
Abstract
This article reexamines the healthy immigrant effect in mental health—as measured by psychological distress—by incorporating the modifying roles of the level of economic development of origin-country and life-stage at arrival among a sample of immigrants to Toronto, Canada—as compared to the native-born. The analytic sample included 2,157 adults, of which 31 percent were immigrants. Multivariate results point to a healthy immigrant effect in distress, but only among immigrants from less developed origin-countries who migrated to Canada in mid-adulthood (between 25 and 34 years of age). Further, this health advantage deteriorates with increase in length of residence only among this group of migrants, in large part because of an increase in chronic stressors. Immigrants from more developed origin-countries do not experience a healthy immigrant effect, as compared to the native-born, nor an increase in distress with tenure in Canada, irrespective of the life-stage at immigration.
Keywords
Introduction
Migration from one country to another, often highly developed country of the world, has been steadily increasing over the past 100 years. In Canada, immigrants have accounted for a growing proportion of the population since the 1950s (Palameta 2004). In 2011, 6.7 million immigrants from close to 200 origin-countries resided in Canada (Statistics Canada 2013); conservative estimates project this number to increase by 334,000 per annum by 2035/2036 (Statistics Canada 2014). The growing number of foreign-born Canadians highlights the importance of understanding immigrant emotional well-being for long-term societal “health” (Antecol and Bedard 2006).
While a substantial body of research has examined the physical health of the foreign-born (e.g., Antecol and Bedard 2006; Jasso et al. 2004; Riosmena, Wong, and Palloni 2012), research on the mental health of immigrants is more limited. Yet, mental health is a central indicator of the adaptive response of immigration (Ataca and Berry 2002) and thus may be more sensitive to variation in the unfolding experience of migrants in a host-country. As with findings for physical health, the majority of research on nonrefugee immigrant emotional health outcomes finds that upon arrival in the host-country immigrants report the same or lower levels of emotional problems than the native-born, but that over time this psychological health advantage decreases (Aglipay, Colman, and Chen 2013; Cook et al. 2009; Jasso et al. 2004). This phenomenon is called the “healthy immigrant effect,” hereafter referred to as the HIE. While, the better mental health of immigrants has been attributed to selection factors at the individual and host-country levels (Kennedy et al. 2015), the decline in mental health with time in the host-country has been attributed, in part, to the accumulation of chronic stress exposure over time (Cook et al. 2009; Montazer and Wheaton 2017).
The majority of work on immigration and mental health has focused on specific immigrant groups from specific origin-countries (Aglipay et al. 2013). Research that focuses on immigrants migrating from the same origin-country is important because it shines light on the distinctiveness of the migration experience. However, such research misses similarities in experience across groups that likely exist because of origin-country contextual level commonalities, such as the level of economic development, at the time of migration (Montazer and Wheaton 2011, 2017). Country-level economic conditions reflect differences in opportunity structures, the quality of life, and availability of resources in origin-countries that may impact the initial adjustment and eventual trajectory in outcomes, including mental health, for immigrants postarrival to the host-country (Jasso et al. 2004; Montazer and Wheaton 2011, 2017). To achieve a broader explanation of the immigration process and to allow for generalization beyond specific cases, previous scholars have advocated for the incorporation of country-level characteristics across a wide range of sending countries (Montazer and Wheaton 2011, 2017; van Tubergen et al. 2004). Thus, the first aim of this article is to consider the effect of an important macro-economic condition—economic development—of origin-country on immigrant mental health.
However, while macrolevel contexts of exit are important, it is also essential to consider individual-level factors such as life-stage at arrival, which has been shown to have significant mental health consequences for migrants (Mossakowski 2007; Takeuchi et al. 2007). For example, the HIE has mostly been observed among immigrants who came to the host-country as adults (Mossakowski 2007). By using data from the Neighborhood Effects on Health and Well-being (NEHW) study (O’Campo et al. 2015), this article investigates (1) whether the HIE in psychological distress is modified by the level of economic development of the origin-country, and (2) the life-stage at immigration; (3) whether the increase in distress with tenure in Canada is altered by these two factors; and, if yes, (4) whether a sense of “failed expectations” and increase in chronic stress exposure explain the relationship between time in the host-country and psychological distress. The NEHW study is based out of Toronto, a major city in North America that shares many of the economic, social, and cultural givens of the “new world” with other major American and Canadian cities. Toronto is home to the largest share of the foreign-born in Canada (Statistics Canada 2013), making it an ideal setting for the study of immigrant adaptation.
Background
Immigration and Mental Health
Considerable debate on whether immigrants have higher or lower rates of emotional health problems than the native-born has permeated the literature over the past century (Takeuchi 2016). Early-twentieth-century scholarships on immigrants predicted higher rates of mental-health problems among the foreign-born that were expected to decrease with time in the host-country (Thomas and Znaniekcki [1918–1920] 1984). These studies often relied on the traditional “straight line” theory of assimilation (Warner and Srole 1945), which (1) viewed immigration to be inherently stressful and thus associated with poor mental health among new arrivals; and (2) viewed the process of the immigrant group’s adoption of the “cultural patterns” of the host society—acculturation—(Alba and Nee 1997) to be the only route for the improvement of immigrants’ well-being.
Contrary to the abovementioned findings, however, newer research on post-1965 immigrants overwhelmingly reports a HIE: lower average levels of mental-health problems—that is, depression, psychological distress, or anxiety—among immigrants than the native-born (Aglipay et al. 2013; Cook et al. 2009; Jasso et al. 2004). The HIE is a counterintuitive finding given that immigrants, on average, have lower social support and lower socioeconomic status (SES) than the native-born—at least initially (Antecol and Bedard 2006; Montazer and Wheaton 2017; Riosmena et al. 2013; Salas-Wright, Kagotho, and Vaughn 2014). Both of these factors are associated with adverse mental health (Eaton, Muntaner, and Sapag 2010; Turner and Brown 2010). Usually, these challenges appear to diminish with time in the host-country, as immigrants’ economic conditions improve, they find employment, and they develop social relationships (Salas-Wright et al. 2014). Despite the social and economic assimilation of immigrants, however, the process of acculturation over time is found to be associated with a decline in the mental-health advantage of immigrants with tenure in the host-country. Although the starting point in traditional theories is the opposite of the HIE reported in newer immigration research, in both models the end result is the same level of well-being as the native-born: mental health assimilation. While the former model predicts this mental health status to be a result of progress, the later predicts this mental health status to be a result of deterioration.
