
Abstract

KEY POINTS
Although radioactive iodine–refractory (RAIR) differentiated thyroid cancer is associated with worse oncologic outcomes, in the 2025 ATA management guidelines, RAIR DTC is not always an immediate indication for tyrosine kinase inhibitor (TKI) therapy.
In carefully selected patients, localized therapies may postpone the need for systemic TKI therapy, improve quality of life, result in long durations of disease control, and optimize long-term management.
SUMMARY
Background
The rationale for prioritizing localized therapy before—or sometimes instead of—systemic therapy in metastatic radioactive iodine–refractory differentiated thyroid cancer (RAIR DTC) has become increasingly clear in recent years and is now strongly reflected in both the 2025 American Thyroid Association (ATA) and the current National Comprehensive Cancer Network (NCCN) guidelines.1,2 Rather than relying on a purely systemic approach, contemporary management increasingly recognizes that many patients may derive prolonged benefit from focal therapies capable of delaying tyrosine kinase inhibitor (TKI) initiation while preserving quality of life. This concept is supported by five converging principles: the variable biology of RAIR DTC that does not uniformly result in rapid progression, the noncurative nature and substantial toxicity associated with currently available TKIs, the potential of local therapies to provide durable disease control, the possibility that local treatment may optimize or prolong TKI efficacy, and the importance of maintaining long-term quality of life in patients who often live many years with metastatic disease.1–5
One of the central arguments favoring local therapy first is the remarkably heterogeneous natural history of metastatic DTC. Both the ATA and NCCN documents emphasize that some patients may remain asymptomatic, with minimally progressive disease, for years without clinically meaningful disease-related morbidity. Because disease kinetics can vary dramatically—from rapidly progressive to extremely indolent—immediate systemic therapy is not universally appropriate. The NCCN specifically notes that patients with indolent and asymptomatic disease may not be ideal candidates for kinase inhibitor therapy. 2 In this context, active surveillance with serial imaging at intervals of 3-12 months may be entirely reasonable for selected patients with stable or slowly progressive disease. 1
Importantly, none of the currently approved TKIs for RAIR DTC are curative.1–3 Although agents such as lenvatinib and sorafenib have significantly improved progression-free survival, treatment-related toxicity remains a major limitation in real-world practice. More than 90% of patients treated with TKIs experience at least one adverse event during therapy. 4 Hypertension, fatigue, diarrhea, mucositis, weight loss, anorexia, proteinuria, hand–foot syndrome, rash, and musculoskeletal symptoms are among the most frequently reported toxicities.1,4,5 In the SELECT trial, 6 dose interruptions and dose reduction were required in the majority of patients receiving lenvatinib, and treatment-related deaths were also observed. Similar toxicity profiles have been consistently reported with sorafenib and other multikinase inhibitors. The recent ASCO guidelines further reinforced that adverse events frequently lead to treatment interruption, dose reduction, or permanent discontinuation. 7 Even more importantly, many patients who are asymptomatic from their cancer may ultimately experience worse quality of life from treatment than from the disease itself.
What Do the 2025 ATA Guidelines Say?
This is precisely where localized therapies gain relevance. The 2025 ATA Guidelines markedly expanded the discussion surrounding focal treatment approaches for metastatic DTC, particularly in the setting of oligometastatic or symptomatic RAIR disease.
Recommendations 76-79 formally incorporated surgery, stereotactic body radiation therapy (SBRT), thermoablation techniques such as radiofrequency ablation (RFA), cryoablation, and microwave ablation, as well as cementoplasty and other directed interventions into the therapeutic framework for metastatic DTC. This represents a substantial evolution compared with the 2015 ATA guidelines and reflects the growing body of evidence supporting the role of local therapies in carefully selected patients.
For patients with oligometastatic RAIR DTC, the ATA now suggests that focal ablative treatment may be considered, ideally within a multidisciplinary setting. Lung metastases remain the most common distant metastatic site, followed by bone metastases. Available local approaches include surgery, radiation-based strategies such as SBRT, and percutaneous ablative techniques. Retrospective series on pulmonary metastasectomy demonstrated impressive long-term disease-specific survival, while thermal ablation data from the TUTHYREF network also showed encouraging overall survival outcomes in patients with lung metastases treated with RFA, cryoablation, or microwave ablation. 8 Additionally, evidence from the SABR-COMET trial 9 suggested that aggressive local therapy may improve survival outcomes across oligometastatic solid tumors.
Another increasingly important concept is the integration of local therapy with systemic treatment during oligoprogression. Directed local treatment may allow continuation of an otherwise effective TKI beyond initial focal progression, potentially extending overall clinical benefit.1,10,11 This strategy has become particularly attractive in patients with otherwise controlled systemic disease who develop isolated progressive lesions during TKI therapy. Emerging evidence suggests that local treatment combined with TKIs may enhance disease control and prolong the therapeutic window before switching to alternative systemic therapies.10–12
The ATA recommendations also strongly support local therapy for symptomatic metastatic disease. Directed interventions can rapidly palliate symptoms, prevent anatomical complications, and improve functional outcomes. SBRT has demonstrated durable local control for both lung and bone metastases, while thermal ablation approaches offer important alternatives in patients previously treated with radiation or considered poor surgical candidates. Bone-directed procedures such as vertebroplasty or cementoplasty may significantly reduce pain and improve mechanical stability, especially in osteolytic lesions associated with high skeletal morbidity.
Management of bone metastases was also expanded in the updated guidelines. The ATA now recommends bone-modifying agents such as zoledronic acid or denosumab in patients with symptomatic and/or multiple bone metastases to reduce skeletal-related events. However, these therapies also require careful consideration of long-term toxicity, particularly osteonecrosis of the jaw and hypocalcemia.
