
Abstract
Skin tone is a status characteristic used in society to evaluate and rank the social position of minorities. Although skin color represents a particularly salient dimension of race, its consequences for health remains unclear. The author uses four waves of panel data from the Coronary Artery Risk Development in Young Adults study and random-intercept multilevel models to address three research questions critical to understanding the skin color–health relationship among African American adults (n = 1,680): What is the relationship between skin color and two global measures of health (cumulative biological risk and self-rated health)? To what extent are these relationships gendered? Do socioeconomic characteristics, stressors, and discrimination help explain the skin color–health relationship? The findings indicate that dark-skinned women experience more physiological deterioration and self-report worse health than lighter skinned women. These associations are not evident among men, and socioeconomic factors, stressors, and discrimination do not explain the dark-light disparity in physiological deterioration among women. Differences in self-ratings of health among women, however, are generally explained by education and income. The results of this study highlight heterogeneity in determinants of health among African Americans. They also provide a more nuanced understanding of health inequality by identifying particularly disadvantaged members of racial groups that are often assumed to have monolithic experiences.
Racial health inequality in the United States has received considerable attention in the social sciences. Compared with whites, African Americans are disadvantaged across an array of outcomes, including objective (i.e., physiological markers) and subjective (i.e., self-rated) measures of health (Brown et al. 2016; Cobb et al. 2016; Duru et al. 2012). Research also suggests that racial disparities in physical health are gendered, as black-white differences tend to be larger among women compared with men (Hargrove 2018; Umberson et al. 2014; Warner and Brown 2011). Although the racial stratification of health is well documented, a majority of studies have been unable to completely explain the health gap between African Americans and whites, even when accounting for various socioeconomic and psychosocial factors (Brown et al. 2016; Sternthal, Slopen, and Williams 2011). The inability of previous studies to explain the health disadvantages of African Americans may be due to the untenable assumption that African Americans as a whole are affected by social factors in an equivalent manner and therefore experience similar patterns of health. This assumption masks potential intraracial heterogeneity in health, as well as health-relevant risks or resources that may be unique to this population subgroup.
One line of research to address this limitation is to examine the health consequences of skin tone among African Americans. Skin tone represents a salient dimension of race that has received less attention in health disparities research than other indicators of race, such as self-identification (Roth 2016). 1 A long tradition of scholarship shows that individuals with lighter skin are awarded social and economic privileges because of their closer phenotypic resemblance to whites and their assumed superior social value relative to their darker skinned counterparts (Dixon and Telles 2017; Hunter 2007). Although research has documented skin color stratification in various aspects of life among African Americans, particularly socioeconomic status (SES; Monk 2014), less is known about the significance of skin color for one of the most crucial determinants of life chances: health. Past research has tended to examine a single outcome (namely, blood pressure), rely on cross-sectional data, and focus on SES as the primary mechanism linking skin color and health. Missing from the literature are therefore recent and systematic investigations of the relationship between skin tone and health, broadly assessed (for an exception, see Monk 2015). This is a particularly pressing topic for social scientists given that recent population trends (e.g., increases in nonwhite immigration and interracial unions) are altering the racial structure in the United States and potentially placing greater emphasis on skin color as a marker of stratification and determinant of life chances (Bonilla-Silva and Dietrich 2010). Although skin complexion has always been consequential among African Americans, changes in the social hierarchy hold significant implications for future health profiles of this group as well as the nature of intra- and interracial inequality.
Furthermore, insufficient attention has been given to examining how skin color may intersect with other dimensions of stratification to shape health, particularly gender. Health disparities research tends to treat systems of inequality (and their consequences) as independent of one another, resulting in approaches that either examine marginalized statuses individually or assume that the poor health of multiply disadvantaged individuals is due to the sum of the health risks associated with each status. Although informative, these types of approaches mask the positions of power and disadvantage within which individuals are simultaneously situated (Collins 2015; López and Gadsden 2016). Studies relying on independent or additive approaches may therefore over- or underestimate health inequalities or overlook groups that are most at risk.
Efforts to reduce health inequalities require increased knowledge of the unique determinants of health among diverse social groups. To aid in this effort, the present study addresses three research questions critical to understanding how skin color is related to physical health among African American adults: What is the relationship between skin color and indicators of overall health? To what extent are these relationships gendered? Do socioeconomic characteristics, stressors, and discrimination help explain the skin color–health relationship? To address these questions, I examine differences in cumulative biological risk (CBR) and self-rated health among African American women and men aged 32 to 55 years using the Coronary Artery Risk Development in Young Adults (CARDIA) study. The findings will offer critical insight into the pathways linking skin color to poor health throughout adulthood.
Background
Colorism in the United States
Research has long found that the hue of one’s skin significantly structures access to opportunities and desired resources above and beyond traditional measures of race (Drake and Cayton 1945; Monk 2014). Originating from slavery and European colonialism, colorism is a system of stratification that derives from racism; it is inextricably linked to hegemonic beliefs in the social superiority of whites over all other racial groups (Hunter 2007). Colorism therefore constitutes an ideological and structural system of inequality that affords special advantages to lighter skinned minorities because of their closer phenotypic resemblance and presumed genetic similarity to Europeans and, therefore, to Eurocentric standards of beauty, morality, intellect, and status (Dixon and Telles 2017; Russell, Wilson, and Hall 1992). Although skin color represents a salient dimension of race, the processes through which it shapes health and well-being among African Americans is both related to and distinct from those of race (Hunter 2007). That is, the experience, nature, and consequences of institutional racism and interpersonal discrimination differ among those with lighter versus darker skin. For example, scholarship has consistently found that despite African Americans’ limited access to social, economic, and political resources as a whole relative to whites, light-skinned blacks are more advantaged than their darker skinned counterparts in the labor market (Monk 2014; Wade, Romano, and Blue 2004), criminal justice system (White 2015), perceived personal attributes such as attractiveness, intelligence, and morality (Adams, Kurtz-Costes, and Hoffman 2016; Maddox and Gray 2002), and, to a lesser extent, exposure to discrimination (Monk 2015; Uzogara et al. 2014). At times, the magnitude of skin tone inequalities among African Americans is similar to the magnitude of black-white disparities (Goldsmith, Hamilton, and Darity 2007). These findings suggest the existence of “light (skin) privilege” in which individuals and social institutions unequally afford opportunities and assign social power to minorities according to indicators of status (e.g., skin tone) other than assumed race (Hill 2002b; Hughes and Hertel 1990). Skin tone therefore represents an entrenched status characteristic both related to, and distinct from, race.