Healthy Immigrant Effect and Psychological Health
Two popular theories have been put forth to explain the HIE. One theory is based on the notion of immigrant self-selection: only the most able in terms of health and resources are able to migrate. Another theory argues that receiving countries’ immigration policies indirectly impact the health profile of the immigrant population (Kennedy et al. 2015). In Canada, for example, the 1967 points system promotes immigrants who are well-educated, skilled, employed, parents, and married (Boyd and Vickers 2000), which could indirectly impact the emotional profile of the immigrant population (Montazer and Wheaton 2017). These two theories, of course, are not mutually exclusive: Canada’s attempt to select the most qualified immigrants may also induce positive self-selection since only those individuals who have the greatest chances of gaining entry will apply in the first place (Kennedy et al. 2015). Despite the popularity of these theories, however, the HIE often holds even after controlling for education, age and other health ameliorating characteristics (Kennedy et al. 2015; Montazer and Wheaton 2017).
The deterioration of this mental-health advantage over time has been attributed to an increase in varying types of chronic stressors with tenure in the host-country that accompany acculturation (Cook et al. 2009; Montazer and Wheaton 2017; Savage and Mezuk 2014). Chronic stressors are threats, demands, or structural constraints that are continuous in nature, develop insidiously, and are usually non-self-limiting (Wheaton et al. 2013). However, immigrants are not a homogeneous group and, as argued by the conditional adaptation model (Montazer and Wheaton 2011, 2017) and segmented assimilation theory (Portes and Zhou 1993) there are diverse trajectories of adaptation and incorporation into the host-society that can impact the HIE. The level of economic development of the origin-country (e.g., Jasso et al. 2004; Kennedy et al. 2015; Read, Emerson, and Tarlov 2005) and the life-stage at immigration (Mossakowski 2007; Takeuchi et al. 2007) are two such important modifiers of this phenomenon.
Healthy Immigrant Effect and Economic Development
While all immigrants, irrespective of origin-country are positively selected at the time of migration (Kennedy et al. 2015), selection is likely highest among immigrants from the poorest and most underdeveloped countries (Jasso et al. 2004; Read et al. 2005). This is because the cost of migration from such countries is greater and may require more resources (Jasso et al. 2004). Selection, however, may not be the only reason for the better mental health among this group of immigrants, since the HIE is not explained away among this group of the foreign-born once studies adjust for health ameliorating factors (e.g., Montazer and Wheaton 2017). This health gap may also be due to unobserved selection criteria of immigrants from the most socioeconomically distant origin-countries, such as perseverance in the face of adversary, being forward-looking (Kennedy et al. 2015) and having higher expectations about life in a host-country perceived to offer better opportunities and life conditions than the one left behind (Rote and Markides 2014).
The level of economic development of origin-countries may also impact the mental health of immigrants with tenure in the host-country. In general, schooling and work experience obtained in less developed countries is not recognized as equivalent to that obtained in more economically advanced countries (Bratsberg and Ragan 2002). While migrants from less developed origin-countries might not be as negatively impacted initially by the lower transferability of their human capital because of greater perceived social distance to the majority group (Shibutani and Kwan 1965), they may have a harder time accepting the barriers in access to opportunities and rewards as their perception of social distance decreases with tenure in the host-country (Montazer and Wheaton 2017). The above lays the groundwork for greater feelings of disappointment, or “failed expectations,” with time in the host-country, which leads to greater experience of stressors in other spheres—that is, financial (Bratsberg and Ragan 2002), work (Magee and Umamaheswar 2011), and family (Cook et al. 2009; Montazer and Young 2017). The deteriorating effect of this “stress proliferation” (Pearlin 1999) may accumulate over time, leading to an increase in mental-health problems only among this group of migrants.
Healthy Immigrant Effect, Economic Development and the Life-stage at Immigration
According to segmented assimilation theory, there are various patterns of psychosocial adaptation that depend on an individual’s characteristics (Portes and Zhou 1993)—such as the life-stage at immigration and level of economic development of origin-country, as argued here. Thus, the stage of the life-course at which immigration occurs adds another layer of complexity to the effect of the level of economic development of origin-country on the mental health outcome of immigrants. There are fundamental differences in the decision and reason for migration between persons who immigrate as adults and those who do so as children (Rumbaut 2004). Specifically, only adults actually go through a selection process at the time of migration, or make the choice to migrate in the first place (Mossakowski 2007), and they are better able to understand the effect migration will have on their life conditions. Children do not choose to emigrate and their mental health is not likely a selection criterion by the family or by the officials of the destination-country (Landale et al. 1999). Indeed, studies show that those who immigrate in adulthood have better mental health than the native-born and their foreign-born counterparts who migrated in childhood (Mossakowski 2007). Thus, those who immigrate in childhood, irrespective of the level of economic development of origin-country, should have the same level of mental health than the native-born, partly because selection is less relevant among this group and they may be less likely to understand migration as betterment in life conditions. Furthermore, because those who immigrate in childhood acculturate more easily than older migrants (Cheung, Chudek, and Heine 2011; Rumbaut 2004) and are able to incorporate into the host-society and make informative connections early in life (Setia et al. 2011), this group of immigrants should not experience an increase in failed expectations and, as a result, an increase in the level of chronic stressors and mental-health problems with time in the host-country, irrespective of the level of economic development of origin-country.
Contrary to child immigrants, the specific stage of the life-course at immigration may have important consequences for selection and eventual mental health trajectory among adult migrants. People are influenced differently by change depending on their age-specific personal histories (Elder 1987). Immigration scholars generally agree that immigrants experience changes in a number of life outcomes (including mental health) as they accommodate to life in a new society, but that these changes are often limited to those who came to the host-country as adults (Alba and Nee 1997). For example, while those who migrate in early-adulthood (before 25) and those who migrate in mid-adulthood (25–34) both may bring a future-oriented outlook to their new host-country (Rumbaut 2004), those who migrate in mid-adulthood should be selected more by immigration policies, such as the points system in Canada, since these migrants generally emigrate after having completed their education, at the beginning of their work careers, and in their peak childbearing and family-formation years (Rumbaut 2004)—all important variables in Canada’s selection process of the best and brightest possible immigrants. This selection, as stated earlier, should be clearest among those from the least economically developed countries.
Mid-adulthood immigrants, particularly those from less developed countries, should also experience greater failed expectations, and consequently higher chronic stressors, with time in the host-country because the lower return to education and experience obtained in less developed origin-countries should be clearest among those who come at the most forward-looking stage of the life-course. While those that migrate after the age of 35 (later-adulthood) are also a highly selected group because they come with years of prior work experience, “they are unlikely to shed their native languages, customs and identities in the process of their accommodation to the new society” (Rumbaut 2004:1167). Therefore, the foreign-born who immigrate in later-adulthood may experience a more attenuated mental-health trajectory with tenure in the host-country than other adult migrants. This group of migrants may never feel truly Canadian—experience a true decrease in social distance—and thus may not be as negatively impacted by the disappointments of postmigration failed expectations.
