
Abstract
This hermeneutic phenomenological study explored the meaning of post-operative pain for patients following day case shoulder surgery. Eighteen adults with a confirmed diagnosis of shoulder injury who were scheduled for day surgery were recruited purposively. Unstructured interviews were conducted by phone or online, audio recorded, transcribed verbatim, and analyzed using Diekelmann’s interpretative method. Four constitutive patterns were developed: (1) Suffering perpetually in pain; (2) Overcoming pain; (3) Living in an unfamiliar body; and (4) Communicating and Lacking Essential Information. Pain was often unexpected, unpredictable and disruptive; the body was experienced as “unhomelike” due to temporary dysfunction of the affected limb and enforced dependence on others for daily help. Pain medication regimes and goals were not always understood, nor used as prescribed, though some participants were able to accept and withstand their temporary post-operative pain. Information from healthcare providers was perceived to be of poor quality, causing confusion during the post-operative period. The experience of shoulder pain following day surgery is complex, and one for which most participants were unprepared, suggesting a need for a nursing approach toward pre-operative preparation and post-operative rehabilitation – acknowledging patients’ relevant prior experiences, providing clear, concise information, creating pre-operative “shoulder” clubs and facilitating consistent follow-up which is not currently catered for by the current day case model.
Introduction
Day case surgery – where the patient is admitted, treated and discharged from hospital within 23 hr – is increasingly prevalent across healthcare systems seeking to enhance efficiencies and improve patient experiences (Bailey et al., 2019). The number of day case surgeries performed in the UK has increased from 35% in 2013/14 to 66% in 2019; best available recent evidence indicates that 83.9% of surgery procedures within England are being undertaken as day cases (Appleby, 2015; NHS England, 2024; NHS England Digital, 2019), comparable with day case surgery rates in the USA (75%–80%) and Scandinavia (85%–90%; American Hospital Association [AHA], 2020; Kreutzberg et al., 2024). Many conditions requiring surgery, including shoulder injuries, can now be effectively managed as a day case when there is no other compelling reason for routine admission. However, there is robust evidence reporting the extent of post-operative pain, and that such pain is often poorly managed in people discharged following day case surgery (Rasmussen et al., 2018).
Patients’ needs for analgesia after day case shoulder surgery reflect those following in-patient shoulder surgery, with a third of patients reporting severe pain on the first post-operative day (Cho et al., 2011; McGrath et al., 2004). Although the incidence of post-operative shoulder pain varies depending on the type of surgery performed, patient population and surgical technique, surgical trauma and tissue manipulation during the procedure can lead to acute post-operative pain; inflammation and tissue edema contribute to pain and discomfort in the early post-operative period, and nerve injury during surgery can result in neuropathic pain or alter sensation in the shoulder. The techniques adopted by both the surgeon and anesthetist, and patient factors such as age, gender, and level of anxiety or uneasiness may also impact on the severity of post-operative shoulder pain (Cuff et al., 2016; Dekker et al., 2016; Menendez et al., 2018).
Suboptimal management of pain after day case shoulder surgery may adversely influence patient outcomes due to delayed post-operative rehabilitation or exercises (Lanna et al., 2012), the potential risk of the development of chronic pain (VanDenKerkhof et al., 2012) and consistent use of opioids that can lead to dependency (Buys et al., 2020). The clinical understanding of post-operative shoulder pain is well-understood from a medical and primarily quantitative perspective, but impact on the patient suffering pain is minimally described. What evidence there is indicates difficulties with basic function of activities of daily living including dressing, showering and cooking (Kolade et al., 2023). Pain impacts restful sleep, further exaggerating discomfort and disrupting involvement in domestic and occupational activities and, in some circumstances, may lead to self-isolation (Karayannis et al., 2019). Further understanding is essential, as prolonged and incapacitating shoulder pain can lead to profound physical, psychosocial and economic consequences (Harding et al., 2005). There is limited qualitative research reporting the impact of post-operative shoulder pain (Lyne et al., 2022; Minns Lowe et al., 2014) but none exploring the meaning of post-operative shoulder pain, following discharge from day case surgery. These terms differ considerably – impact refers to the effect and consequences of an event and in respect of shoulder pain, is typically understood in physiological and measurable terms: increased pain reduces mobility and disrupts sleep. In contrast, meaning refers to the personal understanding and interpretation of an event, and is usually understood and reported in emotive terms, for instance “the pain was so bad I couldn’t do anything for myself, I felt like I was useless.” By exploring meaning from a qualitative perspective, we can gain insight into the contextual everyday consequences of post-surgery pain and draw on those insights to propose strategies for better preparation of future patients for surgery, and recovery. Understanding the impact of post-operative shoulder pain on an individual, and the psychosocial influences that inform the experience of pain can help raise nurses’ awareness of pain after surgery and at rehabilitation, thus facilitating better experiences, setting realistic expectations, and improving outcomes for patients.
This nurse-led qualitative study explored how patients who had undergone day-case shoulder surgery constructed meaning from the experience of pain following discharge, and how their expectations and experiences informed this meaning. By understanding these concerns, new evidence pointing toward the need for better pre- and post-operative nursing intervention, particularly in respect of providing information, setting expectations, and promoting appropriate use of prescribed analgesics has been added to the qualitative literature.
Research Question and Objectives
For this study we asked: What is the meaning of the experience of pain following shoulder operations after the patient is discharged home from day-case surgery? The objectives were to:
understand the meaning of the experiences of shoulder pain following discharge from day surgery
illuminate underlying themes and contexts that may account for these experiences
Methods
Underpinning Philosophy
Heidegger’s philosophy holds that human experience is always experienced in the world (being-in-the-world); it is through our interactions with the world we inhabit, that we make sense of our ongoing experiences. Our being-in-the-world (our “Dasein”) is itself hermeneutic – it is informed by all we have experienced before, the culture we belong to, the history we carry with us; in this way our past informs our future, and thus Heidegger acknowledged Dasein’s temporal existential time as “being ahead of itself” (Heidegger, 1962, pp. 236–237). We therefore make sense of and understand our future experiences because of past experiences we have already had. In the context of pain, a previous anxiety-provoking experience of pain may well influence an individual to anticipate any future experience of pain to be as anxiety-provoking, or perhaps more so. Understanding the meaning of experience therefore requires adoption of a methodology that embraces and engages with the context of those experiences.