Prior research also suggests that the nature of colorism is gendered, with skin complexion being more consequential for black women’s lives than black men’s (Dixon and Telles 2017; Hill 2002b; Monk 2014). Intersectionality theory provides a lens through which to understand how fair skin may afford special advantages and opportunities to African American women in ways that it does not for men. Specifically, intersectionality posits that social inequalities are simultaneous and interdependent. They can combine in multiplicative rather than additive ways to mutually construct one another and structure unique social contexts that frame lived experiences and life chances (Collins 2015). Individuals situated at similar locations in the social structure therefore have shared, yet distinct social realities (López and Gadsden 2016). Indeed, scholars have noted that as a result of its intersection with sexism, forms and consequences of colorism vary by gender (Hill 2002b). For example, physical appearance and perceived attractiveness are critical components of socioeconomic success for women of all races living in a patriarchal society (Anderson et al. 2010; Hamermesh 2013). Beauty can be a substitute for, or considered equivalent to, ability or other characteristics employed by men (e.g., intelligence, political influence) to increase their life chances (Fletcher 2009; Lakoff and Scherr 1984; Wolf 1991). As a result, beauty—defined in the United States by fairer skin and other indicators of European features—is a form of capital for women (Hunter 2007). For African American women in particular, light skin acts an additional form of capital that can be used to accumulate more social and economic resources relative to their darker skinned female counterparts and black men (Hunter 2007; Monk 2014).
Similarly, skin tone may be more consequential for women than men because of its role in mate selection (Dixon and Telles 2017; Drake and Cayton 1945). Marriage is one mechanism through which socioeconomic position may be enhanced, particularly for women (Dixon 2009). Upward mobility via marriage to high-status partners may be a more relevant factor for African American women’s health than men’s, as these women experience disproportionately high rates of socioeconomic disadvantage that translate into few resources (e.g., income, wealth, power) for promoting health (Brown 2016; Chang and Lui 2010). Prior work indicates that light-skinned black women are more likely than their darker skinned counterparts to marry men of greater SES because of the more favorable characteristics associated with fair skin, including attractiveness, femininity, and morality (Keith and Herring 1991; Hamilton, Goldsmith, and Darity 2009). Thus, the advantage lighter skinned women have in marriage can increase their access to socioeconomic resources. These resources may not only improve healthy living and reduce exposure to health risks, but also lessen the potentially negative impacts of the absence of other health promoting resources (Ross and Mirowsky 2006). Taken together, the intersections of race, skin color, and gender may differentially shape the role of skin tone in structuring health among African American women and men.
The Relationship between Skin Tone and Health
Although prior work documents the continued existence of skin tone stratification among African Americans (e.g., Monk 2014), one area that has been particularly understudied is the relationship between skin tone and physical health. Given that, similar to racism and sexism, colorism structures access to resources and exposures to risks (Dixon and Telles 2017), skin color likely constitutes a significant determinant of health. Extant research, however, provides modest evidence of a relationship between skin tone and physical well-being among African Americans. Overwhelmingly, previous studies have focused on a single outcome, finding that dark skin complexion is associated with increased risk for high blood pressure or hypertension among African Americans (Boyle 1970; Harburg et al. 1978). These associations are, at times, explained by SES (Keil et al. 1977, 1981) or are significant only among those of lower SES (Klag et al. 1991).
More recent research, however, has produced mixed results. For example, two studies have used the CARDIA data to examine the relationship between skin color and health measured at one point in time among African American adults. One study revealed no significant association between skin color and self-rated physical health (Borrell et al. 2006), while the other documented a significant skin color gradient in systolic blood pressure (Sweet et al. 2007). Results from the latter study also suggested a significant negative association between income and systolic blood pressure among lighter skinned African Americans only; the association between income and blood pressure was not significant among dark-skinned African Americans. Furthermore, using a nationally representative sample of Black Americans, Monk (2015) found that African Americans who self-reported having darker skin had significantly higher odds of hypertension compared with their light-skinned counterparts. This relationship remained significant when accounting for several sociodemographic characteristics and experiences of racial and skin color discrimination. Similarly, Cobb et al. (2016) reported a skin color gradient in markers of physiological functioning among African American adults living in Nashville, Tennessee that was not explained by socioeconomic resources.
Although recent scholarship provides critical insight into the physical health consequences of skin color, several limitations should be addressed to advance this literature. First, prior work has tended to focus on specific measures of physical health, leaving unclear how skin tone might shape broader indicators of health and well-being. Focusing on specific disorders or conditions not only limits our understanding of the far-reaching health consequences of the social world, but also potentially misclassifies individuals as healthy when they are sick or at risk for becoming unhealthy according to another indicator of health (Aneshensel 2005). The magnitude of health inequality between social groups may therefore be underestimated when basing such conclusions on studies that examine singular health outcomes.
Second, current research tends to aggregate the entire African American sample, precluding an investigation of whether the associations between skin tone and physical health vary by gender. Prior work suggests that race and gender combine in ways that produce alternating health disadvantages within the African American population. Black women, for example, tend to have worse functional health, are at increased risk for several chronic illnesses, and are more likely to experience accelerated physiological aging compared with black men (Brown and Hargrove 2013; Erving 2011; Geronimus et al. 2006; Hargrove 2018; Monk 2015). Black men, however, have consistently higher mortality rates and lower life expectancies than black women (National Center for Health Statistics 2017; Xu et al. 2016). These patterns can be attributed to the unique stressors and experiences that characterize the lives of black women and men—experiences that are structured, in part, by behaviors and expectations stemming from racialized notions of femininity and masculinity (Courtenay 2000; Goff, Thomas, and Jackson 2008; Griffith 2012). Less understood, however, is how skin color might differentiate the health consequences of gender among African American women and men. Given that skin color helps pattern distinct social realities among the African American population, the consequences of race and gender may be further conditioned by skin tone. Such an empirical question will be addressed in the present study.
Third, prior work generally relies on cross-sectional data and analyses, leaving unknown whether and how skin color may affect health over time. Examining the relationship between skin color and repeated measures of health will provide evidence of the extent to which intersecting social factors (such as skin color and gender) have prolonged versus acute consequences on physical well-being. Thus, information from prior research will be augmented here by examining whether skin color differentially shapes average levels of health for African American women and men across an 11-year span.
Fourth, few studies have conceptualized and empirically tested a diverse set of mechanisms that may underlie the skin color–health relationship (see Monk 2015 for an exception). One likely mechanism is socioeconomic characteristics. Previous studies have documented a robust relationship between SES and health in the United States. Those with more socioeconomic resources, including education and income, tend to have better health than their socioeconomically disadvantaged counterparts given their greater access to health-promoting resources, knowledge, and power, and decreased exposure to health risks (Phelan and Link 2015). Studies have also consistently shown that those of lighter skin shades have higher levels of education and income and have partners of higher SES compared with their darker skinned counterparts (Keith and Herring 1991; Monk 2014). Given the plethora of research supporting the notion that interracial differences in SES contribute to racial inequality in health, it is likely that these intraracial variations in SES among African Americans will help explain skin tone disparities in health. Specifically, African Americans with lighter skin may experience better health than those with darker skin as a consequence of their position in the socioeconomic hierarchy and subsequent ability to access health-relevant resources and knowledge.
