
Abstract
Effective and comfortable provider-patient communication is associated with engagement in health-promoting behavior. Although research on medical experiences among sexual minorities has increased, work has not examined how gender intersects with sexual identity to shape medical experiences. Using an intercategorical intersectional approach, we examine whether sexual minorities perceive their medical provider as knowledgeable and comfortable with their sexual identity, and how these relationships differ for cisgender men, cisgender women, and multigendered transgender adults. Drawing on data from 3,050 adults included in the 2010 Social Justice Sexuality Project, logistic regression models show three main findings. First, compared with heterosexual cisgender women, bisexual cisgender women are less likely to perceive that their provider knew their sexual identity—and if they did perceive knowledge, they were less likely to perceive that their provider was comfortable with their sexual identity. Second, gay transgender adults have significantly lower odds of perceiving provider comfort with their sexual identity relative to heterosexual transgender adults. Finally, for each gender group, our models demonstrated the importance of medical and social relationships for perceiving both knowledge and comfort with sexual identity from medical care providers.
Introduction
Open and honest communication with medical providers is important for a comfortable and positive experience that provides individuals with valuable health knowledge, including information about the importance of preventive medical services that may reduce morbidity and improve overall quality of life (Garcia, Lechuga, and Zea 2012). Despite the importance of medical care services, in 2011 the Institute of Medicine (IOM) concluded that in comparison with heterosexuals, sexual minorities have more limited access and interaction with medical care professionals. They also concluded that more work is needed detailing how medical care experiences vary across specific sexual orientation groups. Understanding of how gender identity shapes the medical encounter for sexual minorities is lacking, with limited research providing contradictory results that often fail to address how medical experiences differ by gender identity and sexual orientation.
This study contributes to existing scholarship on medical experiences among sexual minorities by examining the intersections of gender and sexual identity rather than focusing on one identity status to the exclusion of the other. Given the salience of gender identity for shaping conceptions of self (Butler 1999; Connell 2005), and growing recognition that gender is not a binary and is a separate construct from sexual orientation (Fein et al. 2017), it is important to explore how medical interactions vary for persons across different intersections of gender and sexual identity. We use an intercategorical intersectional approach (McCall 2005) and draw on data from 3,050 adults included in the 2010 Social Justice Sexuality Project (SJSP) to examine differences in perceived provider comfort with sexual identity. By focusing on the specific intersections of gender identity and sexual orientation, we avoid the assumption that the experience of perceiving medical providers as uncomfortable with their sexual identity is broadly similar for all sexual minority adults, for cisgender and transgender adults. Sexual orientation is just one of many identity characteristics, and intersectional perspectives are needed in health research if we are to close gaps in the quality of medical care experiences that exist between sexual minority and heterosexual adults (IOM 2011).
Indeed, by differentiating between self-identified heterosexual, gay, lesbian, bisexual, and alternatively defined individuals among cisgender men, cisgender women, and multigendered transgender individuals, 1 we expand examination of the medical care experience to specific gender and sexual identity populations that are underexamined in health research. In other words, we move beyond the simplistic assessments of medical care experiences that examine “all” sexual minorities or focus only on one group to a more nuanced understanding of how experiences differ between cisgender bisexual men, transgender heterosexuals, and others. In this way, we provide needed information on the necessity of tailoring health policies to the unique experiences of specific population groups. More generally, by examining differences in provider-patient communication, we can get a sense of the inequalities that exist in medical encounters for groups in need of positive medical experiences. Studies show that delayed care has economic consequences for our health care system (IOM 2015). Indeed, estimates suggest that reducing disparities in medical care use would save the $230 billion over three years, making examinations of disparities of quality of care, like ours, fiscally important (LaVeist, Gaskin, and Richard 2006; Squires 2015).
Another contribution of our study is that we evaluate whether adjusting for demographic characteristics, socioeconomic status, health care access and utilization, and social support reduces differences in reported comfort across gender and sexual identity groups. Past work has identified barriers in accessing health care as well as higher rates of physical and mental health problems among lesbian, gay, bisexual, and transgender (LGBT) adults (Gay and Lesbian Medical Association 2001). Our study examines whether there are certain health-promoting resources that are positively associated with perceiving provider comfort with sexual identity across gender and sexual identity groups. This perspective is useful because intersectional scholarship should not only emphasize differences found across identity groups but also examine similarities among them. By underscoring the positive associations of certain health-promoting resources across cisgender and transgender men and women, this study avoids depicting minorities as solely negatively affected by social factors and provides information that can be used in promoting better quality of medical care among adults.
Background
An Intersectional Framework
For some time now, scholars have argued and demonstrated that the intersectional position one holds affects life chances and experiences (Crenshaw 1991). Drawing from feminist and critical race theory, intersectionality as a theoretical approach highlights how the multiple identities individuals maintain produce different experiences across social locations (Collins 1999). This approach emphasizes interlocking processes of privilege and constraint in producing varying experiences across social groups (Bauer 2014). Early intersectional theorists, including Crenshaw (1991) and Collins (1999), proposed using an intersectional approach to examine issues of inequality. As a theoretical approach and a methodology, intersectionality offers great potential for examining inequality in health contexts, particularly as it relates to including formerly excluded individuals (Choo and Ferree 2010).
In this article, we examine how perceived comfort from medical providers differs across the intersections of sexual and gender identity. 2 Studies that fail to examine the diversity of sexual identity groups by focusing on aggregated “sexual minorities” rather than separate groups reinforce heteronormative and exclusionary identity categories (Fausto-Sterling 1993). In addition, studies that focus on cisgender men and cisgender women but not transgender adults neglect the continuum that we see in both sex and gender expression (Connell 2005). Failing to examine all social locations frames normative behavior as what people do instead of examining who the people are who are doing these behaviors. By examining the experiences of cisgender men and heterosexuality as intersectional positions in this study, we avoid leaving dominant identities unexamined while reifying them as normative and other identity categories as deviant (Carbado 2013).