The aforementioned argument leads to the following hypotheses:
Method
Data
The data for the study come from the NEHW study (O’Campo et al. 2015), which is an individual-level data set gathered using a cross-sectional, multilevel design across 47 neighborhoods in the metropolitan city of the Greater Toronto Area (GTA). Face-to-face interviews were conducted with ~20 to 30 respondents in 87 census tracts across the city-defined neighborhoods in Toronto. The NEHW data set comprises interviews with 2,412 individuals conducted between 2009 and 2011. The response rate was over 80 percent. To be eligible for study participation, individuals had to be a resident of the selected household, between the ages of 25 and 64, able to communicate in English, and had lived in the neighborhood for at least six months (for more detail on sampling/study design see O’Campo et al. 2015). Sampling weights were derived to correct for any selection biases that may have occurred due to these sampling restrictions, such as the underrepresentation of the most recent immigrants. Refugees were excluded from the analyses (N = 46) because they are a different group socially and economically than the general immigrant population (Setia et al. 2011). Furthermore, only the foreign-born with valid information on birth-country and length of residence were included in the analytic sample yielding a final sample size of 2,157 respondents of which 679 were foreign-born. The foreign-born participants in the NEHW study vary in age, age at immigration, and length of residence (LOR), which is important to disentangle the effect of life-stage at immigrant from tenure in the host-country (Cheung et al. 2011).
Variables
Psychological distress is measured by taking the mean across 16 items adapted from Radloff’s (1977) Center for Epidemiologic Studies Depression Scale (CES-D). Respondents were asked how often they felt “everything was an effort,” “depressed,” or “as though they could not get going,” for example. Respondents are asked whether they felt symptoms such as these “none of the time” (1), “a little of the time” (2), “some of the time” (3), “most of the time” (4), or “all of the time” (5). An index of these items was created so that higher scores reflect greater psychological distress (α = .95).
A number of steps were taken to create economic development/life-stage at immigration categories. First, economic development of origin-country was measured by the Gross National Product (GNP) per capita of origin-country at the time of emigration (The World Bank, 1962–1986a, 1962–1986b; see Montazer and Young 2017 for further detail on classification of origin-country GNP at the time of emigration), which in the analytic sample went as far back as 1963. Respondents were asked “in what country were you born?” and “in what year did you come to live in Canada?” to correctly match respondent’s origin-country with the corresponding GNP per capita category for the year of arrival. This classification also includes the GNP for all intermediary countries beyond origin where respondents may have acquired additional human capital. If an immigrant reported living in an intermediary country, and having received his or her highest level of education in that country, the intermediary country’s GNP at the time of arrival was used instead of the origin-country GNP. Extending origin-country human capital to include human capital obtained in intermediary countries prior to migration—especially if human capital acquisition occurred in developed countries—is important because it will likely impact postmigration expectations, whether these expectations are met, and the occurrence of chronic stressors postarrival (Montazer and Young 2017). GNP was coded into two dummy variables: lower-GNP and upper-GNP—with the native-born as the reference group (0). See Table 1 in the online appendix for the distribution of origin-countries by the level of GNP.
Next, the age at immigration was used to create four life-stage at immigration groups (immigration at or before the age of 15 [childhood], between 16 and 24 [late teens/early-adulthood], between 25 and 34 [mid-adulthood], and after 35 years of age [later-adulthood]) with the native-born as the reference group (0). The decision on the current categorization of life-stage at arrival are based on the work of Rumbaut (2004) for the adults and empirical reasons for the categorization of those who migrated before the age of 18. 1 Finally, information on GNP and the life-stage at immigration were used to create a dummy variable indexed with eight categories: Upper-GNP immigrants who immigrated in childhood (N = 143), late teens/early-adulthood (N = 78), mid-adulthood (N = 84), and later-adulthood (N = 25); and lower-GNP immigrants who immigrated in childhood (N = 81), late teens/early-adulthood (N = 85), mid-adulthood (N = 99), and later-adulthood (N = 84). The Canadian-born are the reference group (N = 1,478).
Because the native-born do not have a value for length of residence (LOR), this variable is coded conditionally on foreign-born status (see Ross and Mirowsky 1992 for a detailed discussion) to allow for the inclusion of the native-born in the analyses. This method treats LOR as a conditional deviation score from the grand-mean of LOR. Conditionally coding allows for a test of the HIE by allowing for the comparison of each GNP/life-stage at immigration group (at the average level of LOR in the sample) to the native-born, while simultaneously representing the effects of LOR only for those who are foreign-born.
In its simplest form, this conditionally relevant variable appears in a regression model as follows:
For the native-born (Foreign = 0) respondents who do not have a value for LOR, distress equals b0. For those who are foreign-born (= 1), distress scores vary with LOR. In these analyses, the effect of LOR is subdivided by GNP and life-stage at immigration for the foreign-born, instead of a single variable representing foreign-born.
Chronic Stressors is an index created from a total of 40 items (Wheaton 1997) and measures chronic stressors across a number of roles and environments (see Table 2 in the online appendix for specific items). This index is calculated using the mean of the total number of stressors respondents indicated experiencing at the time of the interview, including personal, relationship, parenting, employment, financial, and ambient stressors, adjusted by the number of questions that the respondent could potentially answer, depending on occupied roles. If someone is not a parent, therefore, parental items are missing, and cannot count overall. This approach protects the variation in reported chronic stress from being confounded with the number of occupied roles (Turner, Wheaton, and Lloyd 1995). Respondents were asked whether a number of situations are “not true,” “somewhat true,” or “very true” for them currently. Higher scores indicate greater chronic stressors.
The average of three items adapted from the work of Noh and Avison (1992) and asked only of the foreign-born is used to create an index of failed expectations. These respondents were asked to indicate how often “[they] feel that living in Canada is stressful because”: “I have a job in Canada that is below my experience and qualifications” (coded as missing for the unemployed), “the education I obtained in my country of origin/or another country prior to coming to Canada is not recognized here,” and “I am disappointed that my standard of living is not what I had hoped for when I first came to Canada.” Response options include, never (1) to very often (4). Higher values indicate grater failed expectations (α = .87). As with LOR, this index is coded conditionally on foreign-born status to allow for the inclusion of the native-born in the analyses.
The analyses adjust for a number of covariates since group differences in these characteristics may contribute to health disparities between immigrants and the native-born (Cavazos-Rehg, Zayas, and Spitznagel 2007; House 2002; Montazer and Wheaton 2017; Montazer and Young 2017; Noh et al. 1999; Riosmena et al. 2013; Turner et al. 1995). For example, research shows that areas with higher number of co-ethnics might be more likely to provide practical resources and information to facilitate the settlement process of immigrants, which has important consequences for their mental health (Stafford, Newbold, and Ross 2011). However, a comprehensive model of immigration must also account for possible suppressors, or protective factors—such as SES and social support—(Beiser 2004) that may make the association between an independent (i.e., LOR) and dependent variable (distress) apparent or stronger when included in the model (Schieman 2009).