A second mechanism through which skin tone may shape health among African Americans is exposure to chronic and discrimination-related stressors. Social stressors are linked to poor health via multiple pathways, including advanced deterioration of physiological systems, induction of negative emotional states, unhealthy coping behaviors, and lack of adherence to medical regimens (Seeman et al. 2008; Williams and Mohammed 2009). Institutional and interpersonal discrimination additionally affect health among African Americans by structuring access to opportunities, desired resources, and residence in neighborhoods characterized by concentrated social and economic disadvantages (Gee and Ford 2011; Williams 2012). Exposure to stressors and discrimination may be differentially distributed among African Americans by skin color for several reasons. As a marker of social status, skin color has a major impact on the allocation of socioeconomic resources, with those of darker skin being particularly disadvantaged (Dixon and Telles 2017; Goldsmith et al. 2007; Monk 2014). Therefore, dark-skinned individuals, especially women, tend to have fewer social, economic, and political resources to navigate life compared with their lighter skinned counterparts, resulting in constrained choices for healthy living and increased exposure to stressors.
Furthermore, as a phenotypic attribute, skin color acts as a signal for presumed personal characteristics, including race, competency, and morality (Adams et al. 2016). In a racialized society such as the United States, these presumed characteristics and attitudes toward others are not only a result of systems of oppression, but they are also used to reinforce social structures and hierarchies by shaping practices, relations, and behaviors (Bonilla-Silva 2015). For example, pervasive social stereotypes associate dark brown skin with danger, incompetence, and unattractiveness (Hill 2002b; Maddox and Gray 2002). Given that stereotypes influence behavior automatically and unconsciously (Bargh, Chen, and Burrows 1996), darker skinned individuals are likely to experience worse treatment from society compared with light-skinned individuals. These treatments, such as discrimination, can influence access to life chances. Modest evidence does suggest that darker skinned African Americans, primarily men, report more experiences of discrimination than their lighter skinned counterparts (Hersch 2011; Monk 2015; Uzogara et al. 2014). Other studies, however, have shown no direct link between skin color and reports of discrimination (e.g., Borrell et al. 2006).
The Present Study
Overall, limited research has investigated the relationship between skin color and physical health. Prior studies have generally examined specific markers of health at one point in time, produced mixed findings, overlooked the potential gendered consequences of skin color for health, and not evaluated the extent to which several factors may account for the skin color–health relationship. Addressing these gaps in the literature requires examining global indicators of health across a substantial time period as well as assessing the role of multiple factors that may underlie these associations. The present study therefore investigates the consequences of skin color on average levels of health across an 11-year span, Three research questions are addressed: (1) What is the relationship between skin tone and CBR and self-rated health among African American adults? (2) To what extent are these relationships gendered? (3) Do socioeconomic characteristics, stressors, and experiences of discrimination help explain the skin tone–health relationships?
Data and Methods
Data
This study draws on four waves of panel data from the CARDIA study. The CARDIA study was designed to increase understanding of risk factors for cardiovascular disease during the transition from young adulthood to middle age. It sampled black and white women and men aged 18 to 30 at four field centers in 1985 and 1986: the University of Alabama at Birmingham, the University of Minnesota (Minneapolis, MN), Northwestern University (Chicago, IL), and Kaiser Permanente (Oakland, CA) (n = 5,115). In Birmingham, Minneapolis, and Chicago, participants were recruited by random-digit dialing from total communities or specific census tracts. In Oakland, participants were randomly selected from a membership roster of a health care plan. At each research site, participants were selected so that there would be approximately equal numbers of individuals across gender, age, race, and education subgroups. Follow-up data were collected in 1987–1988 (Year 2), 1990–1991 (Year 5), 1992–1993 (Year 7), 1995–1996 (Year 10), 2000–2001 (Year 15), 2005–2006 (Year 20), and 2010–2011 (Year 25). Analyses are restricted to information from Years 7, 15, 20, and 25. The analytic sample includes respondents who self-identify as African American or black and are not missing on the skin color measure (n = 1,680). Skin tone is the only measure taken from Year 7; all other variables are based on information from Years 15 to 25, when respondents are between the ages of 32 and 55. Response rates among the African American sample across Years 7, 15, 20, and 25 range from 62 percent to 75 percent. 2
Dependent Variables
This study considers two nonspecific measures of physical well-being to assess the broad health consequences of skin color. For both outcomes, women who are pregnant at a particular observation are treated as missing. Cumulative biological risk (CBR) is a summary index of risk factors that reflect physiological dysregulation across multiple systems attributable to cumulative and repeated exposure and adaptation to stressors. Scholars commonly refer to and measure this type of dysregulation with the concept of “allostatic load” (Geronimus et al. 2006). Yet the biomarkers available in the CARDIA study are secondary outcomes (e.g., blood pressure, cholesterol) rather than primary stress mediators that directly characterize allostatic load (e.g., epinephrine, norepinephrine, cortisol). These secondary outcomes may reflect physiological responses to stress or, conversely, may be the result of another etiology. Therefore, similar to other recent studies (e.g., King, Morenoff, and House 2011), the term “CBR” is used instead of “allostatic load” to more accurately describe what is being captured.
Ten biomarkers are used to construct the CBR index. Consistent with prior research, biomarkers are dichotomized based on clinical disease cut points and then summed (King et al. 2011; Seeman et al. 2008). Cutoff points for each biomarker are as follows 3 : systolic blood pressure (1 = ⩾130 mm Hg or high blood pressure medication), diastolic blood pressure (1 = ⩾85 mm Hg or high blood pressure medication), creatinine (1 = ⩾1.2 mg/dL in women and ⩾1.5 mg/dL in men), high-density lipoprotein cholesterol (1 = ⩽49 mg/dL in women and ⩽39 mg/dL in men), total cholesterol (1 = ⩾240 mg/dL or cholesterol medication), triglycerides (1 = ⩾150 mg/dL), waist circumference (1 = >88 cm in women and >120 cm in men), C-reactive protein (1 = ⩾3 mg/L), fasting insulin (1 = ⩾75th percentile of insulin distribution), and fasting glucose (1 = ⩾100 mg/dL or diabetes medication).
Self-rated health is measured by respondents’ answer to the question, “In general, would you say your health is: excellent, very good, good, fair, or poor?” Response categories range from 1 (“excellent”) to 5 (“poor”). Given small cell sizes, the “fair” and “poor” categories are combined (range = 1–4). This single, self-reported item is a reliable and valid measure of general health status. It predicts morbidity (Latham and Peek 2012) and mortality above and beyond known risk factors (Schnittker and Bacak 2014). Importantly, this measure represents an individual and subjective multidimensional conception of health that embodies social, psychological, and biological determinants of health and well-being (Jylhä 2009).