Study Design
This qualitative study used a hermeneutic phenomenological methodology (Benner, 1994; Dibley et al., 2020; Ironside, 2006) informed by Heidegger’s (1962) philosophy of interpretive phenomenology.
Participants, Sampling and Sample Size
Participants were recruited from one major London Hospital NHS Trust between April 2021 and September 2021. A study information pack was provided by the first author to patients attending pre-assessment appointments who were due to undergo orthopedic shoulder operations, such as shoulder arthroscopy, shoulder stabilization, rotator cuff repair, correction of shoulder dislocation or instability, acromioclavicular (AC) repair, frozen shoulder and arthroscopic Bankart procedure. These procedures are undertaken regularly at the day surgery unit where this research was carried out.
Participants were eligible if they were at least 18 years old, with a confirmed diagnosis of a shoulder injury requiring surgery and already booked for day case shoulder surgery. The only exclusion criteria were being booked for inpatient surgery, or incapacity to give informed consent. In hermeneutic phenomenology, the world in which an experience occurs (and therefore all cultural, historical, past and present influences) adds context to the present experience; these contextual influences are thus embraced within the research (Neubauer et al., 2019). For example, if someone who needed shoulder surgery also had a diagnosis of diabetes and lived alone, this would add to the meaning of the post-operative shoulder pain experience, which could affect the ability to self-manage the diabetes and carry out other self-care activities. To ignore context would objectify experience, and limit hermeneutic understanding (H. G. Gadamer, 2006).
Purposive sampling was used to ensure the involvement of study participants who were likely to be able to address the research aims and provide data to answer the research question. The quest for rich, contextual data leads to small sample sizes; the aim is to search for individual meanings and similarities of experience of the phenomenon under investigation, rather than prove or disprove any hypothesis. Malterud et al. (2016) propose the concept of “Information power” to guide the size of the sample in qualitative study: the more information the sample holds that is relevant to the study, the lower the number of participants needed. Research studies using hermeneutic phenomenology typically have sample sizes of 10 to 20; for example, Stayt et al. (2015) interviewed 17 patients to explore their experiences of technology in an adult intensive care unit, Firouzkouhi et al. (2022) interviewed 16 patients about their experiences with Covid 19, while K. Clancy (2007) explored the experience of 10 patients living with long-term oxygen therapy. This study recruited 18 participants.
Ethical Considerations
Ethics approval was given by the National Research Ethics Committee in England (Ref:14/SC/1121); research governance was provided by the steering group with oversight of the day case unit at the university teaching hospital research site in London, UK. Written informed consent was secured prior to collection of any data, and participants were fully informed of their right to withdraw from the study at any time without affecting their care and treatment, and that their research and personal data would be managed in accordance with the UK Government’s General Data Protection Act (UK Government, 2018).
Researcher Positionality
At the time of the study, the first author (IM) was a PhD student, and Matron for the day surgery theater and ward at a major hospital in London, England. He had also undergone shoulder surgery for shoulder stabilization following an accident, and 3 years before starting the study and had experience of post-operative shoulder pain after day surgery. These two experiences positioned him with a sound professional and personal connection with the topic of interest; his professional role meant he was well-placed to consider how findings from the study might lead to improvements in practice in the clinical setting. The remaining authors were academic PhD supervisors with clinical or research experience in trauma and orthopedic nursing (TF), chronic and acute pain (TT) and adult (general) and pediatric nursing (LD). The senior author (LD) is also a methodological expert in hermeneutic phenomenology.
Data Collection
In keeping with the philosophical underpinnings, unstructured interviews in hermeneutic phenomenology are usually conducted face-to-face to reflect the philosophical and contextual importance of “being-with” (Mitsein) and “being-in-the-world” (Dasein); however, the COVID-19 pandemic necessitated online data collection due to mandatory social distancing, and ethical issues around patient and researcher safety. Participants were interviewed over the telephone or via video-conferencing, according to their preference. Data collection methods that “give voice to” participants are philosophically and methodologically appropriate in hermeneutic phenomenology, since language is fundamental to human expression of experience (Dibley et al., 2020; Heidegger, 1971; McManus Holroyd, 2007); the researcher also brings their own being-in-the-world knowledge to co-construct with the participants, through language, a new shared horizon of understanding (Crowther et al., 2017; Dibley et al., 2020; Ironside, 2003).
Participants were interviewed during the immediate post-operative period, typically within 2 weeks of surgery. Unstructured interviews lasting 15 to 60 min were conducted by the first author between April and September 2021, with only the participant and researcher present. Participants were invited to “Tell me about your experiences of pain following your discharge after shoulder surgery.” Prompts, such as “How did you feel when X happened?” and “Can you tell me more about X?” were used as appropriate. An iterative approach was used for the interviews, meaning that the use of prompts in each interview helped guide the questioning for interviews of subsequent participants and enabled identification of emergent themes later. Interviews were audio-recorded and transcribed verbatim.
Data Analysis
The method described by Diekelmann et al. (1989) was adapted and applied to analyze data [Table 1]. The goal of the method is to enable development of constitutive patterns (shared meanings across all transcripts) and relational themes (present in some transcripts). Repeated engagement generates familiarity with the data set and develops a holistic sense – the “gestalt” (Flick, 2009) – across the data. Diekelmann’s method reflects Heidegger’s philosophy by creating hermeneutic cycles of understanding which bring significant matters to readers’ attention (Smythe et al., 2008).
The Seven Stages of the Hermeneutic Analysis Method, Based on Diekelmann et al. (1989).