Existing scholarship documents the vulnerable health status of sexual and gender minorities (Conron, Mimiage, and Landers 2010), yet little work has considered how medical care experiences differ across intersections of gender and sexual identity. Although more commonly used in qualitative research, an intersectional framework is also applicable to quantitative studies that analyze relationships of inequality among social groups (McCall 2005). Recent years have seen various scholars and health organizations calling for intersectional approaches in population health studies (IOM 2011).
Gender Identity, Sexual Identity, and Medical Care Experiences
Research on health care utilization emphasizes the importance of quality of medical interaction due to the changing role of patients as more engaged and providers as more collaborative in treatment strategies (Boyer and Lutfey 2010). Satisfaction with care is positively correlated with adherence to treatment (IOM 2015), but varies across gender identity and sexual orientation (Conron et al. 2010). Given the link between quality of care and health care utilization (IOM 2015), it is imperative to examine experiences of vulnerable populations with high health risks as this can improve the effectiveness of health intervention programs, provide valuable information to researchers, and reduce medical care costs. At the same time, scholarship examining whether variation exists in medical encounters across specific sexual identity groups is needed (IOM 2011).
There is evidence of disparities in the medical encounter across various axes of identity (Peck and Denney 2012). Rates of satisfaction with medical experiences and provider interaction vary across gender and sexual orientation, with minorities reporting less satisfaction and poorer quality of care (Boyer and Lutfey 2010). Reasons for poorer perceived quality of care among sexual minorities include discomfort in medical contexts due to quality of the patient-provider relationship, lack of ease of communication with providers, and fear of discrimination (Jenerette and Mayer 2016). In addition to individual level barriers, such as homophobia or provider discomfort, scholars also point to barriers at the institutional level (IOM 2011) that contribute to a lack of access to adequate quality medical care among sexual minorities (e.g., a limited number of available providers that are knowledgeable about lesbian, gay, bisexual issues).
Research on the medical experiences of sexual minorities emphasizes the importance of comfortably disclosing sexual orientation for a positive medical encounter (Daley 2012). Yet, despite the documented link between disclosure of sexuality and safe sex discussions among sexual minorities, various studies present low rates of self-disclosure of sexual identity to medical providers due to fear of discrimination and heterosexual assumption (Meyer 2007; Sinclair 2006), which contributes to less satisfaction with quality of care among sexual minorities (Sherman et al. 2014). Lower satisfaction of medical care services, which is shaped by patient experiences, has also been shown to contribute to lower adherence to recommended health care, fewer preventative care visits, and overall lower utilization of medical services (IOM 2015). For many individuals, disclosing their sexual orientation to their medical provider forces them to “come out,” which can produce uncomfortable and potentially negative experiences (Brotman et al. 2002). Given that an accurate sexual history assists providers in supplying effective treatment, nondisclosure can hinder effectiveness of medical encounters through diminished patient-provider communication and low utilization rates of services. Timely delivery of medical care is vital to adult well-being and studies show that delayed care due to unsatisfactory medical experiences is associated with morbidity, mortality, and poorer overall quality of life, making examinations of quality of care pertinent to public policy and population health (IOM 2015).
Despite evidence of gender differences in health care utilization, there is limited information about differences in the quality of the medical interaction across gender identity (Tabenkin et al. 2004). Studies have found that cisgender women are more critical of provider-patient relationships (Green and Pope 1999), and as a group are in poorer economic standing than cisgender men (Kramer et al. 2012). Yet, cisgender women also tend to have higher rates of concern with their health, higher rates of utilization of health care services, and more willingness to engage in health-promoting behavior (Koopmans and Lamers 2006). In addition, studies that compare medical experiences of cisgender men and women report differences in the context and content of the interaction, with more time devoted to preventive screening for women while more time is devoted to counseling about health behavior for men (Tabenkin et al. 2004).
While limited, studies on health care utilization of gender minorities (those who identify in non-cisgender categories) document high rates of harassment and discrimination related to their gender identity (Noonan et al. 2018). In terms of medical experiences, gender minorities report difficulty in navigating insurance paperwork as well as choosing a knowledgeable health provider (Johnson, Mimiage, and Bradford 2008). As patients, gender minorities report uncomfortable medical experiences due to the insensitivity of medical providers about their bodies and medical history along with the use of incongruent gendered language during medical interactions (Tangpricha et al. 2016).
More broadly, these experiences relate to cisnormativity in society and the lack of education in medical curriculum on transgender medical needs (Safer et al. 2016). Financial barriers as well as increased rates of discrimination also shape access to quality medical care for transgender persons (Lombardi 2010). Recent work by Gonzalez and Henning-Smith (2017) shows that transgender adults are more likely to be uninsured due to legal hurdles associated with their gender transition—and that even when they are covered, many plans do not cover transition-related services. As a result, many transgender adults pay for services out of pocket, which can range from $100 a month to over $100,000 for some procedures. This lack of adequate insurance coverage, along with lower educational attainment and household income relative to cisgender adults, are structural barriers that negatively affect their quality of medical care.
Research on health disparities among sexual minorities document barriers to adequate health care, unmet medical needs, and poorer health status (Bonvicini and Perlin 2003). Although studies have shown that gender identity influences the medical care experience, intersectionality theory leads us to posit that it also conditions the manner in which these experiences differ by sexual orientation. In using an intersectional framework, we not only examine the experiences of individuals with multiple disadvantaged statuses but also examine how the coupling of advantage and disadvantage shapes perceptions of comfort. Although studies indicate varying levels of social and economic disadvantage across gender and sexual orientation groups, in using an intersectionality framework we expect that people who hold multiple disadvantaged statuses would report the lowest rates of perceived comfort because those with the least amount of privilege encounter the highest levels of inequality. For example, we would expect that cisgender men and women, regardless of sexual identity, would report higher levels of perceived comfort relative to multigendered sexual minority transgender adults.