Independent Variables
The main predictor of interest is skin color. Skin color is indexed by three dummy variables: light (yes = 1), medium (yes = 1), and dark (yes = 1). It is measured in Year 7 of the CARDIA study with amber, blue, and green filters of a Photovolt 577 reflectance meter. Values of the meter readings indicate the percentage of light reflected from the upper arm, ranging from 0 percent to 100 percent. Lower values indicate darker skin (less reflectance) and higher values indicate lighter skin (more reflectance). Consistent with previous studies using these data, only amber reflectance readings are used given high collinearity among values of the amber, blue, and green filters (Borrell et al. 2006; Sweet et al. 2007). Values of light reflectance are categorized using the 25th and 75th percentiles of the amber filter distribution among African Americans (range = 7.1–51.2). Respondents with values greater than the 75th percentile are considered “light,” respondents with values between the 25th and 75th percentiles are considered “medium,” and respondents with values lower than the 25th percentile are considered “dark.” Light-skinned African Americans serve as the reference group. The categorization of the skin tone measure as well as these specific cut points are used in attempts to clearly discern independent skin tone groups and accurately capture how individuals may be viewed in the social world, particularly at the extreme ends of the skin color spectrum. Supplemental analyses (available on request), however, indicate that findings are robust to alternative measures of skin color.
Education, income, and marital status are used to examine the extent to which socioeconomic characteristics explain the relationship between skin tone and health. In an effort to use all available information from the CARDIA study, these measures are treated as time-varying covariates. Education is indexed by three dummy variables: whether the respondent has a high school education or less (yes = 1; reference group), has more than a high school education or some college education (yes = 1), or has a college education or more (yes = 1). Respondents’ combined family income is assessed with an ordinal variable that is treated as continuous: 1 = less than $5,000, 2 = $5,000 to $11,999, 3 = $12,000 to $15,999, 4 = $16,000 to $24,999, 5 = $25,000 to $34,999, 6 = $35,000 to $49,999, 7 = $50,000 to $74,999, and 8 = $75,000 or higher. Marital status is measured with a binary variable (1 = married or living with someone in a marriage-like relationship).
Stress and discrimination are additional explanatory variables of interest. In Years 15, 20, and 25, participants are asked about chronic burdens (lasting for >6 months) in four domains of life: health of close others, work, finances, and relationships. Response categories are recoded to 0 = “no”; 1 = “yes, but not very stressful”; 2 = “yes, moderately stressful”; and 3 = “yes, very stressful” and averaged across the four domains (range = 0–3). In years 15 and 25, participants are also asked whether they have experienced discrimination, been prevented from doing something, or been hassled or made to feel inferior in any of the following situations because of their race or color: at school, getting a job, purchasing a home, at work, at home, getting medical care, or on the street or in a public setting. Respondents indicate how often they experienced each situation: 0 = “never,” 1 = “rarely,” 2 = “sometimes,” or 3 = “often.” I average across these seven experiences to create a measure of racial/color discrimination (range = 0–3). Because discrimination is not measured in Year 20, I impute values for this year by averaging discrimination scores from Years 15 and 25, specific to each skin color-gender group. Supplemental analyses (available upon request) indicate that results are robust to varying approaches to imputation. Stressors and discrimination are treated as time-varying covariates and are centered at their means for ease of interpretation.
All models control for age, measured in years and centered at age 32, and whether the respondent has had health insurance for at least 18 months within the past two years (1 = yes). Additionally, taking medication for a health issue (1 = yes) is included in all self-rated health models. Medication use is not only a marker of poor health—of which those of marginalized social statuses (e.g., dark-skinned African Americans, women, those of lower SES) are more likely to suffer—but it represents a particular awareness of a health problem. Such recognition may be relevant when evaluating one’s own health. Medication use is already accounted for in the CBR measure and is therefore not included as a control in the CBR models.
Given theoretical arguments that the consequences of skin color are gendered, models are stratified by gender (0 = men, 1 = women). Chow tests are used to assess whether the magnitudes of coefficients for skin color, socioeconomic characteristics, stressors, and discrimination statistically differ for women and men. To minimize selection biases arising from attrition due to dropout across study waves, I control for the proportion of waves a respondent was not interviewed. This method is consistent with other studies using panel data and similar analytic methods (e.g., Brown et al. 2016).
Analytic Strategy
Random-intercept multilevel models estimated within a mixed-model framework are used to examine the relationship between skin color and average levels of health across ages 32 to 55. These models are ideal for panel data because they adjust for nonindependence of observations due to repeated measures of the same individual across multiple waves (Raudenbush and Bryk 2002). Given the sampling design of the CARDIA study, responses may also correlate among clusters. For ease of interpretation, a linear specification for each outcome is presented, though supplementary analyses suggest that results are robust to a Poisson specification for CBR and an ordinal specification for self-rated health (see online Appendix Tables 1 and 2, respectively). Both fixed effects of covariates and random effects for the intercept are included in each model. Estimating random effects for the intercept accounts for person-specific errors, which represent unobserved differences between individuals that are stable over time and not accounted for by the covariates. Among the random effects, repeated observations (Level 1) are nested within respondents (Level 2). A comparison of likelihood ratio tests indicates that including a quadratic term for age did not improve the overall fit for the CBR and self-rated health models. Therefore, only a linear term for age is considered.
Means and Proportions of Study Variables at Baseline, by Skin Color and Gender.