The method was amended from the original which, in Stage 7, advised sending transcripts back to participants for an assurance of “accuracy.” This common qualitative method of “member-checking” was avoided, since methodological developments in the last two decades have moved toward challenging the notion of truth and accuracy in the narrating of personal stories. Participants tell their story at that moment in time in the way that they do, influenced by their contextual world at the time, and who the listener is. From this perspective, the story cannot be “wrong.” Transcripts might be returned to participants to provide opportunity to redact particularly sensitive information, but not to request a confirmation of “accuracy” (Dibley et al., 2020). Returning transcripts might be considered harmful to participants (Goldblatt et al., 2011) by increasing the likelihood of emotional distress – especially if there is a delay between data capture and the request for member-checking. To support credibility, the phenomenological practice of co-constitution was used during each interview (McConnell-Henry et al., 2011). Co-constitution involves the researcher and participant jointly confirming meaning during the interview to ensure the participant’s account is understood as intended. In this study, various verification statements were used with participants, such as “Have I understood correctly, that when you described X experience, it meant Y to you?.” A summary of what was heard and understood was also provided at the end of the interview to seek the participant’s verification of that understanding. Both techniques give opportunity for the participant to concur, or to offer further explanation to clarify meaning (Dibley et al., 2020); in the hermeneutic circle, meaning is continually interpreted through dialog between researcher and participants, where each clarification wave refines the understanding of the live experiences. Co-constitution is also practiced during analysis, whereby the emerging insights in the data are considered in the light of extant relevant literature and relevant notions from the underpinning philosophy, to create a new understanding–described by Gadamer as a “fusion of horizons” (H. Gadamer, 1975).
Data analysis was carried out by the first author (IM) as the PhD student, with support and comparative analysis to demonstrate credibility in interpretation, by TF, TT, and LD as supervisors.
In Stage 1, all transcripts (n = 18) were read, and audio files listened to by the first author (IM) and six transcripts were read by the co-authors; all identified early aspects of interest within the data.
In Stage 2, written summaries of each transcript were developed (IM); the early aspects of interest were then discussed by all authors, verifying that all had identified similar areas of interest, as well as a few unique areas. This overlap in identification of early issues of interest indicates that the preliminary analysis of each transcript was credible and would likely be reflected in others’ interrogation of the same transcripts.
For Stage 3, early findings were compared, discussed and agreed by all authors; transcripts were revisited to confirm presence of early relational themes and constitutive patterns in the data.
In Stage 4, all transcripts were revisited by IM; growing insights and understandings arising from immersion in and with the data were acknowledged during each new reading, demonstrating the hermeneutic circle; stages 3 and 4 were repeated until all transcripts had been carefully and thoroughly reviewed for all themes and patterns.
In Stage 5, the constitutive patterns were confirmed.
During Stage 6, the senior author (LD) provided analytical guidance, prompting further reflection on the relationship between themes, patterns, and their conceptual labels.
Stage 7 involved the development of the first author’s doctoral dissertation, which forms the basis of this report.
Findings
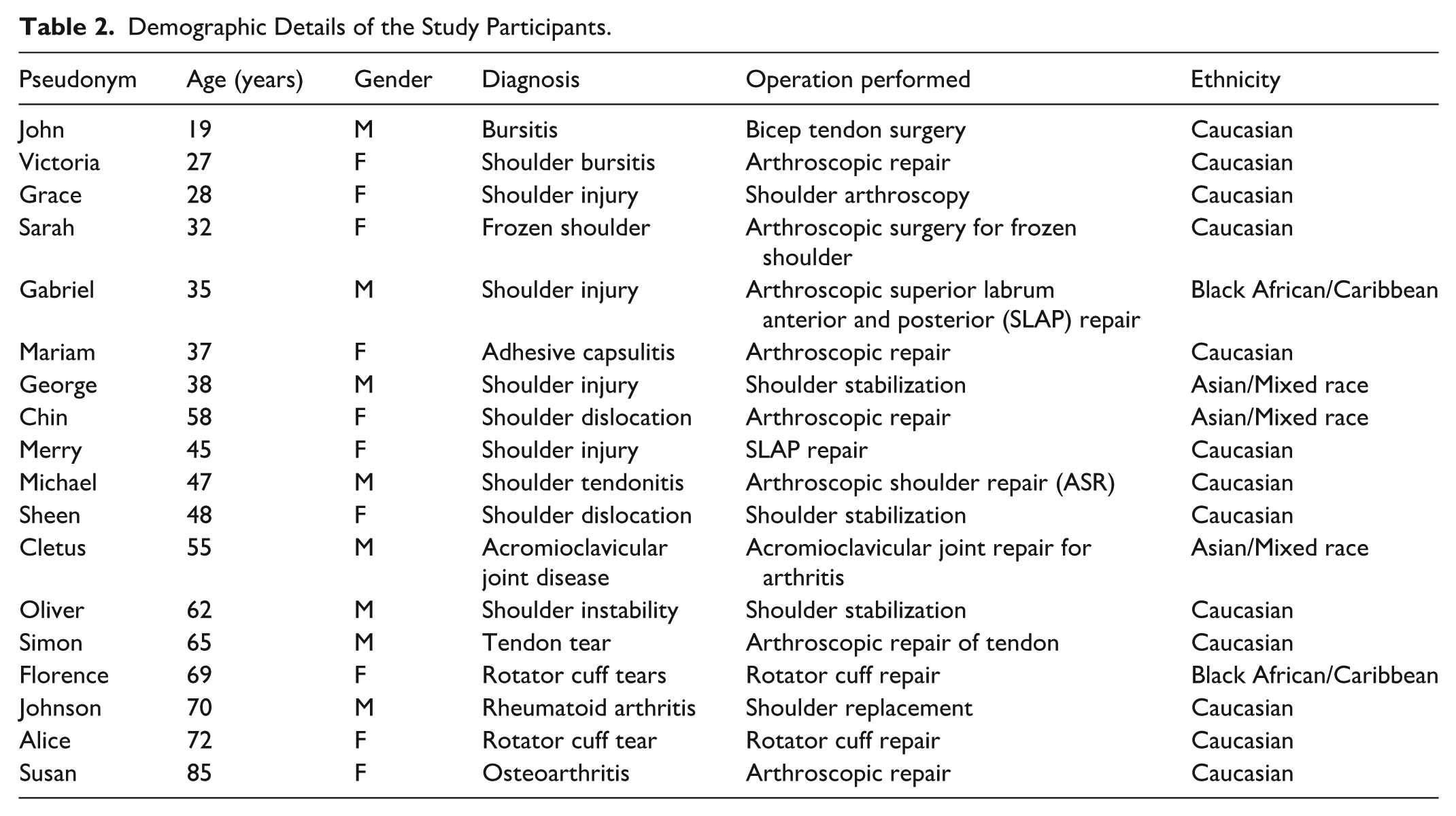
Twenty-five participants expressed an interest in the study and received the participant information sheet, four were lost to follow up, and three declined interview due to personal or health reasons. The remaining 18 participants (10 females, 8 males; aged 18–85 years) participated in unstructured interviews with the first author, contributing a breadth of experience that provided sufficient data to address the research question within a hermeneutic phenomenological framework. Table 2 provides an overview of participant characteristics. The mean age of participants was 49 years (range 17–83 years). Eight participants were male, and 10 were female. The majority of participants were Caucasian (n = 13), two participants were Black African/Caribbean and three participants were Asian or Mixed Race. Participants experienced a range of shoulder problems in the 3 years immediately prior to surgery.