In addition, by examining the confounding role of socioeconomic factors, health care utilization and social support on perceptions of comfort, our study also avoids centering the analysis solely on membership in identity categories.
Although studies that address how both gender and sexual orientation influence the medical encounter are limited, single analysis studies suggest differences in comfort across gender identity (Krawsoski, Gupta, and Imborek 2016). Research on the medical experiences of lesbians suggests that low internalized homophobia in women, as well as their likelihood to maintain more supportive networks, may contribute to more positive medical experiences (McNair, Hegarty, and Taft 2012). Among gay men, studies suggest a preference for other forms of medical services due to a desire to seek nonjudgmental and knowledgeable care (Koester et al. 2013). Gender differences in the medical encounter produced from gendered expectations about health behaviors in addition to the higher utilization rates of cisgender women may contribute to their more comfortable experiences. Therefore, given their more frequent interaction with medical providers and greater propensity to ask for help (Courtenay 2000), it would not be surprising for more cisgender women to report a comfortable medical experience compared with cisgender men.
There is limited information on the differences in quality of medical care of gay and lesbian individuals and even less information on the experience of bisexuals, although Blosnich and colleagues (2014) found evidence of less satisfactory medical encounters among bisexuals. Likely related to their poorer economic profile relative to gay or lesbian adults, studies document poorer access to adequate health care among bisexuals (IOM 2011). Studies also show that compared with heterosexuals and gay and bisexual men, bisexual cisgender women are the most likely to report that they did not see a medical care provider because of cost (Gorman et al. 2015). Altogether, the poorer economic profile of bisexuals, on average, in addition to the lower socioeconomic standing of cisgender women relative to men, suggests that bisexual women may face especially high challenges in accessing quality medical services compared with other gender-by-orientation groups.
Knowledge of sexual identity may also be particularly important in order for sexual minorities to receive quality care from medical providers. In general, studies show that cisgender men who are sexual minorities experience more discrimination when disclosing sexual identity than cisgender women (Swim and Hyers 2009). This could mean that men are less willing to disclose their sexual identity to a medical provider and perhaps are more likely to perceive that their medical provider is uncomfortable with their identity when they do disclose. Across sexual orientation, research documents that sexual identity disclosure rates were significantly lower among bisexuals compared with gay and lesbian adults (Durso and Meyer 2013). As past studies document lower rates of health care utilization among bisexuals (Conron et al. 2010; IOM 2011), it may be that sexual identity disclosure to medical providers is lower among bisexuals compared with gay and lesbian persons.
To date, scholarship in this area has focused mostly on cisgender adults. For transgender adults, limited research has documented whether sexual identity changes after gender transition (De Cuypere et al. 2005). Although some studies indicate that both female-to-male and male-to-female adults report changes in their sexual identity after gender transition events, including hormone therapy or reassignment surgery (Lawrence 2005; Meier et al. 2013), other work shows that these changes do not occur in context with particular transition events (Auer et al. 2014). Due to a lack of reliable representative data, it is difficult to draw conclusions on patterns of sexual orientation identification among multigendered transgender adults, or how that relates to perceptions of comfort when discussing sexual identity with medical care providers.
A lack of attention to the medical experiences of transgender adults in addition to the exclusion of how gender transition shapes quality of care has contributed to an incomplete understanding of how gender identity shapes medical experiences for transgender sexual minority adults. Given evidence of gender differences in health care experiences among cisgender sexual minority men and women, in this study we also examine the impact of gender transition among transgender men and women (male-to-female or female-to-male). Similar to cisgender men and women, we expect gender identity to condition the perceptions of provider comfort with sexual identity for transgender sexual minority adults. By examining the type of gender transition, we not only examine how perceptions of comfort differ between cisgender and transgender sexual minority men and women but also examine how they differ within the transgender identity group. In this way, our study incorporates the heterogeneity of gendered experiences within sexual identity groups into our analytic framework.
Data and Methods
Data
This article examines data from the SJSP. Collected in 2010, this study includes 4,953 respondents residing in all 50 U.S. states as well as Puerto Rico. This data set is unique because it contains a large sample of sexual (n = 4,358) and gender minorities (n = 339) residing across the United States. Although this diversity is a strength of this data set, it is also a nonprobability sample (i.e., respondents were recruited via sampling at LGBT events, respondent-driven sampling, and the Internet 3 ). As such, our sample may misrepresent the characteristics of these broader populations in some unknown way, and this selection bias may affect the findings we report—a limitation we return to in the concluding section of this article.
From the full sample of 4,953 respondents, we restricted our analytic sample to individuals aged 18 years and older that identified as a heterosexual, gay, lesbian, bisexual, or alternative adult (remaining n = 4,770). Indi-viduals who did not answer the gender identity question or identified as an alternative gender identity aside from transgender (n = 347) were dropped from the sample, as were persons who did not answer the perceived provider comfort question (n = 165). Altogether, these restrictions resulted in a final analytic sample size of 4,258 adults that included 2,142 cisgender men, 1,901 cisgender women, and 215 multigendered transgender adults.
Measures
All respondents were asked, Thinking about the last medical professional that you saw, do you feel that he/she: (a) seemed comfortable with my sexual identity, (b) seemed uncomfortable with my sexual identity, (c) seemed to ignore my sexual identity or (d) did not know my sexual identity.