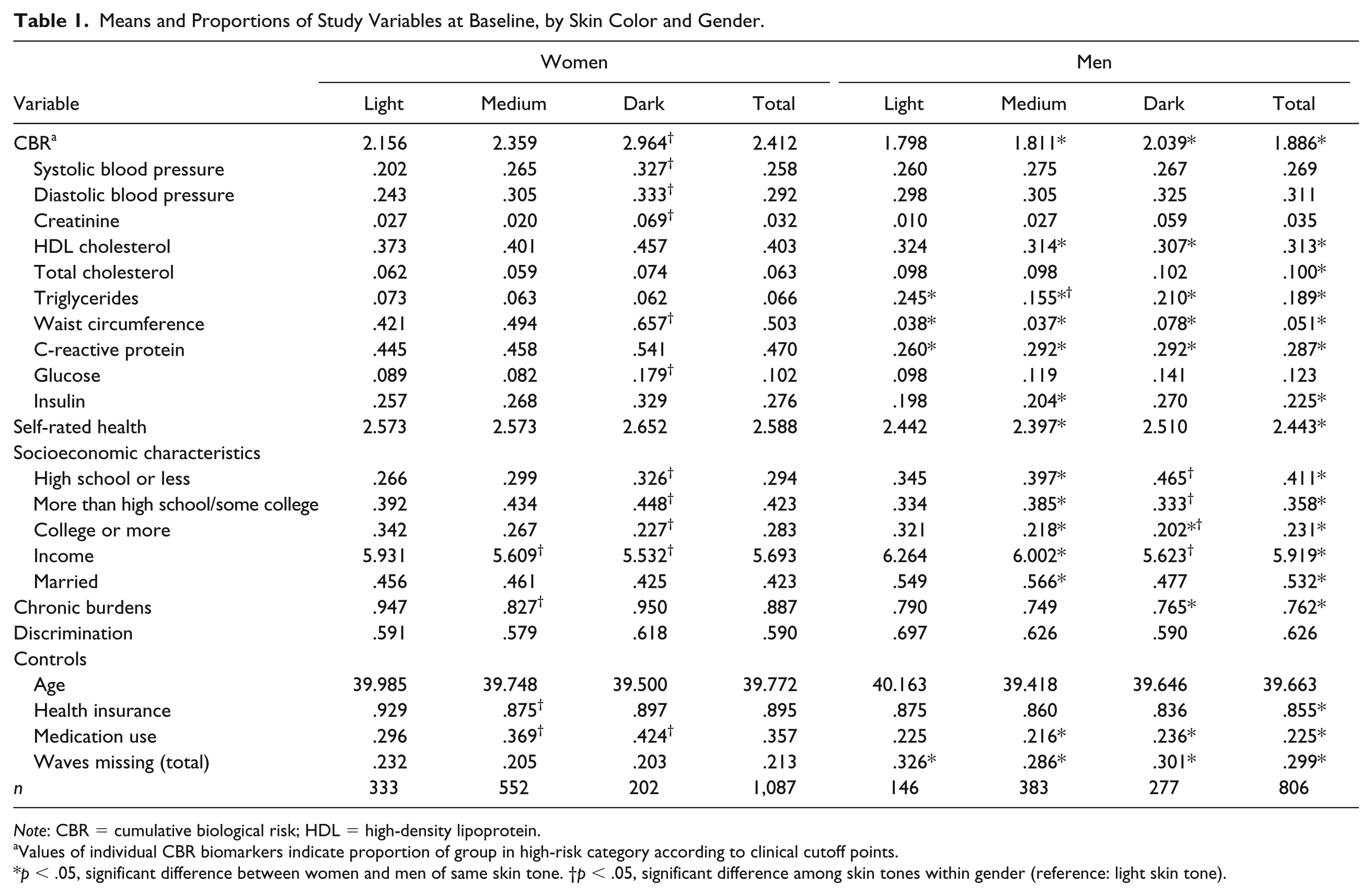
Note: CBR = cumulative biological risk; HDL = high-density lipoprotein.
Values of individual CBR biomarkers indicate proportion of group in high-risk category according to clinical cutoff points.
p < .05, significant difference between women and men of same skin tone. †p < .05, significant difference among skin tones within gender (reference: light skin tone).
Multilevel Models of Skin Color, Socioeconomic Characteristics, Chronic Burdens, Discrimination, and Cumulative Biological Risk.
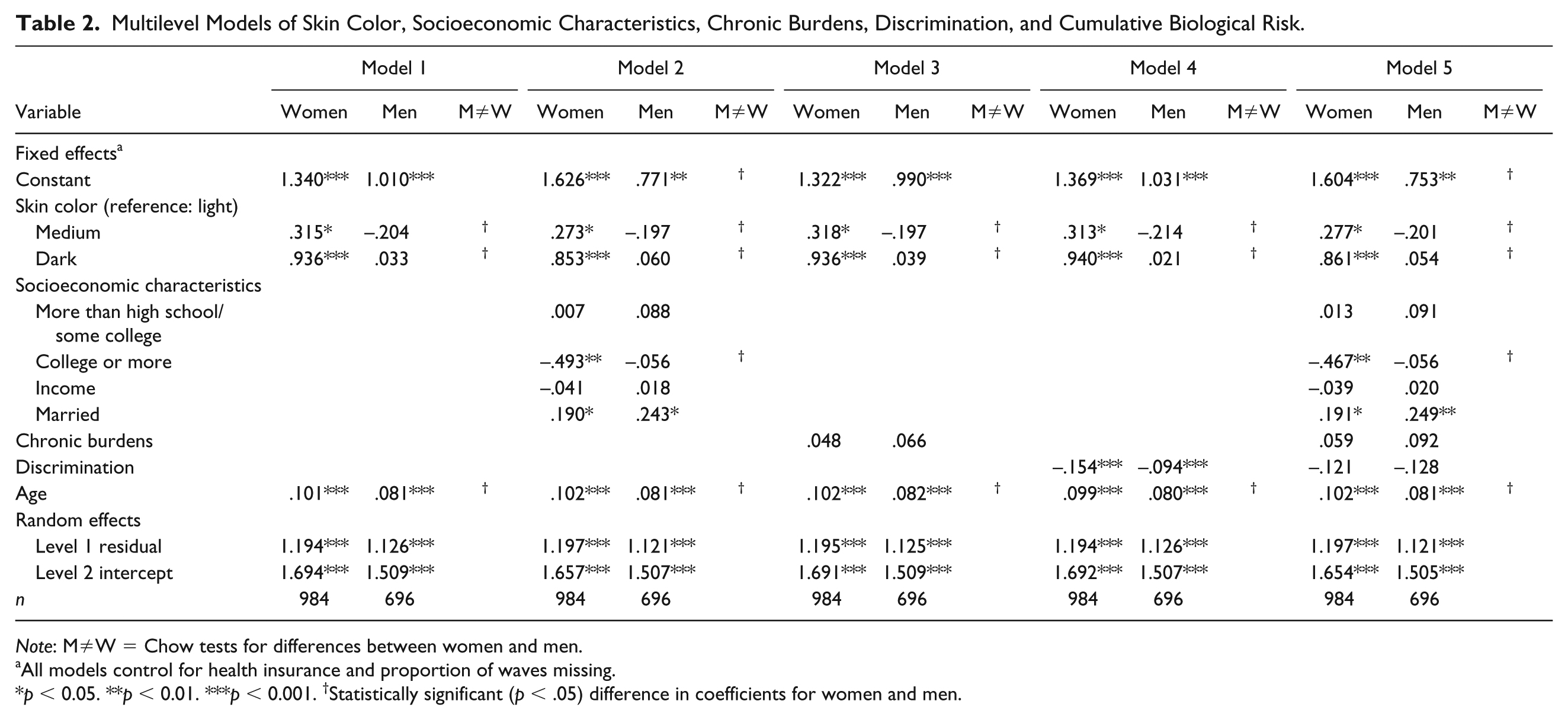
Note: M≠W = Chow tests for differences between women and men.