Demographic Details of the Study Participants.
Participants’ stories revealed troubling experiences of shoulder pain post-operatively following discharge after day case surgery. Data analysis revealed four constitutive patterns (inner circle), informed by eight relational themes (outer circle; Figure 1); verbatim extracts are presented, with the participant’s pseudonym and age. A constitutive pattern is a concept that appears in all interview transcripts, thus representing a shared meaning amongst participants; relational themes arise in some transcripts, and add detail and context to one or more constitutive patterns.

The four constitutive patterns and eight relational themes comprising the experience of post-operative shoulder pain.
These patterns and themes revealed a complex and often distressing experience of post-operative pain that was often poorly managed, with participants feeling under-informed about pain management, rehabilitation exercises, and recovery trajectories and expectations.
Each constitutive pattern is presented below, supported by one or more relational themes. Verbatim extracts are offered, and allocated to participants by pseudonym, age, and type of surgery. In accordance with the co-constitutive world of hermeneutic inquiry, study findings are presented together with published literature, including the underpinning philosophy, to aid the interpretation of meaning that seeks resonance with readers (Crowther et al., 2017; Dibley et al., 2020). The aim is to provoke thinking in the reader and an acknowledgment of something that matters significantly (Smythe et al., 2008).
Constitutive Pattern: Suffering Perpetually in Pain
This pattern speaks to the nature of post-operative pain which some participants felt was never-ending. They were distressed by a level of pain that they had not expected, and its all-consuming nature contributed to a sense of relentlessness. Pain took over and rendered them incapacitated. The pattern is informed by the relational themes of Seriously disrupted and suffering in pain, Pain is a disability, and The unpredictability of pain.
Seriously Disrupted and Suffering in Pain
Post-operative pain caused significant disruption to sleep pattern, and quality, despite appropriate use of post-operative analgesia. Participants had difficulty adopting or maintaining a natural, comfortable, sleeping position; Florence (69, cuff rotator repair) reported that “My sleeping is diabolical. I slept for a couple of hours, and once you get comfortable, the pain wakes you up.” The grammatical tense here switches from the singular “I slept” to “the pain wakes you up,” suggesting that this was, in fact, a repeated occurrence for Florence and for others, including Johnson (69 years), following his shoulder arthroscopy: Well, no, you can’t sleep because you are in so much pain, you wake up every 20 minutes, 40 minutes, if you get back to sleep, suddenly you wake up again, more particularly if you mistakenly sleep on your operated shoulder unexpectedly, just have tablets like paracetamol, ibuprofen, by your bed-side with water.
Sleep is an essential physiological need that must be satisfied to ensure survival; lack of sleep can cause a range of neuro-behavioral deficits, including lapses of attention, slower working memory, reduced cognitive throughput, and depressive mood, with poor preservation of thought (Banks & Dinges, 2007). Repeated disruptions to sleep can have a cumulative and deleterious effect, including delaying the healing process (Das et al., 2025) and paradoxically enhancing the perception of pain (Palsson et al., 2023).
Simon (65, tendon repair arthroscopy) explained the distress caused by the severity of post-operative shoulder pain: I could not handle it, the pain was that severe, l felt like crying. I don’t cry, I don’t cry for the loss of family members, but this pain made me. I don’t cry at all [. . .] as I have got resilient to pain very well, but in this case, I cannot handle the pain; the pain is suffering, [it] was just unbearable.
Simon’s choice of words induced a powerful image that highlighted his distress and struggle against his perception of tortuous pain, as he compared the severity of his unexpected suffering to the loss of a family member.
There are a wide range of situations and events that challenge participant’s abilities and comfort after shoulder surgery. The challenges of post-operative shoulder pain are well documented (e.g., Misir et al., 2021) and when pain and suffering cannot be controlled, human dignity may be compromised (Pullman, 2002). Although the terms “suffering” and “pain” are generally interchangeable in medical and nursing literature, they are phenomenologically distinct (Chan et al., 1999). In some circumstances, pain does not involve suffering. For example, a woman may experience the pain of childbirth as severe yet rewarding, she might not describe the experience as “suffering.” Conversely, it is possible to suffer without experiencing pain (Bueno-Gómez, 2017) - for example, a patient with severe spinal cord injury might suffer because of the loss of bodily function, even though physical pain was absent or well-managed. Cassell (1992) acknowledges the relationship between pain and suffering, reporting that “People in pain frequently report suffering from pain when they feel out of control, when the pain is overwhelming, when the meaning of the pain is dire, or when the pain is acute or chronic” (p. 3). Heidegger (1962) proposed that pain encompasses both existential and concrete dimensions and is a fundamental aspect of human experiences. Accordingly, pain prompts humans to confront the temporality of their existence and leads to authentic living (an awareness of the finitude (finiteness) of our existence) and a deeper understanding of what it means to be human.
Pain is a Disability
Some participants, perceived their pain as disabling, in that it disrupted their ability to function, Florence (69, rotator cuff repair) stated: Oh, Jesus, unbelievable pain . . . [. . .] the pain is so extreme, that you felt someone has got a knife and stabbed you. So sharp, intense, like nerve pain, this completely makes you disabled in your usual activities and no idea when you will be back to normality.