Gender is coded 1 for women. Respondent age is modeled as a five category dummy variable to reflect its possible nonlinear effect (O’Campo et al. 2015). The categories include younger than 30 years of age, 30–39, 40–49, 50–59, and those above 60 (as the reference group). Marital status is a dummy variable that is coded as 1 if the respondent is married or common-law and 0 otherwise. Number of children in the household is a continuous variable that takes the count of total number of children under the age of 18 living with the respondent. Total number of negative life events takes the count of 18 negative life events (see Table 2 in the online appendix for specific items) experienced by the respondent at any time in his/her life (Turner et al. 1995). Parental education is a continuous variable operationalized as the total number of years of education of the more educated parent. Limited English language speaking ability is coded 1 for those indicating limited English language speaking ability versus those who indicated being proficient (0). Immigration entrance category is a dummy variable with three categories: work-visa, landed immigrant (a non-Canadian citizen permanent resident), versus all other respondents as the reference category.
Ethnicity/culture is a dummy variable indexed with eight categories: Arab or West Asian, African, Caribbean, South Asian, East Asian Pacific Rim, Latin, European, with North American/Canadian ethnic/cultural identity as the reference category. These categories were created from the standard Statistics Canada ethnicity coding (Statistics Canada 2008).
To measure the percent of residents with same ethnicity as the respondent (% Ethnic same), 14 separate ethnic groups—based on Statistics Canada classifications used in the 2006 Census (Statistics Canada 2008)—were used to create a percentage-measure to account for the number of people in the census tract who match the ethnicity of the respondent (the latter based on self-reports). This measure is considered an individual-level measure, since the value varies by individual rather than by census tract. Residents not included in these percentages are considered dissimilar from the respondent on that particular feature.
The analyses also adjust for premigration human capital: premigration education and years of employment tenure. These are particularly relevant to those who came to Canada as adults and are criteria for admission to Canada under the points system (selection). As with LOR, the total number of years of education and the total number of years worked for pay before coming to Canada are conditional on foreign-born status.
Suppressors used in the models are perceived social support and three variables that tap at SES: employment status (= 1 for employed), household income—a continuous variable that ranges between $4,800.00 and $800,000.00, and home ownership (= 1 for home owner). Perceived social support is captured with an index that takes the average of 16 items from the Medical Outcomes Study (MOS) Social Support Survey (Sherbourne and Stewart 1991). Respondents were asked how often (None of the time [1], A little of the time [2], some of the time [3], most of the time [4], or all of the time [5]) different kinds of support are available to them. Some examples include “someone who shows you love and affection” or “someone to do something enjoyable with.” Higher values indicated greater perceptions of social support (α = .96).
Statistical Analyses
The NEHW study unavoidably clusters respondents by neighborhood and, thus, error terms across respondents within the same neighborhood are likely correlated. To address clustering concerns and to separate the variance in outcome across neighborhoods (Level 2) as a proportion of the total variance in each outcome (Level 1), all multivariate analyses used hierarchical linear modeling (HLM; Raudenbush and Bryk 2002). All variables were grand-mean centered (Raudenbush and Bryk 2002), making the intercept interpretable at the mean value of the predictor variables. Grand-mean centering also helps with avoiding collinearity among predictors (Y.-W. B. Wu and Wooldridge 2005). All analyses were weighted by gender, age, household income, household size, and nativity. Multiple imputation methods, with five data sets imputed, were used to replace missing values on control variables (Little and Rubin 1987). 2
Table 1 presents unweighted sample characteristics by GNP of origin-country and the life-stage at immigration for all the study variables. Significant difference at the bivariate level between the different immigrant groups and between each immigrant group and the native-born were tested using chi-square test for categorical variables and analysis of variance (ANOVA; Bonferroni post hoc) for continuous variables. To test the study hypotheses, Table 2 presents multivariate results, which assess the impact of GNP/life-stage at immigration by LOR on psychological distress. Results of post hoc tests are used to indicate significant differences in distress between different GNP/life-stage at immigration groups. Unadjusted results of the effect of GNP by LOR are presented in Model 1; Model 2 presents unadjusted results of GNP and life-stage at immigration by LOR; controls and suppressors are added in Model 3; failed expectations is added in Model 4; and finally, Model 5 is additionally adjusted for chronic stressors. Mediation effects are assessed using the three-pronged approach outlined by Baron and Kenny (1986). Thus, Table 3 presents results for the effects of GNP/life-stage at immigration, and LOR on the potential mediators.
Descriptive Statistics for All Variables in the Study (Unweighted).
