
Abstract


KEY POINTS
Ultrasound elastography demonstrates modest incremental diagnostic value when added to conventional grayscale ultrasound risk stratification.
Integration of elastography with American College of Radiology Thyroid Imaging Reporting and Data System may improve specificity and reduce unnecessary biopsy in selected nodules.
Variability in technique, thresholds, and operator dependence of elastography limits routine incorporation into standardized algorithms.
SUMMARY
Background
Ultrasound risk-stratification systems such as the American College of Radiology (ACR) Thyroid Imaging Reporting and Data System (TI-RADS) have attempted to standardize the evaluation of thyroid nodules and reduced unnecessary biopsies. 1 However, overlap in sonographic features between benign and malignant nodules persists. Ultrasound elastography, which assesses tissue stiffness, has been proposed as an adjunctive tool to improve diagnostic accuracy, noting that lower tissue stiffness (softer nodules) suggests benignity. Angelopoulos et al. evaluated the performance of elastography when integrated with conventional ultrasound risk-stratification systems. 2
Methods
This prospective study evaluated thyroid nodules referred for FNA according to the ACR TI-RADS recommendations. All nodules in the study underwent cytological analysis using the Bethesda system, but not all had definitive surgical pathology. Strain elastography measurements were analyzed alongside grayscale ultrasound features. Diagnostic performance metrics, including sensitivity, specificity, and area under the receiver operating characteristic curve, were calculated for conventional ultrasound alone and in combination with elastography.
Results
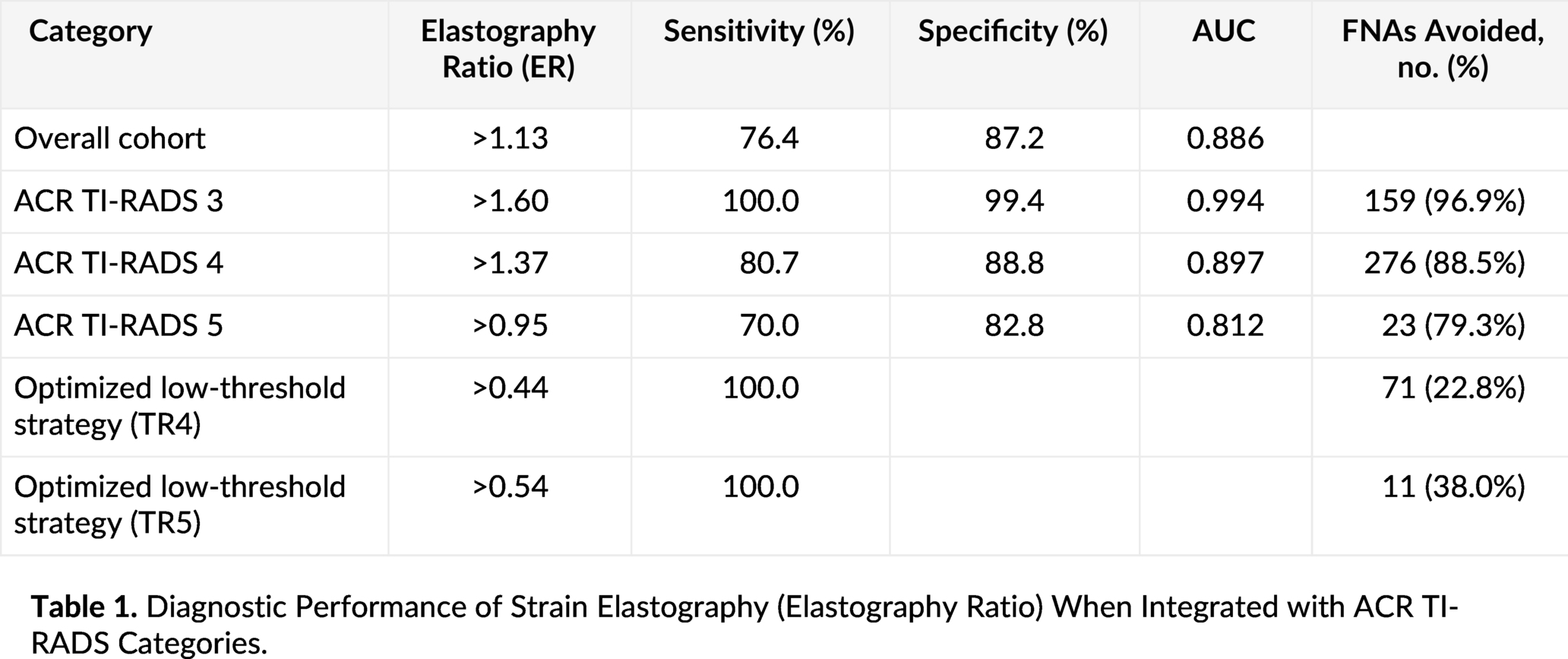
There were 1890 nodules with Bethesda III, IV, or V cytology included in the study. Table 1 shows a summary of the findings. Elastography demonstrated increased stiffness in malignant nodules compared with benign nodules. When combined with TI-RADS classification, specificity improved while maintaining acceptable sensitivity. Applying elastography ratio thresholds for TI-RADS categories 3, 4, and 5 nodules that were referred for FNA reduced the number of recommended biopsies by 48.1% without missing any malignant cases. The greatest benefit was observed in intermediate-risk nodules, where elastography helped refine biopsy decisions. However, overlap in stiffness values remained, and performance varied depending on technique and cutoff thresholds.
Diagnostic Performance of Strain Elastography (Elastography Ratio) When Integrated with ACR TI-RADS Categories.
Conclusions
Ultrasound elastography provides incremental diagnostic value when combined with TI-RADS, particularly in intermediate-risk nodules, with the elastography ratio threshold being particularly discriminatory in TI-RADS 3 category nodules. ardization and further validation are needed before widespread incorporation into routine risk-stratification algorithms.