A sense of disability also arose for participants when their dominant arm was affected, and they had to rely on their non-dominant arm to compensate. Merry (45, SLAP repairs) observed that “I never realized how much I depended on my dominant arm until I had to navigate life with just my other hand–it’s like losing a part of myself.” Participants were frustrated about the negative impact of disability caused by post-operative shoulder pain, which affected leisure and self-care activities, as Cletus, (55 years, acromioclavicular joint repair for arthritis) explained: “A lot of pain is happening to me, I can’t do anything useful, even the movement of my arm is impossible.” The pain restricted their willingness to mobilize the shoulder, disrupting ability to self-care and thus leading them to perceive their experience as disabling. For example, Oliver (62 years) whose surgery involved a shoulder stabilization, stated: “I can’t describe the pain, but I can describe how it made me immobile; it gave me a lot of restriction that prevented the movement of my arm following the operation.” Patients with persistent post-operative shoulder pain have previously reported decreased ability to perform activities of daily living, resulting in a reduced quality of life; the limitations and frustrations imposed by pain can lead to a sense of helplessness, further exacerbating the disability experienced by patients (Kraychete et al., 2016).
For these study participants, pain had an emotional impact; many felt that the pain became horrible to live with, and they felt “dragged down” as it continued. John (19 years) explained that following his bursitis bicep tendon surgery “I was just annoyed, as l could not drive, nor engage in my usual activities, including showering in the bathroom.” With no end in sight, participants became frustrated and miserable, perceiving themselves as disabled by their ongoing reduced functional capacity.
It can be challenging for nurses and surgeons to understand the degree of impairment caused, since pain can fluctuate during initial assessment and examination and the situation may change in subsequent months – yet it often causes significant disabilities (Krief & Huguet, 2006). For these study participants, the sense of disability may have been caused by the unwillingness/inability to move the affected shoulder due to pain. Several factors may be involved in post-operative shoulder pain leading it to be perceived as a disability. Bursitis for example, which is frequently associated with rotator cuff lesion, has significant links to disability (Krief & Huguet, 2006) as it prevents pain-free movement of the affected limb/joint.
Disability can be understood as a physical, mental, cognitive or sensory impairment which, when combined with other environmental and personal factors, disrupts the individual’s ability to participate as they would wish, to, in society (Bigby, 2023). Being able to function in the world, and with others, is fundamental to our lived world (Heidegger, 1962). Whether permanently or, as in this study, temporarily disabled, the social nature of being and the fundamental nature of being-in-the-world with others are significant (Heidegger, 1962) – in other words, how we are in the world informs our sense of who we are in the world. The phenomenological challenge for the study participants was the wish to continue their being-in-the-world with others, when their bodies were rendered disabled due to pain.
The Unpredictability of Pain
Participants were challenged by the changeable nature of pain, which could take them by surprise and cause concern. Oliver (62 years, shoulder stabilization recounted: “I have a few episodes of unexpected pain, sharp pain . . . [ . . .] my thought was, the worst had happened . . . thinking probably the operation hasn’t worked when you keep on having varied extreme pain, weeks after the surgery.” Pain was experienced as having an unpredictable nature, with participants describing their pain as “having electric shock,” “clunking,” “tingling,” and “swelling,” conjuring up images of undesirable pain that, as John (19 years, bicep tendon surgery) explained, materializes unpredictably without warning: “Pain appears suddenly, shocking pain that is hard to describe; you can’t even pinpoint how unpredictable the pain is.” Participants, including Oliver (62 years, shoulder stabilization) reported that this unpredictable pain was disruptive: “after the operation when you are sleeping–despite taking medication, pain woke you unexpectedly.”
Pain demands attention and prioritizes central nervous system resources to disrupt the selection of stimulus-processing responses (Torta et al., 2017); unpredictable pain means that there is no pain pattern, and intervention may be necessary to manage the changeable nature of the pain. Unpredictable pain can also be described as “some activity, new pain,” which usually indicates that the pain may be provoked by either exercise or shifts in position. It is accompanied by fresh symptoms, such as tingling, weakness, swelling, pain to touch, and instability (Alkandari & Hollywood, 2023). Changes in the pain sensation and unexpected episodes of pain can both be considered “unpredictable,” leading to a disruption of expectations for the individual. Dow et al. (2012) further report the frustration that disruptive pain causes, as it impacts on daily activities, life roles, and identity.
Sudden and unpredictable pain can be considered a “breakdown” in Heideggerian terms, a disruption to the everyday ebb and flow of being (Heidegger, 1962); when pain suddenly appears, it throws the individual into a situation of breakdown and anxiety (angst – uncanny or unhomelike) – a concern that things in their world (in this case, their affected shoulder) are not available for them to readily use, or have no purpose. Pain upsets the everyday ready-to-hand nature of the participants’ Dasein, when they cannot function in the way they normally would, thus causing anxiety and frustration.
Constitutive Pattern: Overcoming Pain
This second pattern explores the ways in which participants learnt to manage or rationalize their pain, often drawing on previous experiences. The pattern unites two relational themes: Perception of medication, and Acceptance of pain (readiness to withstand pain). The themes explore connections between participants’ social, cultural and family circles, and with healthcare professionals, which help them fight and respond to the threat of pain. Understanding pain through prior experience can have a considerable impact on patients’ later experiences of pain (Main et al., 2010). In this study, prior pain experience drove patients’ coping behavior and their responses to prescribed medications.
Perceptions of Medication
Study participants recognized the role that analgesia played in managing their pain symptoms but as Michael (47, ASR) explained, prior experience with analgesics and other health conditions, needed to be considered by the prescribing clinician: I have been treated with co-codamol . . . I have never found them good to me. I requested the morphine strength in patches because co-codamol was not effective on me, as I can’t have ibuprofen as I suffered from colitis; this gives me chronic stomach pain.
Michael discarded his co-codamol (a compound prescription analgesia containing 30 mg codeine and 500 mg paracetamol (acetaminophen) per tablet) and thus endured a painful post-operative period, because the prescribing clinician did not take his history into account. Other participants were ambivalent toward the use of analgesia but felt that these were needed after surgery to recover, Gabriel (35 years, arthroscopic SLAP repair) felt that “Those tablets are horrible; there must be a better tablet that helps the pain; it gives you hallucinations because it keeps you awake.”