Similarly, in patients with brain metastases, the guidelines prioritize resection and/or SBRT as the preferred initial approach. Stereotactic techniques are generally favored over whole-brain radiation because of lower neurocognitive toxicity while maintaining excellent local control for limited intracranial disease.
COMMENTARY
Overall, the growing emphasis on localized therapy reflects a broader shift in the management philosophy of metastatic RAIR DTC. Rather than viewing systemic therapy as the inevitable next step after radioiodine refractoriness, clinicians are increasingly recognizing the value of individualized sequencing strategies that balance disease control with long-term tolerability and quality of life (Figure). Many patients with RAIR DTC live for years with relatively indolent disease, and the possibility of delaying systemic treatment—while still maintaining excellent oncologic outcomes—has become an increasingly important goal in contemporary thyroid oncology practice.
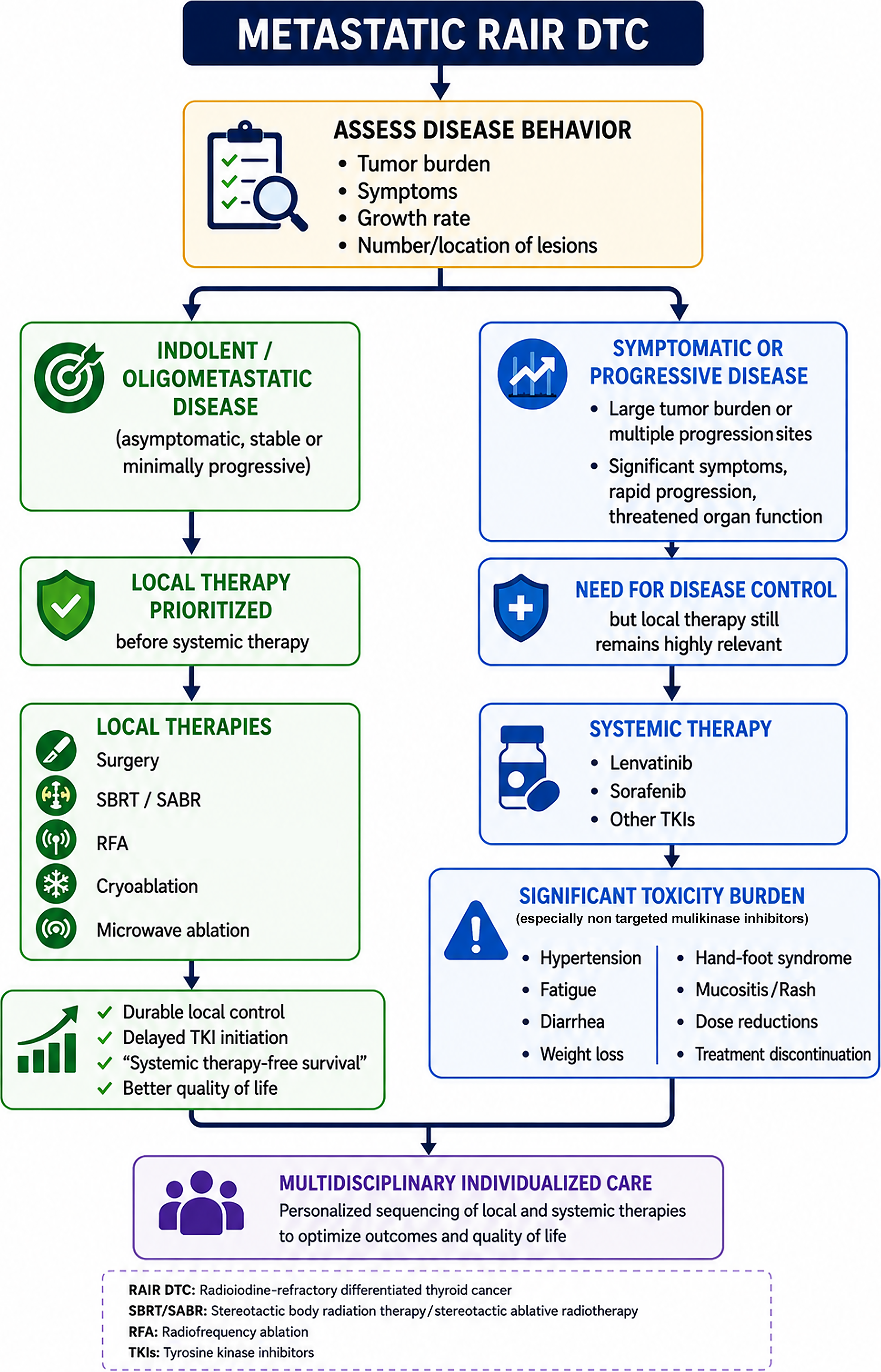
Proposed framework for treatment sequencing in metastatic RAIR DTC. Artificial intelligence–assisted software (ChatGPT) was used for the graphical rendering of this original author-designed figure; all scientific content and final editing were performed by the author.
In the end, the rationale is actually quite simple: many RAIR DTCs do not behave in a rapidly progressing way, TKIs are effective, but far from benign in their side effects, and well-selected local therapies can often control disease for prolonged periods (“systemic therapy–free survival”) while allowing patients to maintain a better quality of life. The expanding role of surgery, SBRT, and thermoablative techniques is therefore not about replacing systemic therapy altogether, but about using the right treatment at the right moment—and sometimes buying patients years before they truly need long-term systemic treatment.