All models control for health insurance and proportion of waves missing.
p < 0.05. **p < 0.01. ***p < 0.001. †Statistically significant (p < .05) difference in coefficients for women and men.
Table 1 presents the means and proportions of all study variables by skin tone and gender at Year 15. Tables 2 and 3 present multilevel models that estimate the extent to which skin color, socioeconomic characteristics, stressors, and discrimination shape CBR and self-rated health, respectively, among African American women and men. A stepwise modeling approach is used wherein each proposed explanatory factor is considered independently then collectively in the final model. Specifically, Model 1 in Tables 2 and 3 regresses the health measures onto skin color, net of control variables. Models 2, 3, and 4 individually add socioeconomic characteristics, stressors, and discrimination measures, respectively, to Model 1. Model 5 of each table includes all covariates. Analyses are performed in Stata 14.1, and multiple imputation is used to handle item missingness.
Multilevel Models of Skin Color, Socioeconomic Characteristics, Chronic Burdens, Discrimination, and Self-rated Health.
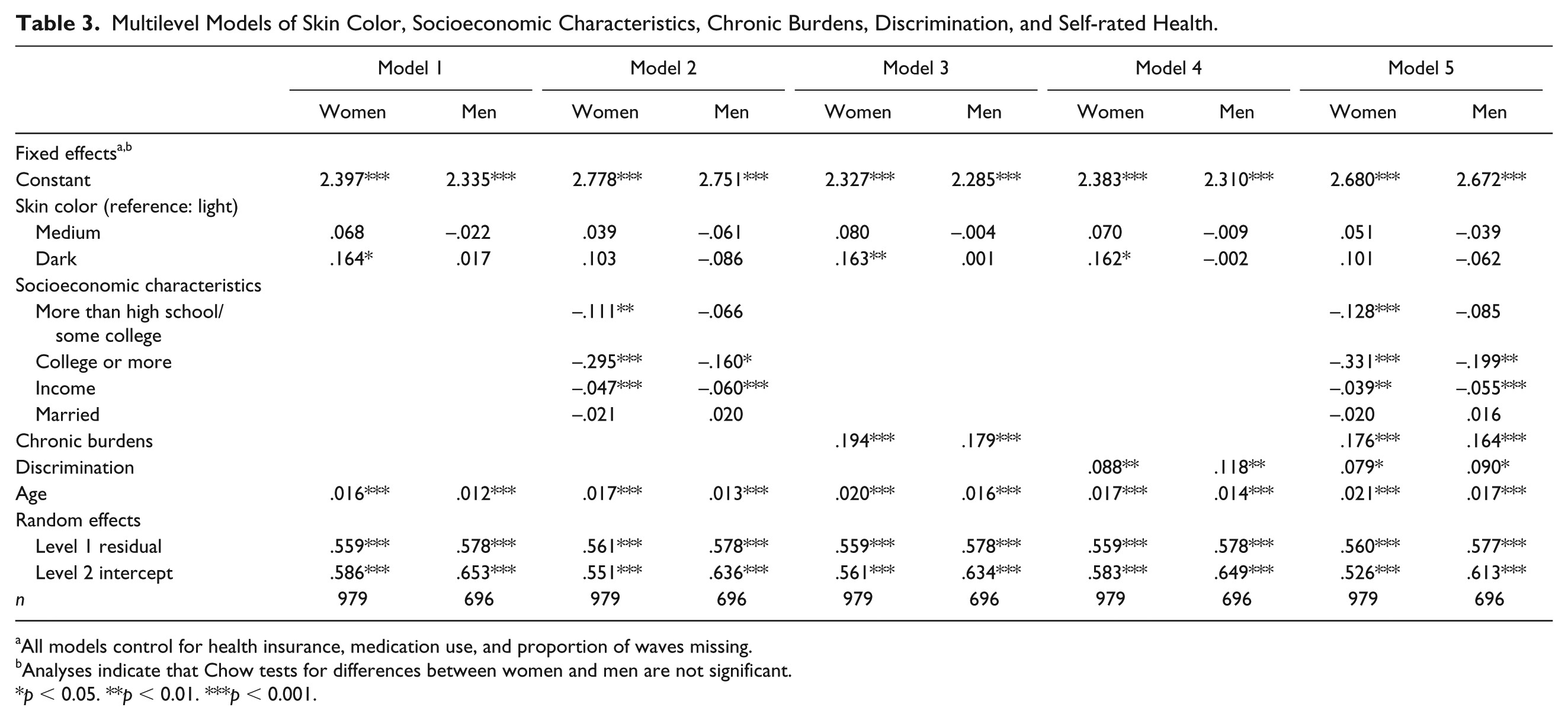
All models control for health insurance, medication use, and proportion of waves missing.
Analyses indicate that Chow tests for differences between women and men are not significant.
p < 0.05. **p < 0.01. ***p < 0.001.
Results
The results in Table 1 indicate that several of the study measures vary by skin color and gender. For example, African American women tend to have a higher CBR score and self-report worse health than men. Gender differences are especially pronounced for high-density lipoprotein and total cholesterol, triglycerides, waist circumference, C-reactive protein, and insulin. Additionally, levels of education, chronic burdens, health insurance, and medication use tend to be higher among women, while levels of income and marriage are higher among men.
There is also a skin color gradient in health and SES among women. Compared with those of light brown skin, dark-skinned women have a higher CBR score, are less likely to have a college education, have less income, and are more likely to be taking medications. Interestingly, light- and dark-skinned women report similar levels of chronic burdens and have similar rates of health insurance, both of which are higher than those of medium-skinned women. Among men, there is a similar skin color gradient in socioeconomic resources whereby dark-skinned men have lower levels of education and income than light-skinned men.
CBR
The results of Model 1 in Table 2 suggest that there are significant skin color disparities in CBR among African American women only. There are no significant skin color differences among men. Compared with women with light skin, medium- and dark-skinned women have higher average CBR scores across adulthood. For example, among women aged 45, those measured as having light brown skin have a predicted CBR score of 2.55, while those measured as having medium or dark brown skin have predicted CBR scores of 2.87 and 3.49, respectively. Ancillary analyses (available on request) suggest that no individual biomarker is driving the results among women or men. Moreover, the significant Chow test for the age slopes across all models suggests that CBR increases with age at a faster rate for African American women than men.
Model 2 adds socioeconomic characteristics to Model 1. The results suggest that education and marital status are associated with CBR scores among women and explain a small portion of the skin color disparity between light-skinned women and their medium- and dark-skinned counterparts. Among men, marital status has a direct, positive relationship with CBR. Results from Models 3 and 4 suggest that neither chronic burdens nor racial or color discrimination explains the skin color disparities among women. Additionally, these stressors do not have a direct effect on CBR for women or men. When considered collectively (Model 5), education and marital status continue to predict CBR among women and account for a small portion of the skin color disparities. Being married remains positively associated with CBR among men.