Opioids remain essential analgesic drugs for alleviating pain, but use of these is plagued by major side-effects, including analgesic tolerance (diminishing pain-relieving effect), increased pain sensitivity, and drug dependence (Trang et al., 2015). Some participants thought that analgesics were not good for them for various reasons, including severe toxicity, side effects, and complications. For Victoria (27 years, shoulder arthroscopy) these aspects informed their decision to stop taking the prescribed post-operative analgesia: The side-effect of the drug made me take the decision not to continue with it . . . I looked at information on the internet, and stopped taking the painkillers for three days, made up my mind, I don’t need them, as codeine was having a negative effect and not given me the benefit (Victoria,
Whilst side-effects of prescribed opioids may be under-reported (Sivanesan et al., 2016), some participants had heard stories from friends and family about people who had suffered unwanted opioid side-effects, including Chin (58 years, ASR) who refused these drugs and tolerated pain due to social influences: Codeine is something that I am afraid of because of my [ethnic] DNA; whenever I have morphine, I am sensitive to it, that is why I do not want to deal with using codeine; but honestly, it has helped me with pain but doesn’t that much, even when I am in pain; my husband will ask me to take paracetamol instead of codeine.
Mayberry and Osborn (2012) have identified that family members can negatively influence patient behaviors toward medication adherence, leading to poorer symptom control. Attitudes and behaviors regarding taking medication are also influenced by factors such as health literacy, socioeconomic status, perceptions of the medication necessity and safety, and concerns over the likely efficacy of the medication for them (Linsky et al., 2015). In Heideggerian terms, conforming to a wider public opinion, such as a generally held belief about the addictive dangers of even short-term, prescribed, opioid-based painkillers, may cause patients to “fall in with” the majority view of “the They” (the wider population) despite the discomfort it causes them.
Acceptance of Pain (Readiness to Withstand Pain)
Some participants had a very stoic attitude to the post-operative pain they experienced, understanding it as a short-term disruption. For example, Mariam (37 years, arthroscopic repair, stated: “You just get used to the pain, and it’s not forever.” Pain acceptance is a valuable construct in the understanding of pain, and is associated with improved physical, social and emotional functioning (McCracken et al., 2004). Pain can also be differentiated by “admission” and “aversion.” Admission supports the reality of living with pain (learning to live with it), whereas aversion resists admission (desiring to become pain-free; Ojala et al., 2014). Alice (72, rotator cuff repair) addressed her admission of pain, as “getting on with it”: I have tried my best to get on with the reality; it is not as bad as I thought it was going to be, but I am quite lucky that I can deal with the pain, bear the pain but just need help around me to do some tasks.
LaChapelle et al. (2008) contextualize acceptance of pain as the “willingness to experience continuing pain without the need to reduce or avoid it,” and Alice’s words reflect an admission of her pain, which thus enables her to accept it, and cope with it. Similarly, Victoria (27, arthroscopic repair) expresses a willingness to accept the pain in order to be productive: “I am in pain, (but) I’m young; if I submit to pain, I would not be able to continue my daily activities.” Healthy levels of self-esteem also enable participants to accept, respect, trust and believe in themselves; having opportunities to develop confidence and problem-solving skills is an essential aspect of self-esteem and can help deal with and accept pain and other life experiences. Self-esteem, and self-respect can also contribute toward how patients coped with pain; Cletus (55 years, Acromioclavicular joint repair) explained that: “The pain was too much for me, but I hold on to it as I do not want my children to see me crying” (Cletus)
Choice theory (Glasser, 1999), which focused originally on mental health and relationships, can be applied to physical pain and may account for participants’ notions of coping with and accepting pain. Choice theory suggests that we have control over our thoughts and behaviors, and our choices can influence our physical and emotional experiences, as Florence (69 years, rotator cuff repair) illustrates: My decision to continue to use my hand, even with presence of pain, helped me better in using my arm; I realized, now I can use my right hand to hold things, bearing the pain but mindful not to do anything stupid with my shoulder.
The concept may also help us understand how Alice and Mariam cope with pain by changing their thoughts and behaviors toward it. Alternatively, their responses could be ascribed to the concept of reframing–changing the thinking about a situation to change related emotions and behaviors (Fereydouni et al., 2019). Instead of thinking of pain as a negative experience, an individual can reframe their thoughts to view pain as a helpful signal from the body that something needs attention (Fereydouni et al., 2019). This shift in participant thinking can help the individual to accept the pain and act to address the underlying issue in coping with it.
Heidegger reminds us that all new experiences are influenced by all that has already been; his concept of thrownness proposes that where we land in a new experience, and how we understand and make sense of that new experience, is necessarily influenced by where we have already been in our journey through life; thus, philosophically, our past is always before us (Withy, 2014). Past experiences of pain, or of coping with and overcoming challenges, therefore inform present and future experiences and an individual’s pain history and familial model can help with the prediction and management of post-surgical pain (van Driel et al., 2022; Yoo et al., 2023). These participants’ pre-understandings, and prior experiences of pain, likely informed the way they chose to deal with contemporary post-operative shoulder pain.
Constitutive Pattern: Living in an Unfamiliar Body
This pattern is informed by two relational themes: The painful body as unhomelike, and Inability to self-care and dependency on family and social support which together, reflect particular experiences of living in an “unfamiliar” body – a body which is not functioning in the expected way. Together, these themes reveal one possible meaning of post-operative shoulder pain, the significance of which lies in the lack of understanding from family and friends. Participants felt they were perceived as a burden during this critical period; they intentionally turned inwards, away from external activities, and their relationships with others were affected (Kitzmüller et al., 2013).
The Painful Body as Unhomelike
A healthy body can be understood as a coherent body, with parts that work in harmony and sustain the peace of everyday activities that insert us into a particular environment. A body in pain loses its natural rhythm or way of doing things; when there is a breakdown in our natural activities, our plans or expectations are placed in shadow, and incoherence occurs (Manea, 2021). George (38 years, shoulder stabilization) experienced this breakdown when his dominant hand was affected: I am right-handed and could not raise my shoulder when I’m in the toilet, so hygiene was a challenge. And eating with my left hand. It was very frustrating, especially cutting something to eat properly was very difficult, [as was] looking after the kids, supporting them.
Similarly, for Cletus (55 years, acromioclavicular joint repair) the temporary inability to use his dominant arm felt “very challenging because I am left-handed, and obviously, most day-to-day functions I do (with that hand) because my left hand is my dominant one. I am not good with my right hand.”
Participants recounted severe restrictions and immobility due to reduced shoulder movement, often due to pain, or sling application. Sarah (32 years, arthroscopic repair of frozen shoulder) explained: On my normal days, I set myself ready to go to work and return late at night, three times a week, and the other days catch up with sleep, housework, shopping, visiting, or receiving friends and family. Currently, I can’t do any of these activities.
