
Abstract
This study uses the National Longitudinal Study of Adolescent to Adult Health to examine racially patterned mechanisms linking parental income and early adult depression, focusing on the mediating roles of family support and college enrollment. Findings suggest two noteworthy Black-White differences. First, parental income is positively correlated with depression for Black adolescents through family support. This is because high parental income tends to decrease family support for Black adolescents, a pattern not replicated for White adolescents. Second, college enrollment mediates the relationship between parental income and adult depression for Whites but not Blacks. This is because Black respondents in high-income families tend to have lower chances of college enrollment than their White counterparts, and this also leads to unequal mental health benefits for highly educated Blacks. These results, framed within a life-course perspective, provide insights about how the pathways from class to mental health are shaped by race.
Keywords
Introduction
Individuals who are exposed to more social and economic stressors tend to have worse mental health (Kessler 1997; Pearlin 1989; Turner and Lloyd 1999). However, although Blacks experience more stress than Whites in the United States (Williams and Collins 1995), racial differences in mental health remains unclear, and the evidence of racial differences often depends on the measures of mental health. For example, while some studies have found that Blacks exhibit lower rates of major depressive disorder or anxiety disorder (Kessler, Mickelson, and Williams 1999; Riolo et al. 2005), others have argued that Blacks consistently report higher psychological distress relative to Whites (Centers for Disease and Control and Prevention 2010; Pratt 2009; Roxburgh 2009).
These inconsistent findings may come from the fact that racialized social systems are not carefully considered in the analysis (Bonilla-Silva 1997; Brown 2003) and mental health status and structural variables, including class and race, are interrelated in complex ways across the life course (Aneshensel 2009; Hayward et al. 2000; Vega and Rumbaut 1991). Although some scholars argue that racial socioeconomic inequality accounts for racial mental health (Yao and Robert 2008), the majority of studies suggest that socioeconomic disadvantages do not fully explain racial mental health disparities (Hayward et al. 2000; Williams and Sternthal 2010). Given that race is socially constructed and racial minorities are unequally exposed to discrimination, racial disparities in mental health can be brought about by racial stratification or racism in society (Brown 2003; Jackson et al. 1996). Moreover, racial differences in health are differently shaped across the life course, interacting with other factors such as age, sex, and socioeconomic conditions (Brown, O’Rand, and Adkins 2012; Hargrove and Brown 2015; Richardson and Brown 2016). That is, the roles of social circumstances surrounding adolescents, such as family and educational system, may differently influence adult health outcomes by race.
To shed additional light on the issue of racial disparities in mental health, this study uses data from the National Longitudinal Study of Adolescent to Adult Health (Add-Health), to investigate different pathways of parental income to adulthood mental health across Blacks and Whites. This analysis focuses on family support in adolescence and college enrollment in young adulthood as potential mechanisms. These two variables differ in important ways between Blacks and Whites in the United States and have important influences on mental health, and therefore they are likely central to understanding race disparities in mental health.
This analysis is informed by and contributes to a life-course model of health disparities. A life-course perspective examines how early environment shapes adult health through biological, behavioral, and psychosocial processes, focusing on the importance of temporality (Ben-Shlomo and Kuh 2002; Hayward and Gorman 2004; Luo and Waite 2005). Adolescence is a physically and psychologically key development period, which often places individuals on trajectories toward unequal positions in adult health and socioeconomic hierarchies (Adler and Stewart 2010; Crosnoe and Johnson 2011). Experiences of adolescence are also racialized in many important ways, which may influence later mental health (Williams, Costa, and Leavell 2010). Nevertheless, surprisingly little is known about whether and how the pathways between childhood disadvantage and adult health differ across racial groups, so more research is required to understand the racially different pathways from the life-course perspective (Pavalko and Caputo 2013). This study responds to such a need by investigating how the mechanisms of parental income and adult depression may act differently by race.
Background
Black-White Differences in Mental Health
A recent review article regarding Black-White differences in mental health found a “double paradox” (Barnes and Bates 2017). The first paradox is that the prevalence of major depressive disorder is lower among Blacks despite their having higher levels of stress in the United States (Kessler et al. 1999; Riolo et al. 2005). The second is that, although major depression and psychological distress are positively associated, Blacks consistently report higher psychological distress relative to Whites (Centers for Disease and Control and Prevention 2010; Pratt 2009; Roxburgh 2009). Although selection bias (e.g., a disproportionate population of Blacks are incarcerated) and measurement errors (e.g., existing variables do not adequately measure the mental illness of Blacks) may contribute to these paradoxical findings, previous research found that these factors are shown to be insufficient explanations (Breslau et al. 2008; Mezuk et al. 2013).
To better understand racial disparities in mental health, it is important to focus more on how social structure affects an individual’s mental health (Brown 2003). Blacks are exposed to higher race-related stress relative to Whites, such as racial residential segregation, low employment, and high rates of incarceration (Pager and Shepherd 2008; Williams and Collins 1995). These stressful circumstances resulting from racial stratification or racism may produce emotional distress and psychiatric disorders for Blacks (Williams et al. 2010). On the other hand, Blacks may have different coping mechanisms such as better social support, religious participation, or poor health behaviors mitigating the adverse effects of stress (Boardman and Alexander 2011; Jackson, Knight, and Rafferty 2010). Together these findings suggest that investigating the interaction between race and other social structural factors helps us to comprehend the seeming paradoxical relationship around Black-White differences in mental health.
Inequalities in Depression with a Life-course Perspective
According to the life-course perspective, early-life environment influences children’s later cognitive, socioeconomic, and health outcomes (Ben-Shlomo and Kuh 2002; Luo and Waite 2005). Early environment has many factors that influence “initial set points of trajectories of mental health over the life course” (Avison 2010:361), including family socioeconomic status (SES), social relationships, and stressful life events (Adkins et al. 2009; Thoits 2011). For example, family economic conditions shape the life chances and instability of family, and they consequently play a key role in determining adolescents’ health in the long term through experiences in family, school, and neighborhood (Adler and Stewart 2010; Luo and Waite 2005). Within the life-course literature, many scholars emphasize the indirect effects through which childhood and adolescent environments set individuals into the social trajectories that affect later health (this is often referred to as a “pathways” model) (Ben-Shlomo and Kuh 2002; Hertzman 1999).