From this we constructed two outcome measures. First, we examined whether respondents perceived that their medical provider had any knowledge of their sexual identity (1 = reported that their provider was comfortable, uncomfortable, or ignored their sexual identity and 0 = reported that provider did not know their sexual identity). This measure is applicable to our entire sample of N = 4,258 adults. Second, for those respondents who reported that their medical provider knew their sexual identity, we examine whether their provider seemed comfortable with their sexual identity (1 = yes, provider seemed comfortable with their sexual identity and 0 = provider seemed uncomfortable or ignored their sexual identity). This outcome is applicable to only a portion of adults in our analytic sample (N = 3,077), excluding respondents who reported that their medical provider did not know their sexual identity.
The independent variables of interest are sexual and gender identity. Respondents were asked, “Which one label comes closest to how you describe your sexual identity?” Respondents could choose between gay, lesbian, bisexual, straight/heterosexual, and a variety of other nontraditional categories (e.g., queer, same gender loving, and other). Gender identity was measured using two questions, including (1) “What is your current gender identity” with responses “male, female, transgender (male to female), transgender (female to male), multiple identities and other” and (2) “What was the sex on your original birth certificate” with responses “male, female and I don’t know.” For this article, respondents who differ in their sex at birth and current gender identity are categorized as multigendered transgender individuals based on their current gender identity (see Note 1). Although this two-step process to obtain transgender identity is not without limitations, other studies use this operationalization scheme in their analysis (e.g., see Conron, Lombardi, and Reisner 2014). Although sample size for transgender adults (n = 215) was too small to support models run separately for male-to-female and female-to-male transgender adults, we include a control for this in our models.
Similar to a previous study on transgender men (Bauer et al. 2013), we found a high number of multigendered transgender individuals who identified their sexual identity in more alternative ways. As such, an additional “alternative” sexual identity category is used in this article. This allows us to examine how perceived comfort from medical providers differs across detailed intersections of gender identity (cisgender men, cisgender women, and multigendered transgender) and sexual identity (heterosexual, gay, lesbian, bisexual, and alternative).
All models control for age at interview and race/ethnicity (categorized as non-Hispanic white, non-Hispanic black, Latino, and other). We adjust for three sets of confounding factors that may be driving differences observed across groups—including socioeconomic status, health care access and utilization, and social support.
Regarding socioeconomic status, although more cisgender women are achieving higher levels of schooling than ever, studies generally show that in the United States, cisgender men are more economically advantaged than cisgender women (APA Task Force on Socioeconomic Status 2006). The limited information that exists about the economic status of multigendered transgender individuals suggests that many are economically vulnerable and maintain low levels of educational attainment (Sanchez, Sanchez, and Danoff 2009). In terms of differences in socioeconomic status across sexual orientation, limited information have produced mixed results and weak conclusions about the economic profiles of sexual minorities (Gates 2014). Although some have suggested that sexual minorities are more highly educated and affluent than heterosexuals, other studies have shown that the pattern is dependent on specific sexual identity groups. Although gay and lesbian adults appear to be doing as well or better than heterosexuals adults, socioeconomic status among bisexuals is quite poor; on average they have lower rates of education, low reported income, and higher rates of unemployment (Badgett, Lee, and Scneebaum 2013). In our models, we adjust for the following measures of socioeconomic status: education (high school or less, some college, college graduate, and graduate/professional) and total household income. Responses for income were originally grouped into 12 intervals; each was recoded to the midpoint and then grouped into two categories: less than $30,000 and $30,000 and more.
Turning to health care access and utilization, studies show that cisgender men are less likely to use health care services compared with cisgender women (Teunissen, Rotink, and Lagro-Janssen 2016). Lower utilization rates may be driven by masculinity practices that impede men from engaging in health-promoting behavior and serve as a means of expressing gender (Courtenay 2000). Cisgender men’s unwillingness to seek medical care services results in fewer doctor visits and delays in seeking adequate treatment (Pudrovska 2010). When cisgender men do go to the doctor, studies show that they are less likely to disclose illnesses (O’Brien, Hunt, and Hart 2005). Less frequent health care utilization and decreased help-seeking behavior produces fewer opportunities for cisgender men to obtain preventative services, which can negatively affect their health status. Although research on health care utilization among transgender individuals is limited, studies report problems in access to quality health care—including lack of sensitivity from medical workers, experiences of discrimination, and low rates of insurance coverage (Sanchez et al. 2009).
Studies also demonstrate that sexual minorities avoid health prevention and treatment services more often than heterosexuals, which may in part be due to lower insurance rates and fear of discrimination (Bonvicini and Perlin 2003; IOM 2011). In addition, studies indicate that lower rates of health care utilization among bisexuals are especially pronounced (Badgett et al. 2013). Given that gender and sexual minorities are more likely to report having poor health and chronic health conditions, lower rates of health care utilization can contribute to health disparities (Ranji et al. 2015). In our models, health care utilization and access are measured using information about health insurance status (1 = insured, 0 = uninsured) and whether they have a regular medical provider (1 = yes, 0 = no).
Finally, we adjust for the potentially confounding influence of group differences in perceived social support. Research shows that social support serves as a protective buffer to both cisgender men and women by providing social ties that create feelings of intimacy, belongingness, meaning, and purpose (Umberson, Crosnoe, and Reczek 2010). Social ties can also act as protective buffers for mental distress among multigendered transgender adults (Moody et al. 2015). More generally, studies show a resilient effect on health status resulting from positive and supportive network ties composed of friends and family among sexual minority groups (IOM 2011). If individuals believe they have a reliable and supportive network, they may be more inclined to be open and honest about their sexuality and medical history to health care providers, which may create a more comfortable and effective medical care experience. Measures of social support in our models include current relationship status (unpartnered, partnered, or married) and perceived emotional support from their family, which is based on a rating of 1 to 6 (where 1 is the lowest level of perceived support and 6 is the highest).