Post-operative pain heightened participants’ awareness of the disruption of their everyday ways of being-in-the-world, as they were (temporarily) not “at home” with their bodies. The implication of these participants’ experiences is that the shoulder plays a larger role in daily life than people realize, and a temporarily disabled or broken body/shoulder causes difficulty with undertaking typically easy and routine tasks. The arms become “unready-to-hand” due to the shoulder surgery – Heidegger (1962) postulated that our lives are surrounded by tools that we take for granted as being available to us; it is only when the tool (or shoulder/arm, in this case) is broken or fails to function normally, that we become fully aware of its presence and it’s now unready-to-hand status. In this study, it was only when the taken-for-granted shoulder became unavailable for use, that participants fully realized the normal utility of that shoulder in their everyday functioning. Disruption in the normal flow of everyday life, of things (tools) being ready-to-hand – is described by Heidegger as “breakdown” (Dahlstrom, 2023). Such breakdown can be understood as angst, an incoherence that can itself be understood as “unhomelike.” For George, Cletus, Sarah, and others, unhomelikeness was precipitated by pain which prevented them using their dominant arm and thus disrupted their everyday way of being-in-the-world when they were forced to try and function with their non-dominant arm. Not-being-at-home with the body appears in many forms of illness, manifesting at any time through fatigue, pain, or other symptoms (Svenaeus, 2013).
Inability to Self-Care and Dependency on Family and Social Support
The complexity of living with post-operative shoulder pain had adverse and profound impacts on participant’s emotions, resulting in feelings of depression, fearfulness, and guilt that were associated with being dependent upon families and other sources to help them with daily living. Susan (85 years, arthroscopic repair) described the extra help she had to accept: I can only manage to dress - well, I don’t do that myself, the carer helps as I could not, I’m learning to do the buttons with both hands, although I can’t put anything over my head, that is out of the question, and one of my sisters is residing with me at the moment. Before the surgery, I lived alone, but she is here with me now, ’til l recover. In addition, I have a cleaner supporting me too.
Families often play a critical role in meeting the care needs of individuals who require assistance due to illness or disabilities (Kokorelias et al., 2019). Social support and help from others during difficult times can be considered a form of material, spiritual care (Zhang et al., 2018), and the involvement of families in patients’ recovery periods improves the quality of care and surgical outcome (Brembo et al., 2017); Victoria (27 years, arthroscopic repair of shoulder) acknowledged that “It would have been completely difficult if I did not have my husband here.”
Despite these known benefits, several participants shared their frustrations regarding having to cope with the transition from being an independent self-caring person to becoming dependent upon their spouse, family members, or carers to support them with various activities, including personal hygiene and dressing. Simon (65 years, arthroscopic tendon repair) described this dependence in detail: My wife was helping with daily activities, showering, scrubbing my back, supporting me when eating, combing my hair; the first two to three weeks were not easy, as I had to use my left hand with cutlery, and had to change what I ate, such as sandwiches
Help was needed particularly with upper body activities, due to reduced movement, stiffness of the affected arm, or restricted movement due application of a sling (to immobilize and stabilize the joint post-operatively, ensuring safety and promoting healing). Even though this situation was temporary, it was troubling to many participants as they struggled to maintain personal care and undertake tasks following surgery, possibly impeded by swelling around the arm and shoulder following surgery (Magone et al., 2021). Having an illness that requires support can impose burden on family members (Ennis & Bunting, 2013; Wittenberg et al., 2013), a feeling that seemed to discomfort George (38 years, shoulder stabilization): To rely on people, this made one feel like burden, the fact that I am constantly having to ask for help in doing things, they may not mind, but the fact remains, it could create an avenue that you are a burden (George, 38, shoulder stabilization).
In phenomenological terms, Svenaeus (2011) proposes that when stricken with illness, the implicit sense of feeling connected and “at home” is replaced with an uncanny sense of feeling “unhomelike” – things that used to be familiar and comforting suddenly become incomprehensible and strange. The taken-for-granted, coherent and intelligible world becomes a disorienting, alienating, even unfriendly place. Phenomenologically, the person cannot be their own-most being, as revealed in the experiences of these study participants. Pain made them struggle with the usualness of their being. Heidegger offers the notion of Sorge – care about, or concern for something (rather than to take care of someone). For these study participants, the meaning structure of post-operative shoulder pain is articulated as a person’s Sorge/concern about being thrown into a world that is strangely unfamiliar or unhomelike. Their painful, broken bodies that temporarily failed to function post-operatively became unhomelike and foreign to them; this dysfunction threatened the unity of the body and being-in-the-world was disrupted (Carel, 2011).
Constitutive Pattern: Communicating and Lacking Essential Information
This final constitutive pattern is informed by the relational theme: Realistic pain management information, and revealed the meaning of essential information, as participants explained the importance of accurate information regarding their care management, when they were discharged home. Effective communication exchanges between healthcare professionals, patients and those who look after them at home, such as families, friends, and carers, are essential (Markides, 2011) as inadequate communication can lead to poor and even dangerous health outcomes for the patient (Tiwary et al., 2019).
Realistic Post-Operative Management Information
Poor communication experiences were reported by participants; they experienced gaps in communication ranging from a lack of effective communication and poor guidance pre-operatively, to a lack of practical information regarding the post-operative period, and contradictory information from healthcare professionals. Mariam (37 years, arthroscopic repair) described how she had not known to expect that a sling would be applied: I probably should have asked the clinicians if my arm would be in a sling; I was surprised that I found my arm in it and admit they did not tell me. The clinician was very busy as I was seeing his registrar, and he just came in and said ‘you need to do so and so’, but the sling aspect was not told to me.
For the clinician, the need for a post-operative sling to support the shoulder may be a taken-for-granted issue, so obvious that they may assume the patient would also realize this requirement. Yet there is a wide range of health literacy amongst patients, and to assume they know what to expect is unhelpful. Had Mariam known to expect a sling, she may have been able to better prepare herself for restricted abilities once discharged by making plans to have support in place.