Multiple mechanisms have been provided to explain the trajectories that link early circumstances and later mental health across the life course. For example, Pearlin and his colleagues have developed their stress process model, which explains how social structure or systems of stratification, including SES, race/ethnicity, and gender, affect individuals’ mental health (Aneshensel 2009; Pearlin 1989; Turner and Lloyd 1999). They have identified social support, mastery, coping resources, and self-esteem as mediators and have demonstrated that the distribution of mental health is affected by social stress including racial discrimination. In comparison, the environmental affordances model better highlights the intersection of status-based stressors, health behaviors such as coping, and mental health from the life-course perspective, which enables researchers to investigate the effects of internalized racism that racial/ethnic minorities experience (Mezuk et al. 2013). However, despite a growing body of research investigating the mechanisms that link early economic conditions and later health inequality, identifying whether the pathways operate similarly across racial groups from early life to young adulthood has been given limited attention.
Racially Contingent Pathways from the Life-course Perspective
Recent studies have examined whether there are racial differences in the association between early life socioeconomic disadvantage and adult health (Brown et al. 2012; Hargrove and Brown 2015; Richardson and Brown 2016). According to their explanations, the relationship between early life SES and later health outcomes is not similar across racial/ethnic groups in part because differential and cumulative exposure to stressors (e.g., institutional and interpersonal discrimination) place individuals on varying life trajectories (Hayward and Gorman 2004). For example, drawing on life-course perspectives such as cumulative disadvantage theory, Brown and his colleagues find that the relationship between early-life SES and later self-rated health is weaker for senior Blacks relative to White counterparts (Brown et al. 2012; Hargrove and Brown 2015). They further report that Black-White disparities in serious conditions, such as heart disease, increase during the 50s and early 60s and decrease through the early 70s. Their research suggests that racial disparities in physical health vary across health outcomes and life stages during late adulthood.
With respect to racial differences in mental health across the life course, however, few studies have examined how the pathways between early-life economic resources and later mental health are racially structured and which factors contribute to the racial differences in the pathways (Pavalko and Caputo 2013). Such questions speak to the complex interactions among class, race, and mental health within the life-course perspective. Previous studies have suggested that race structures important aspects of childhood and adolescence, which likely are related to mental health. For example, low-income Blacks often face “double jeopardy” because of institutional and interpersonal discrimination, which may lead to mental illness (Ferraro and Farmer 1996; Williams and Sternthal 2010), and it is plausible that this would affect parenting styles and family dynamics. However, others have found relatively small differences in adolescents’ daily lives and parenting styles across low-income Black and White groups (Lareau 2002). Moreover, although childhood and adolescence are critical/sensitive periods, the interaction effect of race and class on developing mental illness during the periods has not been examined clearly. In this regard, it is necessary to pay more attention to whether and how the pathways linking early economic conditions to depression vary according to race. In the following subsections, the mediating roles of family support and college enrollment are discussed, and their conditioning effects by race are proposed.
Parental income, family support, and depression by race
Family support covers a wide range of family characteristics, including the emotional support of children, responsive parenting, involvement in child activities, and cohesiveness within the family (Repetti, Taylor, and Seeman 2002). These relationships with family members are one of the key factors that influence children’s mental health in the short and long term because children’s experiences are closely linked with the family network where (dis)advantages can be transferred. Within the life-course literature, this is often referred to as linked lives (Elder 1998).
Although positive family support should foster good mental health, it is often difficult for low-income families to provide positive family support for two reasons. First, parental income is related to quality of parenting, which is a key factor affecting parents’ interactions with their children (McLanahan and Percheski 2008). Empirical evidence has shown that low parental income and economic hardship lead to punitive parenting practices (Yeung, Linver, and Brooks-Gunn 2002). Second, low income and financial insecurity influence parents’ psychological well-being adversely (largely via maternal depression), which is related to less engagement in child activity and yields poor parent-child relationships (Yeung et al. 2002). Therefore, poor family economic resources may be directly and indirectly related to diminished family support (Repetti et al. 2002).
Nevertheless, explorations of racial differences with respect to family structure and support have yielded mixed results in earlier literature. Some scholars found that Blacks’ extended-kin networks are stronger and more supportive than Whites’ family networks (Ellison 1990; Stack 1974) and that Blacks are more likely to exchange aid from their support networks than Whites (Taylor et al. 2013). However, others either argue that Whites tend to exchange more support within kin networks than Blacks or indicate that there are no racial differences in kin support networks (Hogan, Eggebeen, and Clogg 1993; Peek and O’Neill 2001; Raley 1995). Also, interactions of race, social relationships, and mental health remain unclear (Kiecolt, Hughes, and Keith 2008) because multiple factors, including population age and the types of support and kin groups being examined, may contribute to the mixed findings (Taylor et al. 2013).
With focusing on the child and adolescent population, Blacks’ extended family networks can provide strengths to support better child-rearing (McLanahan and Percheski 2008). It is especially helpful for households headed by poor single parents, given that two-parent families are less common among Blacks. Higher co-residence rates among Blacks also enable family members to have extended parenting and more instrumental and emotional support for children (Dominguez and Watkins 2003; Swartz 2009). The above distinct characteristics of Black families suggest that Black children living in low-income families may receive more care and attention from extended and supportive networks compared to White children in low-income families. For these reasons, associations between parental income and family support may be weaker for Black children compared to White children.
Parental income, higher education, and depression by race
Higher parental income often predicts the odds of adolescents’ higher educational attainment. Referred to as the “educational gradient” in health (Mirowsky and Ross 2003), higher educational attainment is associated with fewer symptoms of depression. Nevertheless, it should be noted that associations between parental income, education, and mental health may operate differently by race for two reasons. First, social circumstances related to racial discrimination decrease Black adolescents’ educational attainment, regardless of their parents’ economic resources. For example, Black students in White-dominant schools are more likely to report that they experience prejudice, and teachers’ biased expectations by racial stereotype widens the Black-White test score gap (Walsemann, Gee, and Ro 2013). These previous studies suggest a consequent decrease in college enrollment or completion among Black students, regardless of their early economic background. This is a potentially racialized mechanism that may weaken the negative association between parental income and depression for Black respondents, compared to that of Whites.
Second, buffering effects of education on health vary depending on where individuals are in the social hierarchy. That is, Blacks tend to get lower health returns with increases in educational attainment, which is referred to as the “diminishing returns” hypothesis (Farmer and Ferraro 2005). This unequal health benefit could be attributed to disadvantages from racial discrimination, which may be more noticeable in more highly educated Black groups. Institutional and interpersonal discrimination, racial prejudice and stereotypes, and internalized racism in public places all have been considered factors that may weaken or offset the effect of Black students’ educational attainment on their well-being (Brunsma, Embrick, and Shin 2017; Hayward et al. 2000; Williams et al. 2010). Taken together, more attention needs to be paid to the different roles of educational attainment between early economic condition and later mental health by race.