In each model in Table 2, the coefficients for medium and dark skin among women remain statistically significant, indicating that socioeconomic characteristics, stressors, and discrimination do not explain skin tone differences in physiological markers of health. However, the unequal distribution of education and marital status explains about 12 percent of the medium-light disparity in CBR among women and about 8 percent of the dark-light disparity. Furthermore, the significant Chow test for the intercept and skin color coefficients in Model 5 indicates that dark-skinned women have the highest CBR of all skin color-gender groups, followed by medium-skinned women, light-skinned women, and African American men.
Self-rated Health
Table 3 displays results from multilevel models examining the associations among skin color, socioeconomic characteristics, stressors, discrimination, and self-rated health. Model 1 of Table 3 indicates that dark-skinned women tend to report worse health than light-skinned women. Among average-aged women, for example, those with a light brown skin complexion have a predicted health rating of 2.64, while those with a dark brown skin complexion have a predicted rating of 2.81. There are no initial skin color differences in self-ratings of health among men. Model 2 of Table 3 suggests that higher levels of education and income are related to better self-ratings of health for both women and men. Additionally, the coefficient for dark skin among women in Model 2 is reduced in magnitude (by approximately 37 percent) and to statistical nonsignificance at the .05 α level, suggesting that skin color differences in education and income explain the dark-light gap in self-rated health among women.
Models 3 and 4 suggest that chronic burdens and discrimination each similarly predict worse self-reports of health among women and men. The coefficient for dark skin among women reduces in magnitude but remains statistically significant in these models, indicating that chronic burdens and discrimination slightly contribute to the self-rated health disadvantage among dark-skinned women. When considered collectively (Model 5), education, income, chronic burdens, and discrimination continue to influence self-rated health among women and reduce the coefficient for dark skin in magnitude and statistical significance. Among men, the associations among education, income, chronic burdens, discrimination, and self-rated health remain significant.
Discussion
Racial inequalities in physical health remain a significant issue in the United States. Black-white health disparities have not abated and cannot be completely accounted for by socioeconomic and psychosocial factors (Brown et al. 2016; Hargrove 2018; Sternthal et al. 2011). Examining intragroup heterogeneity in health among African Americans, however, may provide critical insight into the mechanisms underlying disparate rates of poor health among African Americans. Specifically, within-group approaches identify factors that distinguish pathways to health among those similarly positioned in the social structure. These types of approaches highlight the possibility that the impact of social determinants of health are not equivalent across racial groups (Whitfield et al. 2008), and that the experiences and consequences of race may be shaped by other social statuses (Collins 2015).
An important source of intragroup heterogeneity among African Americans is skin color. Scholarship has documented the distinct influences of skin color on life chances above and beyond the consequences of traditionally measured self-identified race (Goldsmith et al. 2007; Wade et al. 2004). To date, however, few studies have systematically investigated the relationship between skin tone and physical health among African Americans, particularly how these relationships may be gendered and influenced by social factors other than SES (for an exception, see Monk 2015). The present study addresses these gaps of prior research and contributes to our understanding of skin color stratification in health in several important ways.
First, this study is among the first to examine the extent to which skin tone differentially shapes global measures of health for African American women and men. This study examined measures of health that go beyond what has typically been considered in past research of skin color and health, and highlights the cumulative and simultaneous consequences of several dimensions of stratification. For example, the findings suggested that skin color was a significant predictor of cumulative biological risk (CBR) and self-rated health among African American women only. Medium- and dark-skinned women tended to experience more physiological deterioration than their light-skinned counterparts, while dark-skinned women also self-reported worse health. Medium- and light-skinned women, however, self-reported comparable levels of health. Given that CBR and self-rated health represent multiple aspects of overall health, the results suggest that skin color exerts a broad impact on the physical well-being of African American women across early adulthood and midlife.
The results of this study provide evidence that the association between skin color and physical health is gendered. These findings are consistent with prior literature indicating that skin color is particularly salient in the lives of African American women compared with men (Hunter 2007; Keith and Herring 1991). The health disadvantages of women with dark brown skin found here, as well as the lack of significant influence of skin color for men’s health, may be a result of the intersecting consequences of colorism and sexism. For example, scholars have noted the particular importance of beauty for the life chances of all women in patriarchal societies (Hamermesh 2013). Hegemonic and Eurocentric constructions of beauty, which tend to privilege white, middle-class women (Jeffreys 2014), teach girls from an early age that their bodies will be evaluated on the basis of their appearance and that beauty is an attribute that must be pursued by women (Franzoi 1995). In turn, aesthetics confer social, economic, and political advantages for women deemed socially attractive in the ways that other characteristics (e.g., intelligence) afford advantages to men (Anderson et al. 2010; Fletcher 2009; Lakoff and Scherr 1984).
For African American women specifically, fair skin, which is a Eurocentric characteristic of beauty, embodies a form of capital that can be translated into health-relevant resources (Hamilton et al. 2009; Hunter 2007). African American men and darker skinned women do not have access to this type of capital. Indeed, results from both prior literature and the present study suggest that lighter skin is associated with several health protective factors among African American women only, including higher levels of education, occupational status, family income, high-status marriages, and self-esteem, as well as fewer chronic burdens (Hunter 2005; Keith and Herring 1991; Thompson and Keith 2001). Taken together, these findings suggest that skin color structures access to resources and exposures to health risks relevant for the physical well-being of black women in ways that it does not for black men.
Second, this study extends previous research by examining several factors that may underlie skin color disparities in health. The majority of past research has tended to focus on socioeconomic explanations for the association between skin color and health. The present study, however, examined the influence of chronic burdens and racial/color discrimination in addition to socioeconomic characteristics. The findings indicated that the proposed mechanisms did little to account for skin color inequalities in CBR among women. Furthermore, stress and discrimination did not directly shape physiological functioning for either women or men. This is surprising given that the CBR index reflects, in part, physiological responses to stress. However, extant studies have similarly found that reports of perceived racial discrimination, in particular, are not directly related to physiological markers of health among African Americans (Chae et al. 2010; Fuller-Rowell, Doan, and Eccles 2012; Roberts et al. 2008). Although scholars propose various explanations for these nonsignificant relationships (e.g., internalized racism, acknowledgment of discrimination as a protective mechanism), future research is needed to test such hypotheses and others as they relate to linkages among stressors, discrimination, and health.