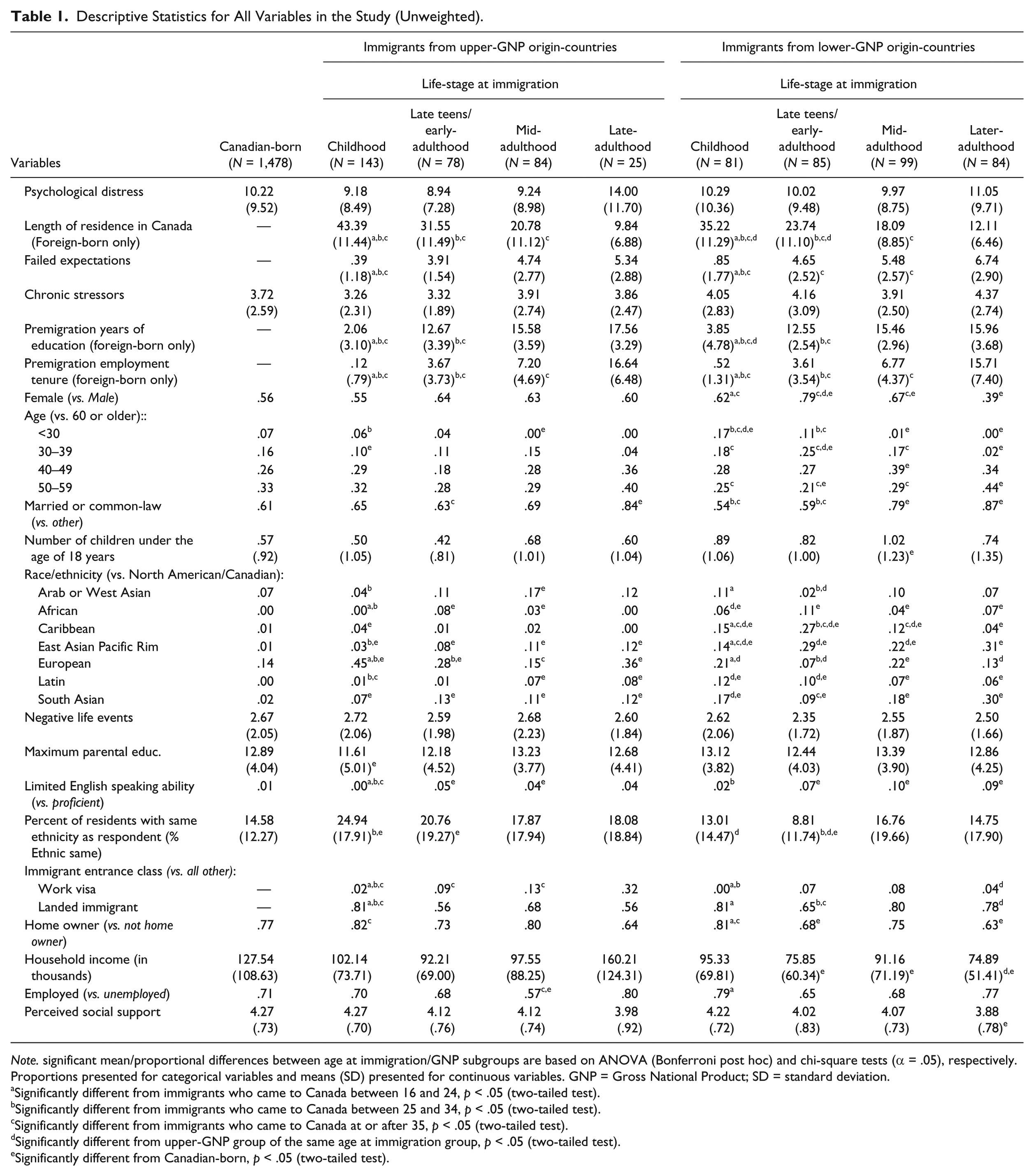
Note. significant mean/proportional differences between age at immigration/GNP subgroups are based on ANOVA (Bonferroni post hoc) and chi-square tests (α = .05), respectively. Proportions presented for categorical variables and means (SD) presented for continuous variables. GNP = Gross National Product; SD = standard deviation.
Significantly different from immigrants who came to Canada between 16 and 24, p < .05 (two-tailed test).
Significantly different from immigrants who came to Canada between 25 and 34, p < .05 (two-tailed test).
Significantly different from immigrants who came to Canada at or after 35, p < .05 (two-tailed test).
Significantly different from upper-GNP group of the same age at immigration group, p < .05 (two-tailed test).
Significantly different from Canadian-born, p < .05 (two-tailed test).
Effects of Level of Economic Development of Origin-country by the Life-stage at Immigration, and Length of Residence in Canada on Distress (N = 2,157).
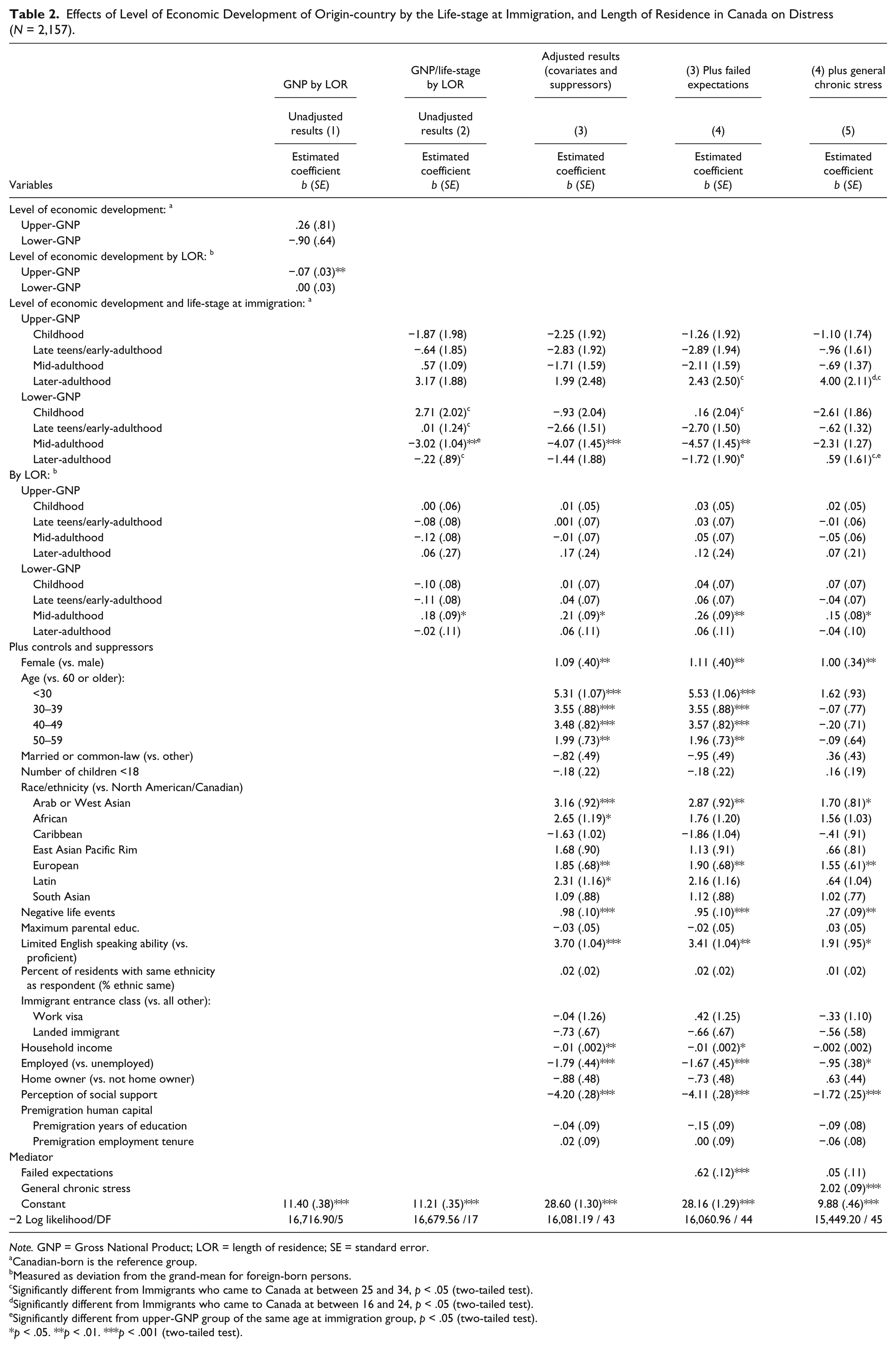
Note. GNP = Gross National Product; LOR = length of residence; SE = standard error.