Analytic Strategy
Data analysis was conducted using the Stata 14 software package. We begin with a descriptive presentation of how perceived comfort from medical providers about their sexual identity differs across sexual and gender identity groups. Following, we use a two-step hurdle approach and present odds ratios (ORs) from logistic regression models that first test the relationship between sexual orientation and perceived knowledge of sexual identity by medical provider in Table 2. Then, we remove respondents who reported that their medical provider did not know their sexual orientation from the analytic sample, and in Table 3, we present models predicting whether or not respondents perceived that their provider was comfortable with their sexual identity. All models are stratified by gender identity (i.e., we run separate models for cisgender men, cisgender women, and multigendered transgender adults). In each logistic regression table, Model 1 includes sexual identity and adjusts only for age and race/ethnicity. In Model 2, we add measures of socioeconomic status and health care utilization and access, and in Model 3, we add controls for social support.
Results
Sample Characteristics
Descriptive statistics for the sample are presented in Table 1. The first row shows the percentage of individuals who perceived that their medical provider was comfortable with their sexual identity. Across gender identities, rates of perceived comfort differ by sexual orientation. Bisexuals had the lowest rate of perceived comfort (33.3 percent for cisgender men and 32.4 percent for multigendered transgender adults, with the lowest comfort rate among cisgender women at 21.2 percent). At the same time, bisexuals are the most likely to report that the last medical professional they saw did not know their sexual identity (44.1 percent of multigendered transgender adults, 51.1 percent of bisexual cisgender men, and 70.5 percent of bisexual cisgender women). Among bisexual cisgender men, we also see a relatively high proportion (12.5 percent) reporting that their provider ignored their sexuality and a relatively low proportion (3.2 percent) perceiving that their medical provider was uncomfortable with their sexual identity.
Demographic and Socioeconomic Characteristics of Sample Adults, by Gender and Sexual Identity (N = 4,258).

Note. Percentages and mean values (standard deviations) are presented. HS = high school.
Across gender identities, Table 1 also shows similar proportions of heterosexual, gay, and lesbian adults perceiving comfort from their medical provider about their sexual identity (between 43 and 50 percent)—with the exception of heterosexual multigendered transgender adults, where the perceived comfort rate is much higher (63.8 percent). Despite this, one quarter of gay and one fifth of alternatively identified multigendered transgender adults reported that they perceived that their last medical provider was uncomfortable with their sexual identity.
When examining differences across gender and sexual orientation, we see that there are different levels of economic constraint, social support, and health care access—which reflect the complicated story of health disparities among sexual minorities. Among cisgender men, the average age ranges from 38.0 years (heterosexual) to 45.0 years (alternative adults), making the age span relatively small for this group. Cisgender men were highly educated, but gay and alternative cisgender men reported higher levels of completed schooling, and fewer reported low income than heterosexual cisgender men. In addition, heterosexual (69.6 percent) cisgender men had lower rates of having a regular medical provider compared with gay (84.5 percent), bisexual (82.5 percent), and alternative (83.7 percent) cisgender men. Heterosexual cisgender men also reported the highest, whereas bisexual cisgender men reported the lowest, rate of marriage and perceived family support.
Cisgender women in the analytic sample range in age from 36 years for heterosexuals to 44 years for lesbians. Education and income levels are highest among lesbian and alternative cisgender women. Income levels are lowest for bisexual cisgender women, who also report the lowest level of perceived family support. Heterosexual cisgender women report much higher levels of perceived family support than sexual minority cisgender women, and they also report the highest rates of having insurance as well as a regular medical provider.
Multigendered transgender adults show a mixed pattern of risk and protective health characteristics. In terms of gender transition, Table 1 shows that 32.6 percent of heterosexual transgender adults are female-to-male. Among transgender sexual minorities, we see a range from 24.4 percent (bisexual transgender adults) to 51.6 percent (lesbian transgender adults) as female-to male. Across sexual orientation groups, multigendered transgender adults report relatively low levels of income and family support relative to cisgender men and women. However, there are proportionately higher percentages of married heterosexual (31.1 percent) multigendered transgender individuals compared with gay (17.7 percent), lesbian (16.3 percent), and alternative (15.4 percent) multigendered transgender individuals. Education levels are also low for gay, lesbian, and alternative multigendered transgender adults, but completed schooling is slightly higher among heterosexual transgender adults when compared with heterosexual cisgender men and women. Although multigendered transgender adults who identify as lesbian report lower rates of health insurance and regular doctor coverage than lesbian cisgender women, multigendered transgender adults who identify as bisexual report higher rates than either bisexual cisgender men or women. Among heterosexuals, multigendered transgender persons report rates of health insurance and regular doctor coverage that are more similar to cisgender women than to men.
Logistic Regression Models
Table 2 shows ORs from logistic regression models predicting perceived knowledge of respondent sexual identity by their medical provider, stratified by gender identity. Looking first to cisgender men, we see no significant association between sexual identity and perceived provider knowledge of sexual identity. Among the control measures, we see that those with a regular doctor have more than twice the odds (OR = 2.78 in Model 3) of perceiving that their medical provider knows their sexual identity than those without a regular provider. We also found that, relative to those with no partner, being partnered (OR = 1.26) or married (OR = 2.21) is associated with significantly higher odds of reporting perceived provider knowledge of their sexual identity. Although Model 2 found a significant and positive association for household income (OR = 1.31), this was reduced to nonsignificance in Model 3 after adjustment for relationship status and perceived family support.
Odds Ratios from Logistic Regression Models Predicting Perceived Knowledge of Sexual Identity by Medical Provider (N = 4,258).