Another possible explanation for the inability of discrimination to predict CBR is the construction of the discrimination measure. The current measure averaged across multiple sites of discrimination, implicitly assuming that each discriminatory event was equally consequential for health. Recent research, however, suggests that African Americans of varying skin shades are exposed to not only different amounts of discriminatory experiences but also different types (Keith et al. 2017). The approach used in the present study to capture discrimination may be obscuring unique patterns and domains in which skin tone might be more germane. Although examining this possibility is beyond the scope of this study, future work should consider whether and how specific types of discrimination differentially shape health among African Americans of various skin tones.
For self-rated health, several of the proposed explanatory factors helped reduce the dark-light disparity among women in both magnitude and statistical significance, namely socioeconomic characteristics. Education and income accounted for the majority of the impact of skin color on self-ratings of health among women. These findings suggest that disparities in self-rated health stem, in part, from the economic disadvantages of dark-skinned women compared with their lighter skinned counterparts. It is likely that increased access to education and income affords light-skinned women the intrinsic and instrumental resources to promote health knowledge and behaviors, reduce exposure to health risks, and possibly ameliorate the consequences of disease after its onset, all of which would contribute to one’s perceptions of their health (Herd, Goesling, and House 2007; Phelan and Link 2015).
Overall, although the findings indicated that socioeconomic characteristics explained the dark-light disparity in subjective ratings of health, chronic burdens and perceived discrimination did little to account for the health disadvantages of darker skinned women compared with light-skinned women. The limited utility of the proposed factors for explaining skin color differences in health—particularly objective measures of health—suggests a need to evaluate whether other structural and psychosocial factors mediate the skin tone–health relationship. One potential line of inquiry involves examining experiences of unfair treatment specific to one’s skin color. Although prior work generally indicates that darker skinned African Americans report more experiences with discrimination (Hersch 2011; Maddox and Gray 2002), additional scholarship suggests that those with light skin may experience considerable unfair treatment from other African Americans because they are less readily perceived as members of the black community (Cunningham 1997; Uzogara and Jackson 2016; Veenstra 2011). Social cues and treatments by others that do not confirm personal identities and act to exclude individuals from the communities with which they identify can induce stress or jeopardize several determinants of health, such as self-esteem or other psychosocial resources (Campbell and Troyer 2007).
Recent work provides evidence for such a possibility, documenting that discrimination from other African Americans on the basis of skin color is disproportionately experienced by those of dark- and light-skin complexion (Monk 2015; Uzogara and Jackson 2016; Uzogara et al. 2014). Although skin color discrimination from varying sources is likely a crucial pathway linking skin tone to health, questions regarding unfair treatment in many data sets tend to confound or equate consequences stemming from race and color. This limits researchers’ ability to disentangle the influences of race and color on life chances. The data used in the present study, for example, do not capture social experiences and interactions attributable specifically to skin color, nor do they collect information on the race of the person committing the discriminatory act. Future data collection efforts should be geared toward obtaining more specific information on individuals’ unique experiences with discrimination.
This study is not without limitations. First, although geographically diverse areas were sampled, the CARDIA data are not nationally representative, and findings cannot be unequivocally applied to the broader U.S. population. It is important to note, however, that prior analyses indicated that the health statuses of CARDIA respondents at baseline were similar to those of black and white participants in national data sets collected around the same time (Friedman et al. 1988). Thus, it is unlikely that the findings here do not apply in any way to the broader African American population. Relatedly, the data may be subject to potential selection bias given the disproportionate experience of socioeconomic disadvantage and incarceration among blacks compared with whites and dark-skinned blacks compared with their lighter skinned counterparts (Western and Pettit 2010; White 2015). This type of selection bias, however, would likely produce conservative estimates of skin color disparities in physical health. Indeed, those who have the worst health (i.e., the socioeconomically disadvantaged) or are exposed to the most severe stressors (i.e., incarcerated populations), both of whom are more likely to be darker in skin complexion, are less likely to be included in the CARDIA study.
Second, this study is unable to examine whether skin color shapes health among a diverse set of racial/ethnic groups, as the majority of information available in the CARDIA study is for non-Hispanic white and black adults. Similarly, because of data limitations, the extent to which the skin tone–health relationship varies by ethnicity and nativity among Black Americans remains unclear. Prior research documents a health disadvantage among U.S.-born African Americans compared with their U.S.- and foreign-born counterparts of African or West Indian ancestry (Jasso et al. 2004; Read and Emerson 2005). Variations in historical and contemporary understandings of, and interactions with, racialized social structures may further differentiate the skin color-health relationship by ethnicity and nativity among the Black American population (e.g., Read and Emerson 2005).
Third, skin color is measured objectively, as the percentage of light reflected off of respondents’ skin. This type of measurement lacks the subjectivity and complexity characteristic of self-identification and social appraisals of others (Bargh et al. 1996; Strack and Deutsch 2004). Furthermore, recent work suggests that self-assigned and socially assigned skin color have distinct impacts on health status and determinants of health among African Americans (Monk 2015). Self-assigned and socially assigned measures of skin color likely represent different aspects of social categorization processes that occur at various levels of society. Interviewer-rated skin color, for example, might better capture the consequences of macro-level systems of power and domination that position individuals and groups in the social hierarchy (Bonilla-Silva 2015).
Self-rated skin tone, however, represents individuals’ assessments of their relative placement in the social structure. This type of self-identification is argued to be shaped by dynamic lived experiences and relationships with others, and to represent the culmination of interactions with the social world across the life course (Monk 2015). Given that different measures of skin color embody unique features of stratification processes, they likely have varying relationships with health. Although multiple measures of skin color should be evaluated in the context of health inequality, objective measures of skin shade are still important, and at times preferable, indicators of skin color. Objective measurements, for example, allow for comparability across studies and populations, and reduce biases and use of nonrelevant information inherent in interviewer ratings of skin color (Branigan et al. 2013; Hill 2002a).
Despite these limitations, the present study provides new evidence of skin color stratification in physical health among African American women. These findings augment prior research that documents skin tone biases and the gendered nature of colorism in the United States. The within-group approach used here aids in identifying specific groups that may be overlooked in studies relying solely on between-group analyses. These groups may be key to helping explain health disparities between and within social groups that are often assumed to have monolithic experiences. Policies directed toward eradicating health inequality should be attentive to the unique mechanisms underlying health among social groups, as these varied pathways reflect, in part, the differential consequences of simultaneously experienced social statuses.
Supplemental Material
Appendices_TH_SRE_17-0129 – Supplemental material for Light Privilege? Skin Tone Stratification in Health among African Americans
Supplemental material, Appendices_TH_SRE_17-0129 for Light Privilege? Skin Tone Stratification in Health among African Americans by Taylor W. Hargrove in Sociology of Race and Ethnicity
Footnotes
Acknowledgements
I would like to thank Tyson Brown, André Christie-Mizell, Dan Cornfield, and Hedy Lee for their continual support and guidance as well as Erika Leslie and Bob Hummer for their helpful comments.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.