
Abstract
The incidence of childhood central nervous system tumors in infants is about 6 per 100 000 children. Recent studies have showed recurrent fusion of the neurotrophic tyrosine receptor kinase (NTRK) gene in 10% of non-brainstem high grade glioma in very young children suggesting an oncogenic effect of the NTRK fusion genes. In this report, we present a rare, severe case of a full-term neonate who was noted to have widely splayed sutures and a bulging fontanelle at birth who was found to have infant-type hemispheric glioma with NTRK1 fusion with course complicated by seizures refractory to medical treatment. Patient was deemed a poor surgical candidate due to the size of the mass and thus parents opted for comfort care.
Introduction
The incidence of childhood central nervous system tumors in infants is about 6 per 100 000 children with glioma having the highest incidence at 1.38 per 100 000.1,2 Recent studies have showed recurrent fusion of the neurotrophic tyrosine receptor kinase (NTRK) gene in 10% of non-brainstem high grade glioma in very young children suggesting an oncogenic effect of the NTRK fusion genes.3,4
Here we present a rare, severe case of a full-term neonate who was noted to have widely splayed sutures and a bulging fontanelle at birth who was found to have infant-type hemispheric glioma with NTRK1 fusion.
Case
A full-term infant with normal prenatal course, including a 20-week anatomy scan, was born with widely splayed sutures, bulging anterior fontanelle and head circumference >99th percentile (40 cm). Head ultrasound showed severe hydrocephalus and a large intracranial mixed echogenicity lesion in the left cerebral hemisphere with hemorrhage. He had sustained leftward gaze, and video EEG revealed seizures that were refractory to medical treatment. MRI demonstrated a large 6 × 7cm lesion, hydrocephalus with subfalcine herniation and mass effect on the brainstem (Figure 1A-B). He underwent biopsy and ventriculoperitoneal shunt placement. MRI 2 weeks later showed tumor enlargement, obstructive hydrocephalus and severe brainstem compression (Figure 1C-D). Pathology was consistent with infant-type hemispheric glioma with NTRK1 fusion. Neurosurgery evaluated patient, who was deemed a poor surgical candidate due to the size of the mass and very young age. In the setting of this assessment, the patient's severe refractory seizures, and the resulting dismal prognosis, parents opted for comfort care.
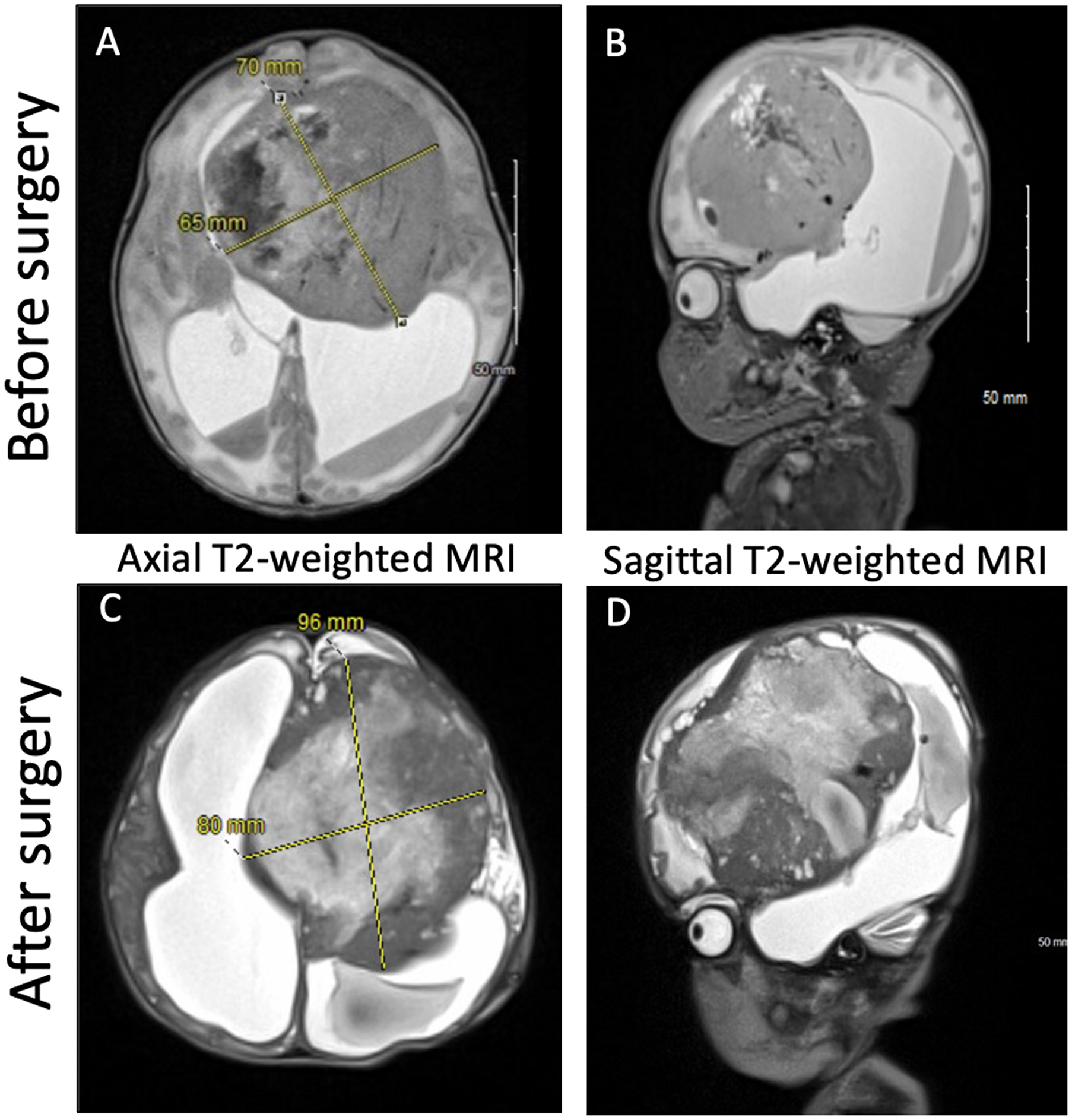
(A-B) Preoperative imaging. (C-D) Postoperative imaging 3 weeks after shunt placement and biopsy demonstrates a progressively enlarging mass and severe hydrocephalus.
Discussion
Infant-type hemispheric glioma, previously termed glioblastoma (GBM), is a rare, rapidly-growing congenital tumor, and prenatal imaging is often normal. Mixed-age hemorrhages and diffusion restriction is suggestive of the diagnosis. 5 Our patient represents an unusual presentation of this rare disorder due to the size of the tumor and diagnosis made at birth.
As seen in our patient, the NTRK genes NTRK1, NTRK2, and NTRK3 are involved in infant-type hemispheric gliomas, which are typically high grade in histology. A recent study by Torre et al showed most NTRK-fused gliomas were hemispheric and had a higher prevalence in non-brainstem high grade gliomas in patients younger than 3 years old. Although historically associated with high mortality and/or recurrence due to their high grade histology and aggressive nature, the prognosis of NTRK-fused gliomas may change with the recent FDA approval of selective pan-TRK inhibitors, larotrectinib and entrectinib. 6
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.