COMMENTARY
Without a doubt, one of the most frustrating aspects of clinical thyroidology is the frequent inability to give a patient a definitive diagnosis and the anxiety patients develop over their nodules, especially when they are recommended for FNA. Risk stratification of thyroid nodules has evolved substantially with the adoption of structured ultrasound systems such as the ATA criteria and ACR TI-RADS.1,3 These frameworks prioritize grayscale sonographic features and have successfully reduced unnecessary biopsy without compromising cancer detection. Nevertheless, indeterminate nodules remain common, and we should continue to seek adjunctive tools to refine management. Elastography represents one such tool, measuring tissue stiffness as a surrogate for malignancy. 4
The study by Angelopoulos et al. suggests that elastography may offer modest incremental benefit when integrated with existing ultrasonographic risk-stratification systems. Notably, the improvement appears greatest in nodules that fall into intermediate-risk categories. This is clinically meaningful, as these nodules often drive uncertainty in FNA biopsy decisions. In such cases, additional stiffness information may help avoid FNA biopsy in nodules that would otherwise meet size thresholds.
However, several limitations understandably temper enthusiasm for routine incorporation. Elastography performance varies across platforms and techniques, including strain versus shear-wave elastography. 5 Reported stiffness thresholds differ among studies, and reproducibility remains operator-dependent. Furthermore, malignant nodules—particularly follicular-pattern cancers—may not demonstrate markedly increased stiffness, limiting sensitivity. 6
From a practical standpoint, integration with ACR TI-RADS should be selective rather than universal. Elastography may be most useful when grayscale features and clinical context are discordant or when considering deferral of biopsy in borderline cases. Importantly, any adjunctive technique should not override well-established sonographic risk features. The broader question is whether elastography meaningfully alters management. Although specificity improvements are appealing, they must translate into fewer biopsies without missed malignancies. Prospective studies incorporating management outcomes will be particularly valuable. Until then, elastography should be considered complementary rather than essential.
Elastography demonstrates the greatest incremental value in low- and intermediate-risk nodules, particularly ACR TI-RADS 3, where it functions as a highly effective rule-out test and substantially reduces unnecessary FNA procedures without compromising sensitivity. Data derived from Angelopoulos et al.