The Current Study
This study examines how parental income conditions the relationship between race and depression, which has not been exhaustively addressed in previous research (Pavalko and Caputo 2013). Four hypotheses are tested in this article. First, it is hypothesized that parental income predicts adolescents’ depression in adulthood, even after controlling for depression in adolescence. This study adjusts for adolescent depression as a lagged variable to address the temporal issue, which indicates that depression in adolescence may affect educational attainment and depression in adulthood (Winship and Morgan 2007). Second, because of institutional and interpersonal discrimination, Black respondents are expected to have a higher prevalence of depression in adulthood, holding all other variables in adolescence constant.
Third, higher income of White families is hypothesized to be related to higher family support, but in Black families, the process is not expected to work in the same way because the characteristics of Black families (i.e., care and support in the extended family network) may moderate the effects of parental income on family support. But as discussed in the literature review, the relationship between adolescent family support and higher adulthood depression is not expected to be moderated by race (Repetti et al. 2002).
Fourth, while high parental income leads to a greater possibility of college enrollment (which decreases the odds of adulthood depression among Whites), it is hypothesized that the mediating role of college enrollment is weakened or not observed in Black young adults. This may occur both because the positive effect of parental income on the odds of college enrollment is hampered by social circumstance surrounding Black adolescents and because college enrollment has a less protective effect on depression in Black respondents. To identify the specific roles of college enrollment across race, respondents’ adult household income (Wave 4) is also included as a mediator in the analyses.
Data and Methods
Add-Health is a longitudinal survey of a nationally representative sample of adolescents in grades 7 through 12, which began during the 1994–1995 school year. Add-Health data include social, economic, psychological, and physical well-being indicators with contextual data, and the school sample is a stratified random sample of all high schools in the United States. The Add-Health cohort has been followed into young adulthood with four in-home interviews (1994–1995, 1996, 2001–2002, 2007–2008); the most recent study (Wave 4) was in 2008 when the sample was 24 to 32 years old. This study merges Wave 1 and Wave 4 Add-Health data. While 20,745 students completed the in-home interview in Wave 1, 15,701 individuals completed the Wave 4 interview. Despite this attrition, an Add-Health report comprehensively demonstrated that the Wave 4 sample adequately represents the same population who responded at Wave 1 (Brownstein et al. 2012). Among 15,701 respondents in Wave 4, 10,824 are Black or White respondents with a sampling weight. This study additionally restricted the sample to respondents who do not have missing data on the set of covariates used in the analyses (n = 7,719), which is 71.3 percent of 10,824 respondents. Statistical analyses were adjusted for survey design using sampling weights, which account for the corrections for nonresponse and oversampling of Black adolescents with highly educated parents (Chen and Chantala 2014). More information about data structure is available on the Add-Health website (http://www.cpc.unc.edu/addhealth).
Second, college enrollment is dichotomized based on whether the respondents have some college or more status. The reason this study uses some college or more as a threshold is that respondents’ ages range from 24 to 32. According to a report from Complete College America (2014), the majority of college students do not complete their degrees on time, which suggests that some college students, especially in low-income families, may not have graduated college by the time of the Wave 4 survey. Therefore, those who have some college or more are coded 1, and less than college are coded 0. Additional analyses using college degree or more are conducted as a sensitivity check, which does not alter the main findings. Last, adult household income is included as a third mediator to identify the distinctive role of college enrollment. It is measured using a top-coded ordinal scale (from less than $5,000 to $150,000 or more) in Wave 4, which is different from the continuous measure of parental income in Wave 1. Despite the difference, to keep consistency between income measures in the two periods, the log-transformed midpoint (in thousands of dollars) of each category in Wave 4 is considered.
Analytic Strategy
In this study, Hypotheses 1 through 4 are tested mainly using two sets of analyses. First, logistic regressions are used to model the association between parental income, race, and depression in adulthood for the total sample and then separately for White and Black respondents. It assesses the effects of parental income on adult depression by race and analyzes whether Black respondents experience fewer symptoms of depression after controlling for other variables (see Table 3). Second, using KHB’s “khb” Stata module (Breen, Karlson, and Holm 2013), this study examines whether the two mediators, the level of family support and college enrollment, are on the causal pathways between parental income and depression in adulthood. It is important to decompose the total effect of parental income on depression into direct and indirect effects to better understand how family support and college enrollment differently mediate this link by race. To identify the net effect of each mediator, the KHB model estimates the mediating effects of family support, college enrollment, and adult household income together in one model (see Table 4).
The newly developed KHB method has two advantages over the conventional mediation methods. First, while conventional mediation analysis cannot decompose the total effect into direct and indirect effects when the outcome variable is not continuous (Baron and Kenny 1986), the KHB method can be applied to nonlinear probability models (Breen et al. 2013). All effects (direct, indirect, and total) are measured on the same scale with the KHB method even when the outcome of interest is dichotomized like in this study (i.e., depression = 1, not depression = 0). In contrast, with the conventional mediation methods, the error variance in nonlinear probability models varies across models, which leads to scale identification issues’ appearing when researchers compare the coefficients of the total, direct, and indirect effects.
Second, while most conventional mediation methods allow only one mediator (Hayes 2013), the KHB method can not only accommodate multiple mediators at the same time but also control for potential confounding variables. This makes it possible to investigate the unique role of each mediator after taking into account other mediators and confounding variables. Therefore, the KHB mediation analysis is the most appropriate method to elucidate the racially patterned mechanisms from parental income to adult depression via family support and college enrollment. The more detailed advantages of the KHB method for mediation analysis are thoroughly described elsewhere (Breen et al. 2013). To statistically identify the racial differences in the mediation processes, moderation analyses using interaction terms were conducted, and their results are presented in Figures 1 and 2.
Results
Descriptive Statistics
Table 1 presents the weighted descriptive statistics for the analytic sample, stratified by race. As shown in the Race Difference column in the table, all the differences across the White and Black sample are significant at the .05 level or higher. To be specific, first, it shows a significantly higher proportion of depression in adulthood for Black respondents (26 percent) in comparison to White respondents (17 percent). Second, Black respondents are more likely to have lower SES than Whites. For example, Black families tend to earn roughly $11,000 (adjusted for by the number of family members) less than White families (exp(3.12) − exp(2.40) = 22.65 − 11.02), and approximately 58 percent of Black respondents enroll in college, compared to 69 percent among Whites. Third, Black respondents tend to have slightly better family support (16.30) than their White counterparts (16.09), with a statistically significant racial difference. This result indicates that Black adolescents generally have been exposed to greater socioeconomic disadvantage than Whites but that factors related to family support may play a different role in children’s lives.
Weighted Means or Proportions for Measures of Variables by Racial Group, National Longitudinal Study of Adolescent to Adult Health.