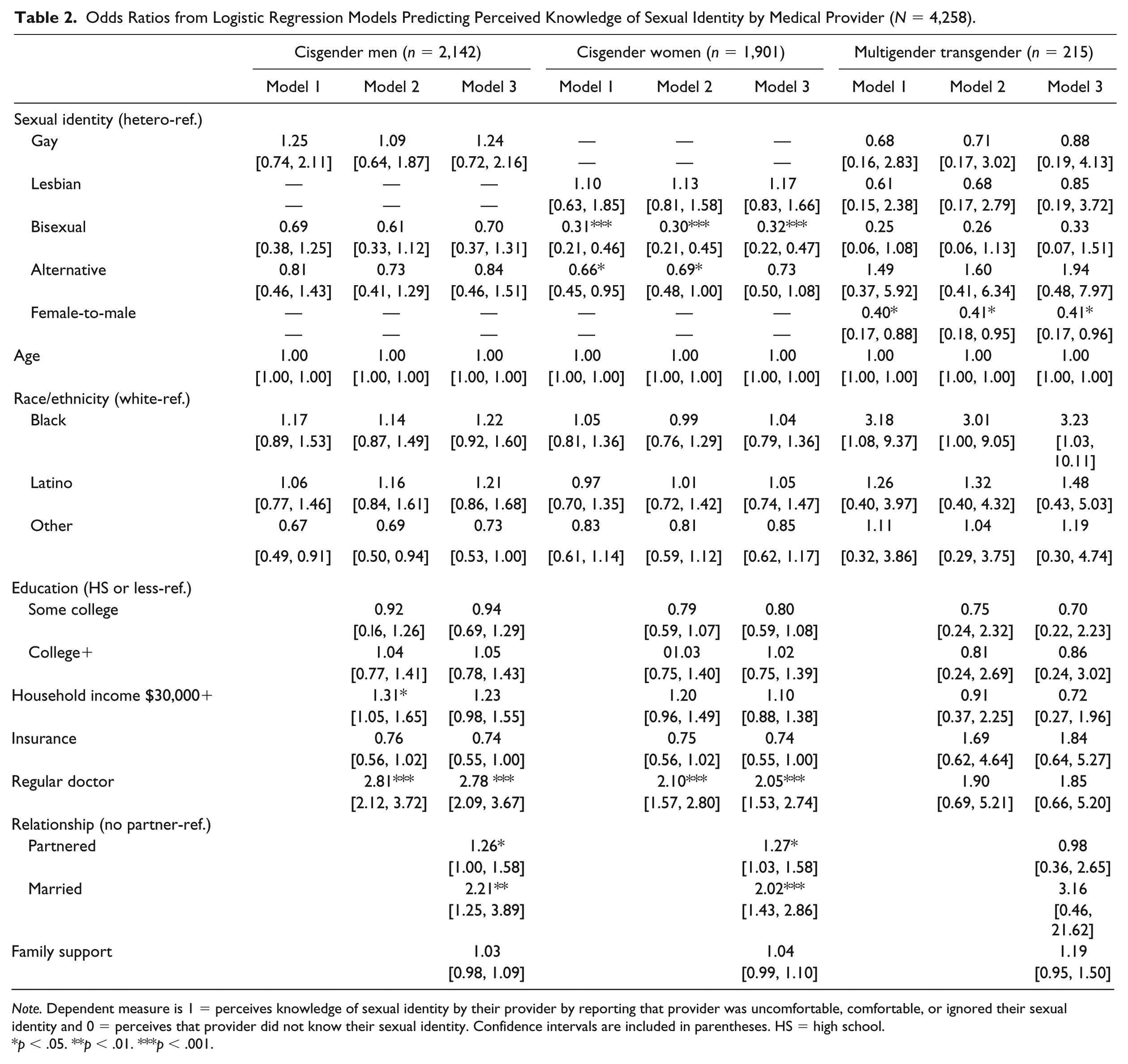
Note. Dependent measure is 1 = perceives knowledge of sexual identity by their provider by reporting that provider was uncomfortable, comfortable, or ignored their sexual identity and 0 = perceives that provider did not know their sexual identity. Confidence intervals are included in parentheses. HS = high school.
p < .05. **p < .01. ***p < .001.
Among cisgender women, we found a significant association between sexual identity and perceived medical provider knowledge of their sexual identity. Compared with heterosexual cisgender women, the odds of perceiving provider knowledge was significantly lower among bisexuals—and across all three models, ORs for bisexual women shift very little (OR = 0.32 in Model 3). Models 1 and 2 also show that alternative cisgender women also have significantly lower odds of perceiving that their provider knew their sexual identity. However, controlling for relationship status reduces the contrast among alternative cisgender women relative to heterosexual cisgender women to nonsignificance. Similar to cisgender men, Model 1 shows no significant differences in demographic characteristics, while adjusting for socioeconomic status and health care access and utilization in Model 2 shows that having a regular doctor is associated with significantly higher odds (OR = 2.10) of reporting perceived provider knowledge of sexual identity. In Model 3, similar to cisgender men, relationship status is significant in that respondents with a partner (OR = 1.27), and especially those who are married (OR = 2.02), are more likely to perceive that their medical provider knew their sexual identity.
Finally, Table 2 shows the ORs for predicting perceived knowledge of sexual identity by medical provider among multigendered transgender adults. Most measures are not significant, with the exception of gender transition. Across all three models, female-to-male transgender adults have significantly lower odds (OR = 0.41 in Model 3) of perceiving that their medical provider knew their sexual identity relative to male-to-female transgender adults.
Next, we removed respondents who reported that their medical provider did not know their sexual identity from the analytic sample, and in Table 3 we present models predicting whether or not respondents perceived that their provider was comfortable with their sexual identity. Among cisgender men, again we see no significant differences across sexual identity in any model. Among the control measures, having a regular doctor is strongly associated with perceiving comfort from their medical provider with their sexual identity (OR = 2.48 in Model 3). In addition, increased levels of perceived family support are associated with higher odds (OR = 1.21) of reporting perceived provider comfort with sexual identity.
