participated in the data collection. M. Agbétou, D. Adedemy, A Noudamado and J Agossou participated in critical revision of the manuscript T. Adoukonou and M Agbetou were responsible for diagnosing of epilepsy. F Agbeille, D. Adedemy, A Noudamado and J Agossou were responsible for diagnosing cerebral malaria. All authors reviewed the manuscript and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical Aspects is included at the end of the methods section.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.