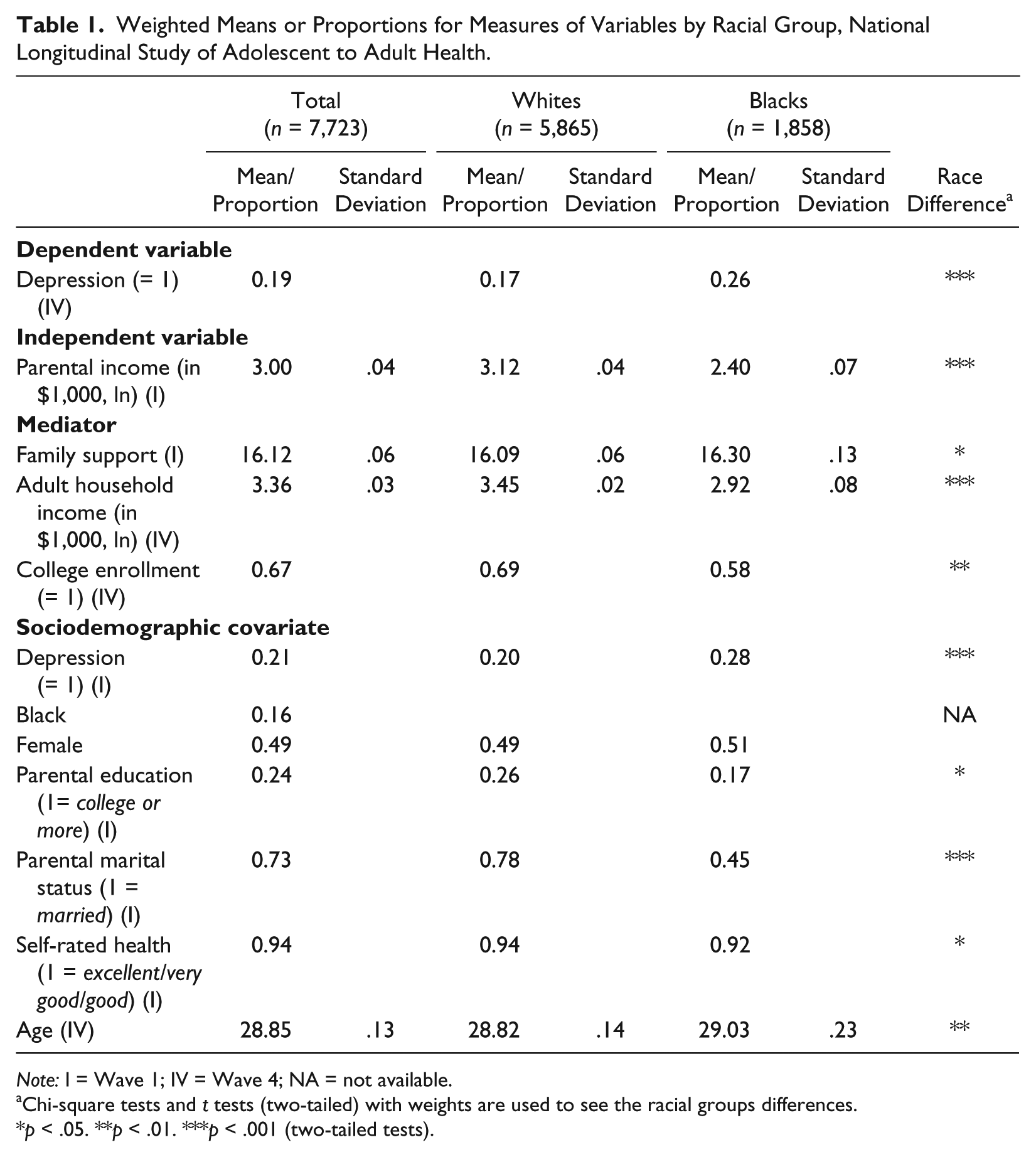
Note: I = Wave 1; IV = Wave 4; NA = not available.
Chi-square tests and t tests (two-tailed) with weights are used to see the racial groups differences.
p < .05. **p < .01. ***p < .001 (two-tailed tests).
Before testing for mediation effects, it is necessary to establish that the proposed mediators are in fact sensitive to the independent variable of parental income. These results are presented in Table 2. In Model (1) in Table 2, after adjusting for all adolescent background and demographic covariates, it is determined that parental income is not related to family support in the total sample. However, this null pooled estimate reflects significant associations that run in opposing directions in the White and Black subsamples. While the effect of parental income on family support is significantly positive among Whites, the effect is significantly negative on family support among Black adolescents. This implies that there are racial differences in the association between parental income and family support in adolescence. In Models (2) and (3) in Table 2, high parental income in adolescence is positively related to higher adult household income and a greater probability of college enrollment in wave 4. It is consistent with evidence that childhood SES has long-term effects on adulthood SES (Blau and Duncan 1967).
Parental Income and Three Mediators by Race, Adjusted for All Covariates, National Longitudinal Study of Adolescent to Adult Health.