Odds Ratios from Logistic Regression Models Predicting Perceived Medical Provider Comfort with Sexual Identity, among Respondents Reporting Provider Knew Their Sexual Identity (N = 3,077).

Note. Models limited to respondents who perceived that their medical provider knew their sexual identity. Dependent measure is 1 = perceives that provider is comfortable with their sexual identity and 0 = perceives provider is uncomfortable or ignored their sexual identity. Confidence intervals in parentheses. HS = high school.
p < .05. **p < .01. ***p < .001.
Among cisgender women, bisexuals are about half as likely as heterosexuals to perceive that their provider was comfortable with their sexual identity. Once we adjust for family support in Model 3, however, this association becomes nonsignificant. Among control measures, being black (OR = 1.56 in Model 3), having a regular doctor (OR = 2.48 in Model 3), and having perceived family support (OR = 1.21 in Model 3) are associated with significantly higher odds of reporting perceived provider comfort with their sexual identity.
Finally, among multigendered transgender adults, we see that gay adults have significantly lower odds of reporting perceived provider comfort in Models 1 and 2 (OR = 0.28), relative to heterosexual transgender adults. However, after we adjust for relationship status and family support in Model 3, this contrast becomes nonsignificant. Unlike Table 2, we see no significant differences between female-to-male and male-to-female transgender adults in perceived provider comfort, across all models. Similar to cisgender men and women, we see that having a regular doctor is associated with significantly higher odds of reporting perceived provider comfort with sexual identity (OR = 2.69). Model 3 also shows that being partnered (OR = 2.33) along with increasing perceived levels of family support (OR = 1.28) is associated with higher odds of reporting perceived provider comfort with sexual identity among this group.
Discussion
There are three main findings to highlight from our analysis. First, the most consistent finding is that, compared with heterosexual cisgender women, bisexual cisgender women are less likely to perceive that their provider knew their sexual identity—and if they did perceive knowledge, they were less likely to perceive that their provider was comfortable with their sexual identity. These findings are perhaps unsurprising given the intersectional position that bisexual cisgender women hold. In terms of knowledge, bisexual cisgender women may have failed to disclose, or the provider failed to ask, about their sexual orientation. Work has shown that bisexuals are less likely to be “out” than gay/lesbian adults due to fear of harassment as well as a tendency to “pass” as heterosexuals among medical providers to avoid negative or uncomfortable interactions (Lingel 2009). Given that sexual minority patients have health risks that require honest and quality communication for an accurate diagnosis (Dahan et al. 2008), and many sexual minority patients believe their health care would be of higher quality if they could safely disclose their sexual identities (Makadon 2006), our findings suggests that bisexual cisgender women may be more at risk of experiencing medical interactions that are less informative and more uncomfortable.
In addition, previous work has noted the lower economic profile of bisexuals among cisgender women relative to cisgender men, as well as documenting that bisexuals are more economically vulnerable relative to heterosexuals and other sexual minority groups (IOM 2011). Other work documents low rates of health care utilization along with higher rates of poor physical health and mental distress (Gorman et al. 2015; IOM 2011) among bisexuals. Among cisgender women in our sample, heterosexual cisgender women have only slightly higher rates of reporting perceived provider comfort than lesbian cisgender women, but have more than double the comfort rate compared with bisexual cisgender women. Given the lower rates of health care utilization and economic profiles of bisexuals in addition to lower rates of sexual identity disclosure (Durso and Meyer 2013), it is not too surprising to see lower rates of perceived provider comfort among cisgender bisexual women relative to heterosexual and lesbian cisgender women.
Second, our results also showed that female-to-male transgender adults have significantly lower odds of perceiving that their medical provider knows their sexual identity than male-to-female transgender adults. However, among those who indicated that their provider had knowledge, gender transition was not significantly associated with perceived comfort with their sexual identity. We also found that gay transgender adults have significantly lower odds of perceiving provider comfort with their sexual identity relative to heterosexual transgender adults. Other intersectional work has found that gay transgender adults experience an elevated risk of violence and harassment in social interactions due to the history of gay men being either stereotyped as sexual deviants or overly feminized (Vidal-Ortiz 2002). Scholars point to the cultural expectations gay transgender adults face in navigating not only how men should act in social interactions but in how sexual minority men should act due to the interplay of gay transgender adults living as both gender and sexual minorities (Schilt 2010). This interplay between gender and sexuality that transgender adults experience after transition, which Schilt and Windsor (2014) referred to as “sexual habitus,” reflects the dynamic manner in which “gendered sexuality” shapes experiences and behaviors.
One limitation of our study is that we do not know the context in which the referenced medical encounter occurred (e.g., with a regular doctor vs. a physical exam). Even so, our finding that female-to-male transgender adults have lower odds of perceiving that their medical provider knew their sexual identity is in-line with scholarship by Scheim and Bauer (2015), documenting that female-to-male adults are more likely to have socially transitioned without medical intervention, and that they are less likely to be perceived as transgender by others. Other work shows that female-to-male transgender people report higher rates of postponing medical care when sick or injured because of fear of discrimination by medical providers (Grant et al. 2010). Altogether, this suggests that female-to-male transgender adults may be less likely to disclose details of their identity, gender, or sexual, to a medical provider than male-to-female transgender adults. Ultimately, more research is needed to examine our finding of difference in perceived knowledge about sexual identity, but not perceived comfort, across gender transition groups.
Finally, our analyses demonstrated the importance of medical and social relationships for perceiving both knowledge and comfort with sexual identity from medical care providers. Similar to previous studies (Spooner et al. 2016), we found that across all gender identity groups having a regular medical provider was significantly associated with a more positive medical experience. As trust and support in the provider-patient relationship are vital for comfortable health care experiences, it makes sense that having a regular medical provider is strongly associated with respondents perceiving provider comfort with their sexual identity. That said, while having a regular doctor was significantly associated with perceiving provider knowledge of sexual identity for cisgender men and women, the relationship was not significant for multigendered transgender adults. Additional study is needed to explore the meaning behind this finding.