Canadian-born is the reference group.
Measured as deviation from the grand-mean for foreign-born persons.
Significantly different from Immigrants who came to Canada at between 25 and 34, p < .05 (two-tailed test).
Significantly different from Immigrants who came to Canada at between 16 and 24, p < .05 (two-tailed test).
Significantly different from upper-GNP group of the same age at immigration group, p < .05 (two-tailed test).
p < .05. **p < .01. ***p < .001 (two-tailed test).
Effects of Level of Economic Development of Origin-country by the Life-stage at Immigration, and Length of Residence in Canada on Failed Expectations and General Chronic Stress.
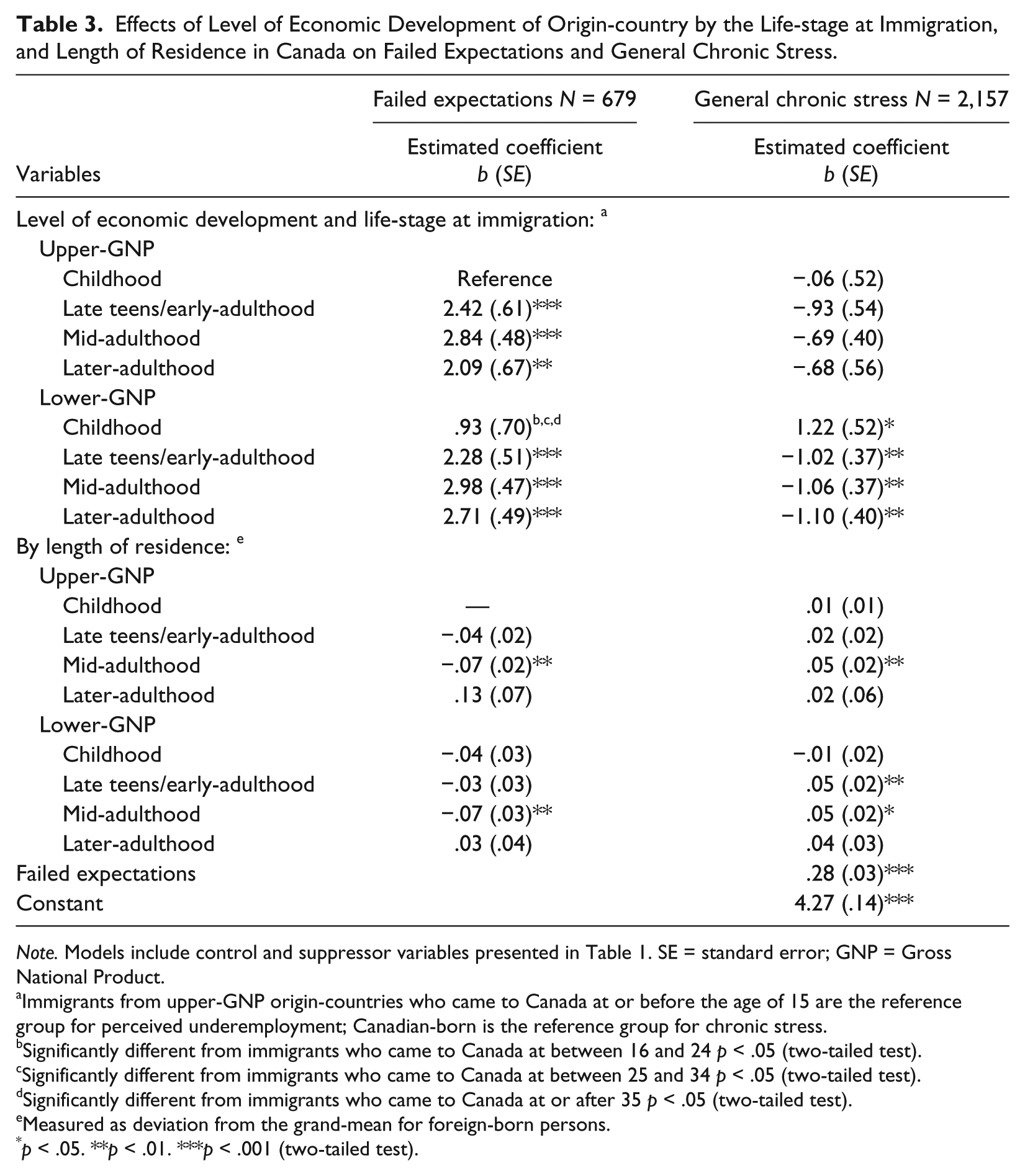
Note. Models include control and suppressor variables presented in Table 1. SE = standard error; GNP = Gross National Product.
Immigrants from upper-GNP origin-countries who came to Canada at or before the age of 15 are the reference group for perceived underemployment; Canadian-born is the reference group for chronic stress.
Significantly different from immigrants who came to Canada at between 16 and 24 p < .05 (two-tailed test).
Significantly different from immigrants who came to Canada at between 25 and 34 p < .05 (two-tailed test).
Significantly different from immigrants who came to Canada at or after 35 p < .05 (two-tailed test).
Measured as deviation from the grand-mean for foreign-born persons.
p < .05. **p < .01. ***p < .001 (two-tailed test).
Results
Unweighted bivariate results presented in Table 1 indicate that, contrary to the predictions of the HIE, there are no significant differences in average distress among the various groups. However, average failed expectations is significantly lower among immigrants who came to Canada in childhood, irrespective of GNP as compared to other life-stage at immigration groups of the same GNP. While there are no significant group differences in average chronic stress, lower-GNP immigrants who came to Canada in childhood report significantly higher average chronic stress (p < .10, two-tailed test; difference not shown in table) than their upper-GNP counterparts (Low GNP:
GNP/Life-stage at Immigration, LOR, and Psychological Distress
As can be seen in Model 1(unadjusted results) of Table 2, and contrary to the predictions of the first hypothesis, there are no significant differences in distress between either of the GNP groups, at average LOR, and the native-born. Furthermore, while the increase in LOR does not have a significant effect on distress among lower-GNP immigrants, increase in LOR tends to decrease distress among those from upper-GNP origin-countries. Model 2 tests the second hypothesis. As predicted, distinction by level of economic development alone is not enough—the HIE and the ensuing decline in distress with time in Canada varies by the level of economic development of immigrant’s origin-country and the life-stage at migration. This model improves significantly on Model 1. At average LOR in Canada, only immigrants from lower-GNP countries who came to Canada in mid-adulthood benefit from a HIE. This group has significantly lower distress than all other lower-GNP immigrants, the Canadian-born, and upper-GNP immigrants who came to Canada in mid-adulthood. The results of this model also show how the association between each GNP/life-stage at immigrating group and distress changes with one-year increment in LOR. The effect of LOR is positive and significant only among those who migrated in mid-adulthood from lower-GNP origin-countries. This significant positive coefficient suggests that each year increase in LOR increases distress by .18 among this group of immigrants. These results persist with the addition of controls and suppressors in Model 3. Indeed, the HIE among this group of migrants becomes even stronger (mainly because of the suppressors) in the adjusted model and is now evident among lower-GNP mid-adulthood immigrants in relation to only the native-born. The results for these last two models provide support for H2 and H3. To assess whether the increase in distress with time is due to an increase in failed expectations (H4a), this variable is added next. However, contrary to predictions, the addition of this variable suppresses the relationship between LOR and distress among immigrants who migrated in mid-adulthood from lower-GNP countries. Finally, to test H4b, chronic stressors are added to Model 5. The inclusion of this variable reduces the coefficient for the effect of LOR on distress among this group of migrants by 42 percent (.26 – .15 / .26 × 100).