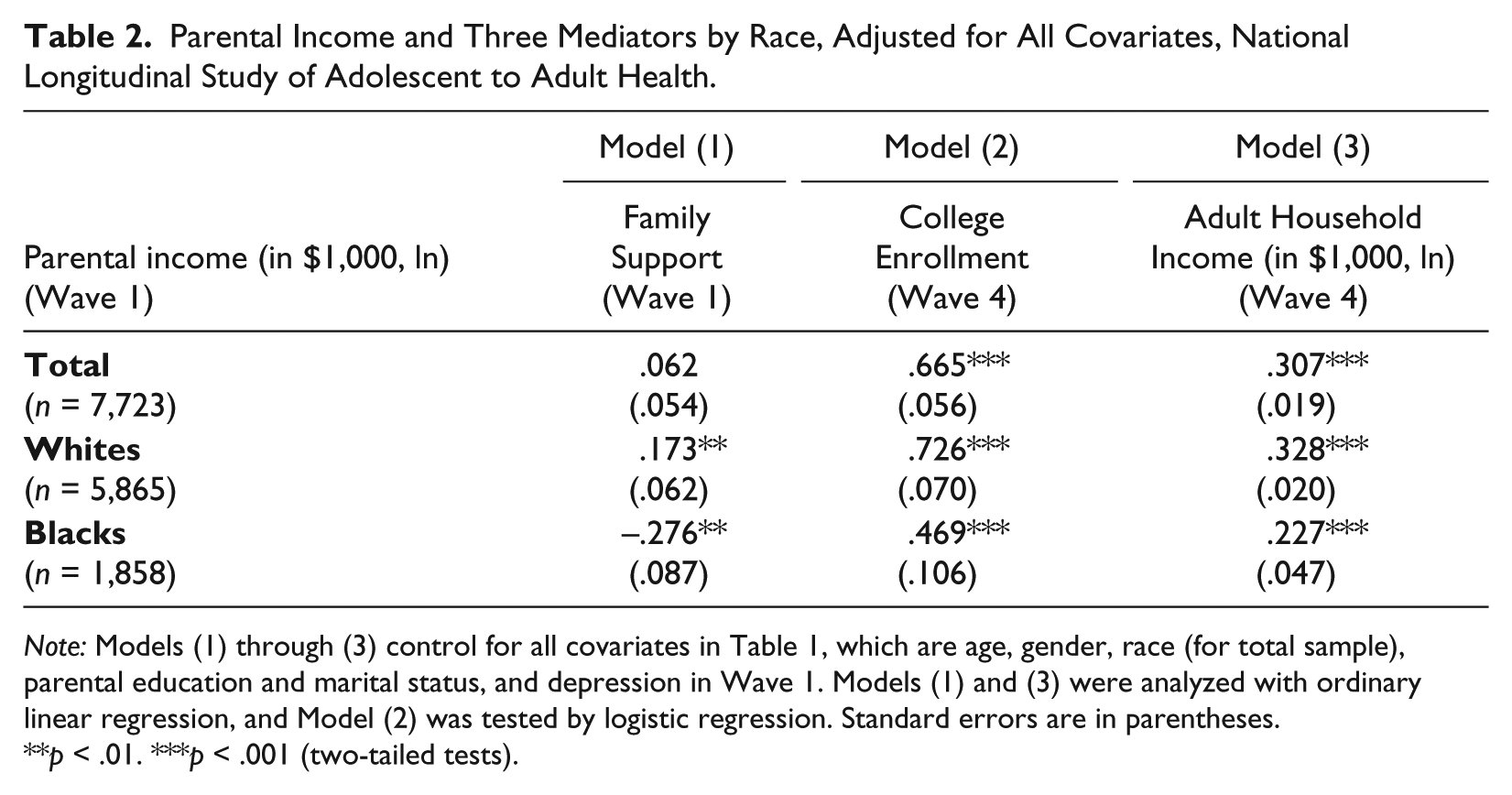
Note: Models (1) through (3) control for all covariates in Table 1, which are age, gender, race (for total sample), parental education and marital status, and depression in Wave 1. Models (1) and (3) were analyzed with ordinary linear regression, and Model (2) was tested by logistic regression. Standard errors are in parentheses.
p < .01. ***p < .001 (two-tailed tests).
The Effects of Parental Income on Adult Depression, by Race
First, logistic regressions are employed to test whether parental income predicts adult depression after controlling for depression in adolescence (first hypothesis). Model (1) in Table 3 presents associations between adult depression and parental income, adjusting for adolescent depression and Black racial status. Specifically, a one-unit increase in parental income (in $1,000, ln) decreases the odds of depression in adulthood by 24.2 percent (= 100 × [1 − exp(–.277)]). In Model (2), after holding constant key demographic variables and other adolescent background characteristics, which are expected to affect depression, the relationship between parental income and adult depression does not change. Model (3) includes the three mediators of family support in adolescence, college enrollment, and adult household income. After taking the mediators into account, parental income is no longer a significant predictor of adult depression, which suggests that the three mediators mediate the largest amount of parental income effects on depression.
Logistic Regression Models Predicting Depression in Adulthood, National Longitudinal Study of Adolescent to Adult Health.
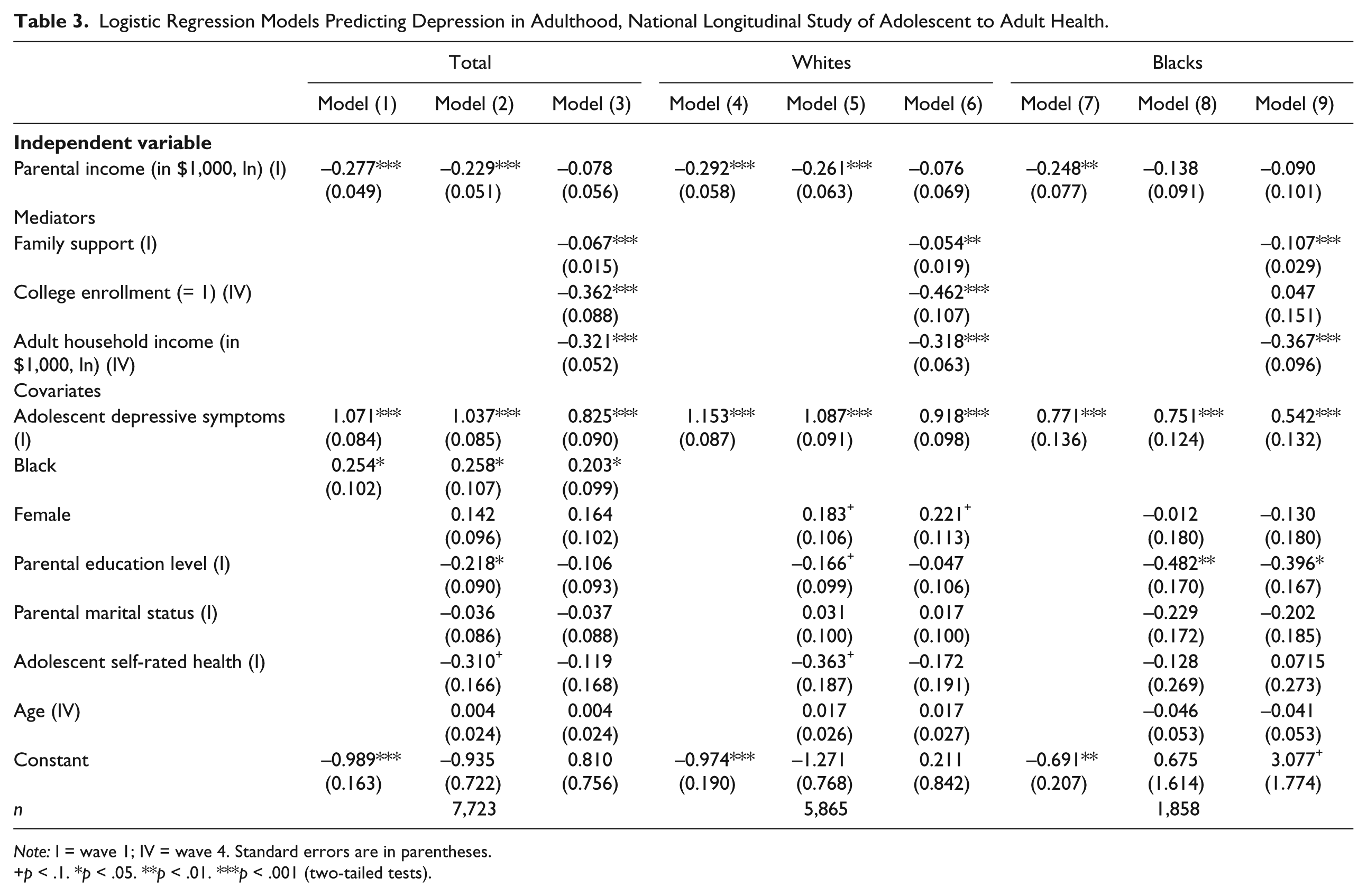
Note: I = wave 1; IV = wave 4. Standard errors are in parentheses.
p < .1. *p < .05. **p < .01. ***p < .001 (two-tailed tests).