Our results also demonstrated the salubrious role for personal relationships and perceived family support, which is well supported by prior work demonstrating the positive effects of familial support among sexual minorities for health status and well-being (Watson, Barnett, and Russell 2016). Our findings highlight the important role of partners (marital and nonmarital) for cisgender men and women in perceiving that their medical provider knows their sexual identity and the positive role of family support for perceiving that medical providers are comfortable with sexual identity among cisgender and multigendered transgender adults.
Conclusion
Effective and comfortable provider-patient communication is important because it is highly correlated with positive health outcomes and engagement in health-promoting behavior (Spooner et al. 2016). Individuals who feel comfortable with their medical provider may feel empowered because they are able to ask questions, communicate assertively, and express concerns and feelings about their health (Jenerette and Mayer 2016). In order to expand the limited research on medical experiences of transgender adults and sexual minorities, we applied an intersectional lens to investigate whether gender identity conditioned the relationship between sexual orientation and perceived provider knowledge and comfort with their sexual identity.
We found evidence that perceived provider comfort was shaped by the sexual orientation of the patient as well as their gender identity. Scholars have pointed to the importance in examining intersectional social positions to obtain a more complete understanding of experiences across social groups (Bauer 2014; McCall 2005). In our study, we found that sexual orientation was not the sole stratifier of adults perceiving that a medical provider is comfortable (or not) with their sexual orientation. This indicates that having a shared sexual identity does not necessarily mean that patients will report similar medical experiences—and our results suggest that studies which neglect the manner in which gender and sexuality intersect may overlook important differences across gender by orientation groups.
We also evaluated whether observed differences in reported knowledge or perceived comfort across groups were confounded by socioeconomic status and other health-relevant controls. Although we found heterogeneity across gender identity groups in perceived provider comfort, we also found evidence that having a regular doctor and family support was an important predictor of perceiving that their medical provider was comfortable with their sexual identity. This was true across all gender identity groups, indicating that there are certain factors that can contribute to positive medical encounters for sexual minorities regardless of gender identity. Thus, despite the differences across intersectional positions in medical experiences, there may be certain health-promoting resources that are beneficial for all groups.
Although our study provides novel information about medical interactions among under-examined populations, a key limitation is that we examine data from a nonprobability sample of adults. As the sample was collected using purposive selective methods, our findings about perceived provider comfort may misrepresent the characteristics of gender and sexual minorities to some unknown extent. Compared with demographic characteristics of the LGBT population drawn from probabilistic surveys, our sample is similar in patterns of average age, education, and income (Gates 2014), although research does suggest that region and racial identity contribute to economic variability (Kastanis 2016). Despite the nonprobability nature of the data used, our study provides needed information about overlooked populations across all 50 states, and other scholars have used this data set to examine differences across a range of outcomes (Turner, Pastrana, and Battle 2015). Future work should collect similar information using probability-based sampling to draw more generalizable conclusions.
In addition, the relatively small size of the transgender population in the SJSP prohibited stratification of multivariate regression models by gender transition category. Although we were able to include a gender transition control variable in our models (contrasting female-to-male with male-to-female adults), additional work with a larger sample is needed for a more detailed assessment of how gender transition category relates to sexual identity and interactions with medical care providers. Finally, a key limitation of our study relates to the outcomes variable. The SJSP did not collect information from medical providers and instead relied on respondents to self-report their perceptions of how providers behaved during their last medical care interaction. As a result, the respondent’s own biases may influence this outcome to an unknown extent. For example, Table 1 shows that heterosexual cisgender men report lower rates of perceiving that their medical provider was comfortable with their sexual identity than gay cisgender men, heterosexual cisgender women, and heterosexual multigendered transgender adults. It may be that our models are capturing discomfort among these men in answering this question, rather than actual discomfort from medical providers with the sexuality of heterosexual cisgender men. In addition, we do not have any information about the specifics of the medical care interaction (e.g., with a first time or ongoing provider), which prohibits our ability to investigate this further and suggests another avenue for future work in this area.
Given that the average medical visit lasts between 10 and 16 minutes (Nouri and Rudd 2015), effective communication is highly significant in ensuring that appropriate diagnosis, treatment, and management of illness occur among vulnerable communities. This can be especially important to members of marginalized communities with high health risk profiles that require more frequent interaction with medical professionals. Unfortunately, the limited nature of existing research on gender and sexual minorities has made it difficult to assess the extent of disparities in quality of care. In addition to underlining the importance of the quality of provider-patient interactions, our study also highlights the importance of considering how the specific intersectional position that one holds relates to medical care experiences among adults.
Within the medical context, effective training of medical professionals can improve experiences with members of marginalized communities. To start, there is limited training and education on sexuality and gender identity for health professionals and medical students. Textbooks, medical school courses, and training seminars that discuss the varied cultural expressions of sexuality can contribute to more effective communication, and more comfortable encounters overall, between patients and medical providers (Malebranche et al. 2004). Within the medical encounter, focusing on the use of heteronormative language that assumes different sex partnership from medical professionals can avoid causing distress and reduce apprehension for gender and sexual minority patients, especially when choosing to disclose sexual orientation. Research shows that this can be accomplished by focusing on wording of questions about sexual orientation, sexual history, and partnership rather than assuming heterosexuality and different sex coupling. When inquiring about sexual history, medical professionals should do so in ways that can be answered by all patients regardless of partnering status and follow questions with nonjudgmental discussions (Politi et al. 2009).
In conclusion, additional research centered on the medical experiences of gender and sexual minority patients can provide more insight into the gap in quality of medical care. Ultimately, future studies should continue examining how medical experiences differ across groups, especially among those with poorer health status and health behavior risks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.