Interestingly, while the HIE among this group (at average LOR) is reduced to nonsignificant, the addition of chronic stressors suppresses the effect of having immigrated in later-adulthood from an upper-GNP origin-country on distress. This later group reports significantly higher distress than their mid-adulthood counterparts from upper-GNP countries and their lower-GNP counterparts who immigrated during the same stage of the life-course.
GNP/Life-stage at Immigration, LOR, Failed Expectations, and Chronic Stress
To better understand the role of mediators, Table 3 presents adjusted results intended to evaluate (1) the impact of GNP/life-stage at immigration by LOR on failed expectations, and (2) chronic stressors, controlling for failed expectations. Since a sense of failed expectations is only measured among the foreign-born, the adjusted results for this variable as outcome are restricted to the foreign-born only. Failed expectations is on average higher among all of the immigrant groups (at average LOR) as compared to those who migrated in childhood from upper-GNP countries. Child immigrants from lower-GNP countries have the same average levels of failed expectations than their upper-GNP counterparts and lower average failed expectations than their adult counterparts from lower-GNP countries. Despite the higher average failed expectation among adult immigrants, and contrary to the predictions of H4a, experience of failed expectations tends to decrease with LOR among immigrants who migrated in mid-adulthood, irrespective of GNP. As can be seen in the second column of this table, failed expectations tend to increase chronic stressors (b = .27, p < .001; stress proliferation) and chronic stressors are, on average, lower among adult immigrants from lower-GNP countries as compared to the native-born. Child immigrants from lower-GNP countries report higher (not the same) average chronic stressors than the native-born. Chronic stressors increase with each additional year in Canada among some GNP/life-stage at immigration groups: namely, lower-GNP immigrants who came to Canada in their late teens/early-adulthood and lower and upper-GNP immigrants who migrated in mid-adulthood. The results of this table in conjunction with those reported in Models 4 and 5 of Table 2, provide support for H4b but do not fully support the predictions of H4a: while increase in failed expectations tends to increase chronic stressors, immigrants from lower-GNP countries who migrated in mid-adulthood experience a decrease (not an increase) in failed expectations with time in Canada.
Discussion
By using data out of Toronto, a city with a population that consists of almost 50 percent immigrants (O’Campo et al. 2015), the current article found evidence for the commonly reported HIE in mental health but with one important qualification: only immigrants from lower-GNP origin-countries who migrated in mid-adulthood experienced a HIE in psychological distress, at average LOR in Canada, as compared to the native-born. This was also the only group that experienced an increase in distress with time in the host-country. A parallel increase in chronic stressors, despite a decline in failed expectations, with time in the host-country among this group of immigrants partly explained the effect of LOR on psychological distress. As predicted, immigrants from developed origin-countries, irrespective of the life-stage at immigration, did not experience a mental-health advantage or an eventual decline in mental health with tenure in the host-country. This group of immigrants in general migrate from countries with similar life outcomes—in terms of income and quality of life—that may minimize the health effects of migration between developed countries (Urquia, Frank, and Glazier 2010). The findings here compliment the predictions of segmented assimilation theory (Portes and Zhou 1993) that there are various patterns of psychosocial adaptation that depend on an individual’s characteristics. While this theory was originally developed to better understand second generation racial/ethnic minorities’ path toward integration into the American society, the results here suggest that there are also various patterns of psychosocial adaptation among adults migrating to other contexts—that is, Canada—that are conditional on the life-stage at immigration and the level of economic development of the origin-country at the time of migration (Montazer and Wheaton 2011, 2017).
Healthy Immigrant Effect and Distress
The emotional health advantage among immigrants has been attributed to selection factors at the individual and host-country levels (Kennedy et al. 2015). This article argued that health selection should be highest among immigrants from lower-GNP countries, particularly those who migrated in mid-adulthood, because these immigrants generally immigrate after having completed their education, at the beginning of their work careers, and in their peak childbearing and family-formation years (Rumbaut 2004)—all important variables in Canada’s immigrant selection process. While results indicate the HIE to only be evident among lower-GNP immigrants who came to Canada in mid-adulthood, the data do not provide support for the assertion that this HIE is due to selection since the gap in distress continued to be present despite adjustment for possible selection, as well as other factors. Selection on such measurable factors, therefore, may not be the only reason for the lower rate of distress among this group of immigrants in the sample. Furthermore, unlike the assertion that immigrants from lower-GNP origin-countries are more selected by the host-country than those from developed countries (Jasso et al. 2004), “lower-GNP” adult immigrants did not have higher years of education or work experience than their counterparts who migrated from upper-GNP countries during the same stage of the life-cycle (Table 1).
Similar to results reported in previous work using national-level panel data (Montazer and Wheaton 2017), multivariate results indicate that the observed HIE among mid-adulthood lower-GNP immigrants is in large part due to fewer chronic stressors (at average LOR) among this group, as compared to the native-born. This finding, although counterintuitive, may be due to unobserved selection criteria of immigrants from the most socioeconomically distant countries of origins, such as perseverance in the face of adversary and being forward-looking (Kennedy et al. 2015). These factors may either help these immigrants to overcome or combat chronic stressors, or not to view life conditions (such as financial problems) as stressful because they are still better off than those family and friends left behind (Montazer, Wheaton, and Noh 2016), leading to lower psychological distress in this group. Of course, it is also possible that immigrants, especially those from the most distinct origin-countries, either express mental-health problems with different symptoms than are asked here or are more motivated to hide problems (Montazer and Wheaton 2017). However, psychological distress—measured with similar questions used in the construction of the current psychological distress scale—has been used in numerous studies in many countries (in diverse languages) for the World Mental Health Survey (Wu et al. 2003). Thus, this possibility is likely to account for a small portion of the variation in distress. Nonetheless, future scholarship should extend the current research to consider additional mental-health outcomes.