Second, the effect that Black racial status has on adult depression (second hypothesis) is tested. In Models (1) and (2) for the total sample in Table 3, Black respondents are roughly 29 percent more likely to have adult depression, compared to Whites. This is a net difference between Blacks and Whites because the models control for adolescent variables. After holding constant the three mediators in Model (3), racial differences between Blacks and Whites are partly explained by the three mediators but are still significant. Overall, these results are consistent with previous literature, suggesting that parental income and race play independent roles in developing depression.
Before examining the racial differences in the mediation effects of parental income, Model (4) through Model (9) present race-stratified estimates. Although many covariates are not significant because the models control for adolescent depression, the race-stratified models show consistent results with the full sample. To be specific, in Models (6) and (9), the direct effect of parental income loses its statistical significance because the effect of parental income on adult depression is mainly transmitted via the mediators. This is consistent with the results for the total sample in Model (3). Among Whites in Model (6), a one-unit increase in family support results in a 5.3 percent decrease in the odds of depression, while college enrollment decreases the odds of depression by 37.0 percent and a one-unit increase in adult household income decreases the odds of depression by 27.2 percent. However, among Black respondents, while family support and adult household income strongly decrease adult depression, college enrollment does not. Also, Blacks’ parental education (= college or more compared to less than college) still significantly decreases the odds of adolescents’ later depression, even after controlling for the three mediators. This suggests that parental education level among Black adolescents has an independent effect on their later mental health.
Decomposition of Total Effect of Parental Income into Direct and Indirect Effects through Mediators, by Race
In this section, the KHB method is employed to decompose the total effect of parental income into direct and indirect effects and to examine the specific roles of family support in adolescence and college enrollment and adult household income. In Table 4, the top panel shows the decomposition of the total effects into direct and indirect components, and the bottom panel shows the unique contribution of each mediator of the indirect effects. Note that all of the control variables in Table 3 were used in the KHB analysis, but only the mediation analysis results were presented in Table 4.
Decomposition of the Total Effect of Parental Income into Direct and Indirect Effects on Depression through Mediators, National Longitudinal Study of Adolescent to Adult Health.
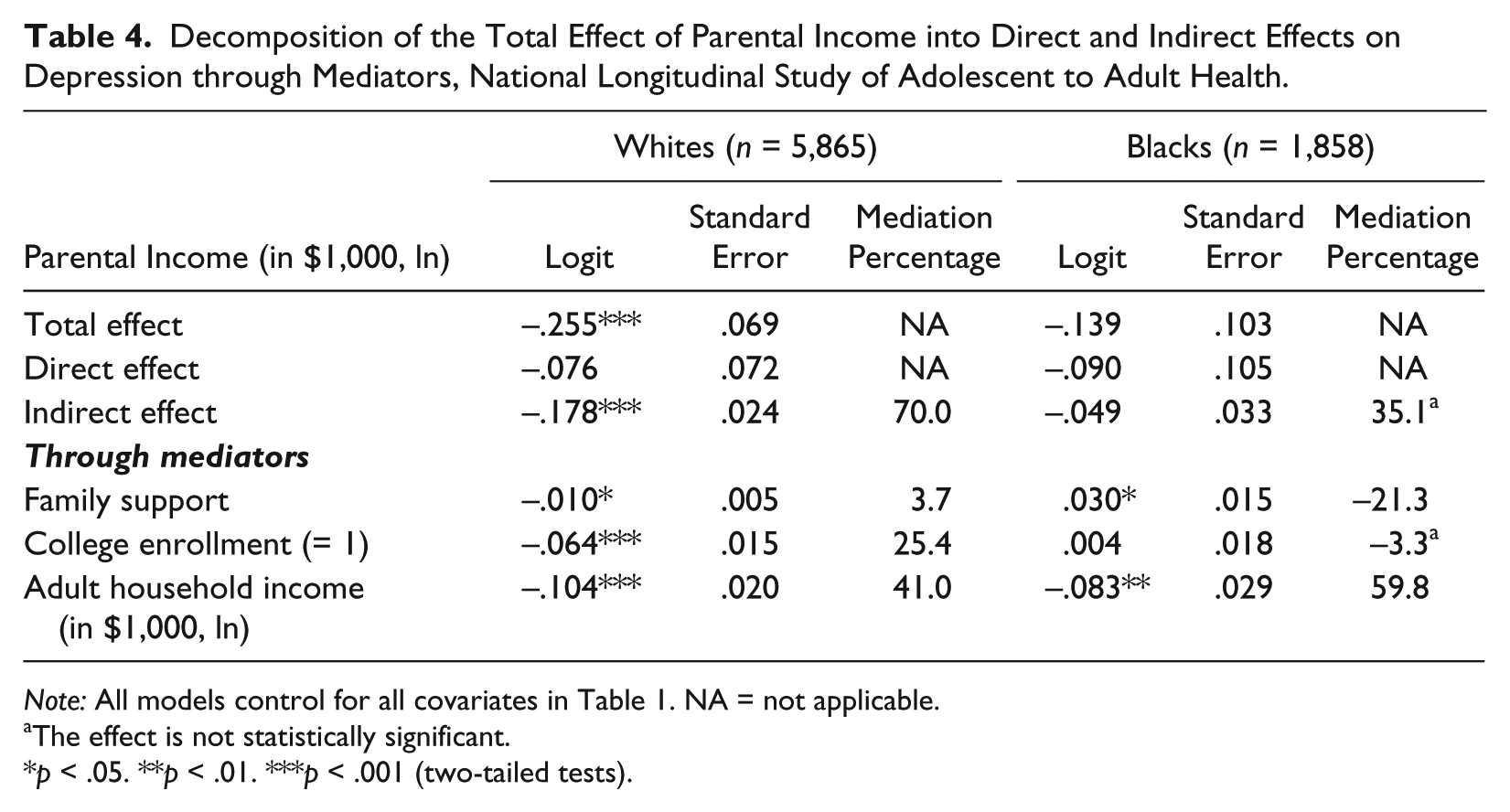
Note: All models control for all covariates in Table 1. NA = not applicable.