Failed Expectations, Length of Residence and Distress
This article argued that despite the potential higher selection (on observable or unobservable factors) among immigrants from lower-GNP countries, this group should experience a steady increase in the sense of “failed expectations” with time in Canada, which should lead to an increase in other chronic stressors (stress proliferation), and psychological distress as a consequence. According to Shibutani and Kwan (1965), a reduction in social distance precedes and stimulates economic advancement and structural assimilation. It is thus natural that as time in the host-country increases, perception of social distance should decrease. Research has shown, however, that even with time in the host-country immigrants from less developed origin-countries continue to be underemployed (Galarneau and Morissette 2008). While recent immigrants from lower-GNP countries might accept that their lower economic standing, for example, is due to the fact that they are from countries that are fundamentally different in opportunity structure—that is, education system—than that of the developed host-country, this acceptance will likely decrease as tenure in the host-country increases, perception of social distance decreases, and the immigrants comparison group shifts from other co-ethnics to the dominant group (Hurh and Kim 1990). With increase in time in the host-country, immigrants from lower-GNP countries, particularly those who came to Canada at the most forward-looking time of the life-course—mid-adulthood—were predicted to have a harder time accepting being underemployed, for example, because of the lower return to skills and education obtained in less developed origin-countries (Bratsberg and Ragan 2002), leading to greater relative deprivation (Hurh and Kim 1990) or, as conceptualized here, a general sense of “failed expectations.”
However, while “failed expectations” were generally higher among all immigrants as compared to those who migrated in childhood from the same GNP origin-countries (Table 3), it decreased with tenure in Canada among those who migrated in mid-adulthood, irrespective of GNP. Indeed, failed expectations suppressed the effect of LOR on distress among mid-adulthood migrants from lower-GNP origin-countries suggesting that a decline in this feeling with time in Canada is protective against the experience of distress. It appears that at least in this sample, LOR is associated with betterment in life conditions and a decline in failed expectations among these immigrants.
Chronic Stressors, Length of Residence and Distress
Another proposition of this article was that the decline in mental health with time in the host-country would in part be due to an increase in general chronic stressors (Cook et al. 2009; Montazer and Wheaton 2017). The analyses did not find support for the mechanism—that is, failed expectations—linking chronic stress to distress among lower-GNP immigrants who migrated in mid-adulthood. But, a parallel increase in chronic stressors uniquely mediated a large percentage of the effect of LOR on distress among this group, despite the protective effect of a decrease in failed expectations with tenure in Canada.
What could be the reason for the increase in chronic stressors with time in the host-country among mid-adulthood immigrants from lower-GNP origin-countries? One reason may be that this group of migrants is more likely to find a partner and have children in the host-country (Rumbaut 2004). The 2.5 generation children born to one parent from a less economically developed origin-country and one Canadian-born parent have been found to be more likely to experience mental-health problems because of difficulties experienced by these children in both the private and public spheres (Montazer and Wheaton 2011). Thus, stressors concerning child mental health and family stressors among those with a partner and/or children due to dissonant acculturation may be especially prevalent among this group of immigrants where the “tug of war” between family members may be clearest (Montazer and Wheaton 2011). Other studies have attributed the increase in mental-health problems to an increase in perceived discrimination (Cook et al. 2009). While the chronic stress scale used here does not measure perceived discrimination directly, it might be tapping into this indirectly through stressors in work, neighborhood, and financial spheres. However, lower-GNP immigrants who migrated in mid-adulthood were not the only group that experienced an increase in chronic stressors with time in Canada, as mid-adulthood immigrants from upper-GNP immigrants also experienced an increase in general chronic stressors with time in the host-country. It may be, however, that the specific chronic stressors experienced by these two groups are fundamentally different. 3 Future research should examine the mediating effects of specific stressors in the relationship between LOR and distress among migrants.
Future Research and Limitations
Future research should also examine the effect of economic development of origin-country and life-stage at immigration on distress in conjunction with membership in other statuses that the individual may hold, including gender, religion, social class, and English language proficiency (Brondolo et al. 2015). The sample of immigrants in the current study was too small to allow for such distinctions. An alternative finding that needs to be explored in future work is whether the observed patterns are due to the region of origin of the immigrants in the sample. The current analyses adjusted for ethnicity to control for differences across GNP that may be due to ethnicity. Furthermore, auxiliary analyses not shown (but available) controlled for region of origin and the main findings remained, which confirms the robustness of the association between economic development, life-stage at immigration, and distress postarrival. Research should examine the effect of immigration from different regions of origin conditional on the level of economic development within region and life-stage at immigration as a further distinction. Again, the sample of immigrants here was too small to allow for this type of categorization.
The current study is limited in several ways. First, the analyses are based on cross-sectional data and cannot address issues of causal order for relationships between mediators, some controls/suppressors (i.e., perceived social support, negative life events), and outcomes. Second, while the analyses control for one macrolevel contextual factor at the time of emigration—GNP—and migration entrance category, they do not account for all of the pull or push factors in the migration process that may determine the migratory forces unique to any year of arrival, such as the political and legal conditions (Jasso et al. 2004) in origin-countries. Third, participation in this study required respondents to have reasonable skills in English and to have lived in their neighborhood for at least six months. These restrictions may have attributed to the overrepresentation of more established immigrants in the sample who have, for the most part, overcome the most difficult phase of adjustment, which may have underestimated the effect of LOR on distress among some groups. The analyses, however, included individual-level sample weights to ensure that the sample was representative of the census tracts from which the participants were drawn (O’Campo et al. 2015). Finally, it is necessary to replicate these analyses with a larger sample of migrants to Canada. It may be, for example, that nonsignificant results observed among some groups, such as the later-adulthood upper-GNP group of immigrants, are due to small numbers in these groups.
The benefits of the current study, however, outweigh the above noted limitations. This scholarship provides evidence that the HIE in psychological distress is not universal. It is dependent on the economic context of the origin-country and the stage of the life-course at migration. Only those from the most economically distant origin-countries who left the life they knew in mid-adulthood benefit from a HIE. This is also the group that experiences a decline in mental health with tenure in the host-country in large part because of a parallel increase in chronic stressors over time.
Supplemental Material
Online_Appendix_updated – Supplemental material for Economic Development of Origin-countries, Life-stage at Immigration, and Length of Residence Effects on Psychological Distress
Supplemental material, Online_Appendix_updated for Economic Development of Origin-countries, Life-stage at Immigration, and Length of Residence Effects on Psychological Distress by Shirin Montazer in Social Currents
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Canadian Institutes of Health Research (CIHR) Grant MOP-84439 and the Social Sciences and Humanities Research Council (SSHRC) Grant 410-2007-1499 (Blair Wheaton, Patricia O’Campo, PIs).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.