The effect is not statistically significant.
p < .05. **p < .01. ***p < .001 (two-tailed tests).
According to the KHB result in Table 4, a one-unit increase in parental income among Whites significantly decreases the odds of depression by 22.5 percent (= 100 × [1 − exp(–.255)]) in total, with 16.3 percent of that total effect operating through indirect pathways (= 100 × [1 − exp(–.178)]). Since most of the parental income effect is transmitted to adult depression through the three mediators (70.0 percent), the direct effect of parental income is not significant. In contrast, the total, direct, and indirect effects of parental income among Black respondents are not significant. Nevertheless, racial differences in the specific roles of family support and college enrollment as mediators, which test Hypotheses 3 and 4, are apparent in the lower panel.
First, the lower panel of results in Table 4 shows evidence about whether family support differently mediates the effect of parental income on adult depression by race (third hypothesis). While the coefficient of family support among Whites is significantly negative, the coefficient for Black respondents is significantly positive. Since parental income is expected to increase family support and higher family support tends to decrease the odds of depression, the coefficients of parental income through family support are generally expected to be negative, as seen in the White sample (β = −.010 in Table 4). However, because higher parental income decreases family support in Black adolescents as seen in Table 2, and higher family support decreases the odds of depression in Table 3, the overall direction of mediation effect is significantly positive (β = .030) among Blacks. This indicates that among Black respondents, the indirect effect of parental income via family support significantly increases the odds of adult depression by 3.0 percent (= 100 × [1 − exp(.03)]). This is the reason the mediation percentage of family support is −21.3 percent, which indicates that family support influences depression in the opposite way to the total effect of parental income. This KHB result is also consistent in a model with imputed variables, which indicates that missing data do not alter the main findings (available upon request).
Considering the relationships between adolescent family support and adult depression are negative in both race groups in Models (6) and (9) in Table 3, this racial difference in the mediating role of family support may be derived from the relationship between parental income and family support. To confirm this argument, this study employs a moderation analysis by including an interaction term of parental income and race, which is presented in Figure 1 (regression results including interaction terms are available upon request). Figure 1 graphically illustrates this interaction and presents a result that is consistent with the third hypothesis. Among low-income families, predicted family support is higher for Black adolescents relative to Whites. In contrast, among high-income families, predicted family support is lower for Black adolescents compared to Whites. The interaction effect of race and parental income on family support is statistically significant (β = −.502; p < .001; regression results including interaction terms are available upon request). That is, as parental income increases, White adolescents tend to experience more family support, but Black adolescents experience less. Given that family support significantly decreases the probability of adult depression in both races, this racial difference in the effects of parental income on family support produces disparities in mental health.
Second, the lower panel of results in Table 4 presents analyses examining the racially contingent role of college enrollment (fourth hypothesis). Adult household income (Wave 4) is also included as a mediator in the KHB model, which allows for comparison of the mediating roles of adult household income and college enrollment in adulthood across race. Among Whites, college enrollment mediates a relatively similar extent as adult household income (25.4 percent for college enrollment and 41.0 percent for adult household income) of total parental income effects. Among Black respondents, adult household income mediates 59.8 percent of parental income effects on adult depression; however, college enrollment plays a nonsignificant mediating role. This decomposition result suggests that parental income is differently transmitted to adolescents’ depression via college enrollment by race. Though the parental income effect was positively related to college enrollment among both Blacks and Whites (see Table 2), Black adolescents’ college enrollment does not ensure a decrease in the odds of depression in adulthood (see Table 3).
Figures 2(a) and 2(b) illustrate the racially conditional roles of college enrollment in the pathways from parental income to adult depression in detail, which are consistent with the fourth hypothesis. Based on the ad hoc moderation analyses presented in Figures 2(a) and 2(b) (regression results, including interaction terms, are available upon request), race moderates the effect of parental income on the odds of college enrollment and moderates the effect of college enrollment on adult depression. In detail, as parental income increases, Whites are more likely to have a greater probability of college enrollment than Black respondents when parental income is higher than about $29,960 (exp(3.4) = 29.96, approximately $29,960) (see Figure 2(a); β = −.233; p < .1; regression results, including interaction terms, are available upon request). Moreover, even when Black respondents have college enrollment, it has a weaker association with the odds of depression, in contrast to Whites (see Figure 2(b); β = .396; p < .05; regression results are available upon request), which statistically supports the diminishing returns hypotheses. In sum, the effects of parental income through college enrollment exert little influence on adult depression among Black respondents.

Moderating effects of race and parental income on the level of family support.
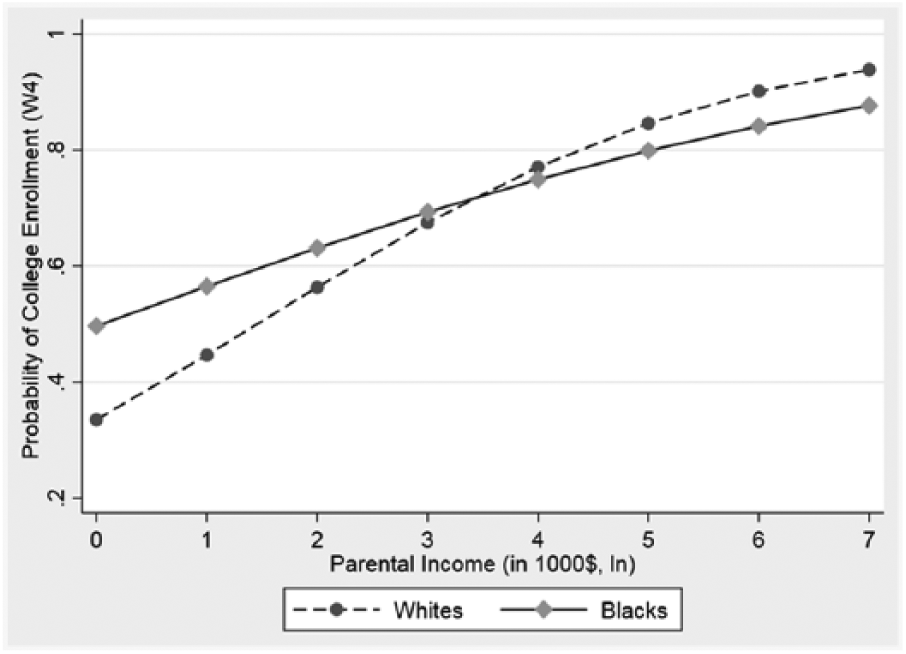
Moderating effects of race and parental income on the predicted probability of college enrollment.

Moderating effects of race and college enrollment on the predicted probability of depression.
Discussion
Drawing on the life-course perspective, this study examines how parental income is transmitted to adult depression and elucidates racially patterned mechanisms by exploring mediators contingent on race. The results from logistic regressions and KHB mediation analyses generally support the four hypotheses of this study. First, after adjusting for depression in adolescence and other adolescent background variables, higher parental income generally decreases the odds of depression in early adulthood. Second, Black respondents tend to have higher levels of depression in adulthood, holding all covariates in adolescence constant. This suggests that Black respondents are more likely to suffer from depression in early adulthood even when they have adolescent backgrounds similar to Whites’ including parental income as well as adolescent mental and physical health. These first and second findings highlight the role of adolescent economic condition in developing mental health inequality and echo the previous results showing Blacks’ disadvantage in depressive symptoms (Williams et al. 2010). In sum, with regard to the CES-D measure, this study does not find a Black-White paradox in mental health, which partially supports previous studies (Jackson et al. 2010).
Third, while higher parental income among Whites brings about higher family support, Blacks’ higher parental income tends to decrease family support (see Figure 1). This indicates that higher parental income may not necessarily ensure lower depression in Black respondents, even though higher family support leads to lower depression when Black and White subgroups are combined. One explanation for this tendency is that Black families are likely to maintain extended family networks (Swartz 2009), especially when parental income is low. Further investigation (available upon request) shows that higher parental income is significantly related to fewer family members among Black adolescents (p < .001), which may be correlated with less family support. That is, Black children in nuclear and high-income families may lose important resources of family support. This racial heterogeneity in the effects of parental income on family support may be one of the reasons income’s effects on family or social support have mixed and insignificant results in the previous research (Aneshensel 2009). Taken together, this result requires a more in-depth understanding about the association between family social class and family support, which has potential as a promising intervention target.
Fourth, among Whites, higher parental income decreases the odds of depression via college enrollment. On the other hand, among Black respondents, the income effects through college enrollment do not exert influence on adult depression, which supports evidence discussing unequal health benefits from socioeconomic resources (Williams et al. 2010). Based on Figure 2(a), the effects of parental income on college enrollment among high-income Blacks are significantly lower than those among high-income Whites. Additionally, Blacks’ college enrollment does not significantly decrease the odds of depression when holding other covariates constant, while more education among Whites clearly decreases the odds of depression (Figure 2(b)). Racialized gaps in disadvantage from these pathways are more obvious among more socioeconomically advantaged Black adolescents (i.e., adolescents raised in high-income families and/or highly educated Blacks). This suggests that the racial disadvantages (i.e., discrimination) that highly educated Blacks face may block the effective deployment of socioeconomic resources; thus, institutional and interpersonal discrimination need to be addressed simultaneously.
In sum, these findings point to the conclusion that Black families’ higher parental income does not always ensure better adult mental health of Black adolescents, compared to their White counterparts. In certain conditions, higher income in Black families does not improve adolescents’ mental health in adulthood. Race moderates the effect of family economic resources on later mental health, especially in middle-income or affluent Black families, and these differences may contribute to the persistence of mental health disparities by race. Meanwhile, White children in low-income families also need to be paid more attention. As Figures 1 and 2(a) illustrate, White children in low-income families tend to receive less family support than not only White children in high-income families but also Black children in low-income families. This implies that we need to address the differential transmission of inequalities that Black and White children may face across their life courses.
Limitations and Future Research
This study is subject to several limitations. First, it is possible that selection bias and measurement error contribute to the differences between Blacks and Whites in terms of depression in this study. Given that Blacks are disproportionately institutionalized with a greater number excluded from household samples, selection bias may affect racial differences in depression (Barnes and Bates 2017). Also, existing measures may not adequately capture depression in Blacks compared to Whites, because it is possible that Blacks tend not to endorse questions about depression using the same criteria as Whites (Breslau et al. 2008; Brown 2003). However, previous research found that both the selection bias and measurement error explanations are insufficient to explain the patterns of Black-White disparities in mental health (Barnes and Bates 2017; Mezuk et al. 2013).
Nevertheless, it should be noted that the CES-D measure of depression used in this study may not be a valid indicator for use in race and ethnic comparison (Perreira et al. 2005). Using Add-Health data, Perreira and her colleagues suggested an abbreviated five-item version of the CES-D (i.e., depressed, sad, blues, happy, and enjoyed life) to correctly measure the level of depression across racial and ethnic groups. I reanalyzed the results of this study with the abbreviated CES-D measures and found results substantively similar to those presented above (full results are available upon request). This echoes epidemiological research showing that the dichotomized CES-D indicates a clinical diagnosis of depression and provides high internal consistency and reliability among diverse racial/ethnic populations (Bromberger et al. 2004).
Second, although trajectories of mental health during the transition to adulthood are important parts of the life-course perspective, this study is not able to explicitly examine the trajectories. Future research may analyze the trajectories of depression during adolescence and young adulthood, focusing on the effects of individual and contextual characteristics, such as sociodemographic factors, health behaviors, and neighborhood contexts (Adkins et al. 2009; Boardman and Alexander 2011). Mobility from low SES to high SES and the racial differences in developing depression may be topics of future research as well.
Third, this study operationalized college enrollment as higher educational attainment because the majority of college students do not complete their degrees on time (Complete College America 2014) and respondents’ ages in this study range from 24 to 32. Nevertheless, further investigation using college completion shows similar racial differences in the roles of mediators (available upon request). Finally, although racial discrimination is considered an important factor explaining why Blacks’ college enrollment does not diminish the odds of depression, it cannot be directly tested using Add-Health data because it does not include a racial discrimination variable. Further investigating the effects of racial discrimination on mental health with appropriate data can be an avenue for future research.
In spite of these limitations, drawing on the life-course perspective, the findings reported in this study enhance our understanding of whether depression is the outcomes of early-life disparities and how family support and college enrollment differently contribute to the development of mental health disparities by race. Also, this study employs a KHB mediation analysis to parse out the direct and indirect effects of parental income with the well-suited Add-Health data set, which is a nationally representative cohort survey. These results enable researchers and policy makers to consider how the trajectory from class to mental health can be differently shaped by race, which may provide race- and class-specific solutions to mental health problems.
Footnotes
Acknowledgements
I acknowledge assistance from the Center for Social and Demographic Analysis at the University at Albany, State University of New York, which receives core funding from Eunice Kennedy Shriver National Institute of Child Health and Human Development (R24-HD044943). A previous version of this article was presented at the 2015 American Sociological Association meeting. For suggestions and criticisms, I thank Lei Lei, Jeffrey Napierala, Benjamin Shaw, Kate Strully, Katherine Trent, Colleen Wynn, Tse-Chuan Yang, and three anonymous reviewers.