Just as Mariam was ill-informed pre-operatively other participants, including Michael (47 years, shoulder stabilization) spoke about confusion in the post-operative period in respect of rehabilitation: “[The physiotherapist] was unsure about what type of physio exercise to give me because the written [discharge] document did not specify and there were not many details as to what could be done [while] I was recovering at home.”
Post-operative exercises are tailored to the surgical intervention and cannot be determined pre-operatively as the surgeon will be unaware of what action would be required after surgery, until they enter the operation site. However, having completed the procedure, precise instructions for post-operative rehabilitation should be included in the discharge document. Proper communication is essential to avoid the negative consequences of patient dissatisfaction and decreased adherence to post-operative treatment (Tiwary et al., 2019), which can delay recovery. The uncertainty that arose due to the lack of detailed explanation, resulted in fear of pain and anxiety for Michael.
In health care environments, pre-operative assessment is typically carried out as part of surgical planning; during this assessment, post-operative management – including pain management, post-procedural and discharge information – should be discussed with patients. Information helps reduce patient concerns and assists them in preparing for their post-operative recovery at home.
A general principle of rehabilitation that follows some shoulder surgeries, in particular, rotator cuff repair, is to provide a sufficient period of immobilization to achieve reliable tendon healing while a passive range of exercises are undertaken to prevent stiffness (Jeon & Kholinne, 2020). Participants were concerned about a lack of clarity on how the sling should be managed, leading to a sense of frustration and disappointment with health care professionals. Simon (65 years, arthroscopic tendon repair) addressed the confusion this lack of clarity could cause: I need more information as it is the key; I was confused at some stage; when I saw the surgeon, he said ‘all right, take it off tomorrow and do your exercise’, and the nurse sort of looked [and said] it wasn’t (ready) . . . (there were) not too many aftercare specific instructions of what you were supposed to do, but ‘the physio will tell you a lot more’ . . . but if certain essential information is missing in your notes, it will make it harder to get the knowledge expected.
Participants received contradictory information from healthcare professionals, which caused confusion and was challenging to decipher. Heidegger (1971) considers that language is the most powerful tool that humans have developed, and that it is used iteratively to address the back and forth of interaction between each person and their contextual, situated world which they are constantly interpreting to reach new understandings. Effective communication is the same – it is a continuous, circular process by which information, such as ideas and feelings are transmitted between people and their environment, leading to a new knowledge/understanding. The goal of communication is to understand and to be understood, and in healthcare, is essential for safe and effective patient care (Amudha et al., 2018); if either party does not understand the purpose of the information conveyed, communication cannot be considered to have been adequate (Ratna, 2019).
Discussion
To our knowledge, this is the first nurse-led study to explore the meaning of living with post-operative shoulder pain following day surgery discharge, using hermeneutic phenomenology. Heidegger’s notion of “being-in-the-world” (Dasein) is an understanding of everydayness which is brought into consciousness when events interrupt “normal” activities (Heidegger, 1962). In this study, everydayness was disrupted by pain, a nebulous phenomenon that we tend to treat as something to be explained (Hillard, 2014).
Perhaps the most common biomedical explanation locates pain within the domain of sensation and feelings. The etiological and pathophysiology of post-operative shoulder pain remains poorly understood and it is difficult to define how tissue damage and nociceptive stimulation influence perception of pain following shoulder surgery. Pain experience does not correlate directly with the state of the tissue and many factors across somatic, psychological and social domains influence pain modulation (Moseley, 2007), which may help understand explain why most participants in this study experienced severe, excruciating, unpredictable and debilitating pain.
A second explanation locates pain as a facet of disability, and it is this that captures the core meaning of the experience of these participants. Kenkmann (2005) encapsulates Dasein’s being-in-the-world succinctly by stating “We are to a great extent what we do” (p. 480), but what does this mean for patient with a disability? It is impossible for patients with shoulder disabilities to “do” anything, at least for a period of time during recovery and rehabilitation; it is difficult if not impossible to hold an item or undertake daily living activities when the pain is present. The perception of pain as disability can be understood through an appreciation of the impact of the ill body on being-in-the-world (Svenaeus, 2011). Svenaeus suggests that illness evoked an unhomelike or uncanny way of being in the world, which he called “das unheimlich” (scary). Unhomelike being-in-the-world ascertains that we know the world in which we are engaged and thus understand when that “knowing” is disrupted (Svenaeus, 2011); pain that is experienced as disability gives rise to “unhomelikeness” and distances us from our known world, which, for the most part, we yearn to return to – a desire most commonly expressed as “returning to normal.”
There is an ever-growing body of evidence which explores the concepts of chronic and/or acute pain (e.g., Morley, 2008; Moseley, 2003; Smith & Osborn, 2007). Attitudes, informed by previous experiences of pain, are likely to influence the perception of later experiences of pain. Other responses, for instance, catastrophizing, or anxiety over what to expected, are linked to heightened pain experiences, whilst strong social support and an individual’s resilience may help improve pain (Sullivan et al., 2001). The psychological distress experienced by some of the participants in this study evidences the importance of acknowledging and addressing patient expectations, social isolation, unhomelikeness, and procedure-related anxiety in a timely manner, when managing post-operative shoulder pain.
The experiences of pain can also be understood from pharmacological and social perspectives. Study participants had negative perceptions of their pain medication due to anxiety about side effects; they were willing to forego pain relief and endure suffering, so intense were their concerns. Ninety-two percent of patients with acute pain post-operatively develop at least one side effect due to pain medication, such as nausea, or vomiting (Benyamin et al., 2008; Gregorian et al., 2010), but negative assumptions by participants in this study regarding side-effects resulted in lack of adherence to prescribed post-operative analgesia (Gast & Mathes, 2019; Markotic et al., 2016) and potentially contributed to unnecessary suffering.
Participants valued the emotional and practical support they received from family and friends during their post-operative recovery. Social support promotes self-management, encourages adherence to medication regimens and improves clinical outcomes. Related evidence demonstrates that family and friends play a crucial role in providing support and helping patients with chronic lower back pain to manage the pain (Alatawi et al., 2024; Shahin et al., 2021).
The findings in this study offer insights into the physiological, disability, pharmacological and social meanings associated with the experience of post-operative shoulder pain following day case surgery. Findings also suggest the need to reconceptualize the treatment planning to facilitate an improved post-operative recovery experience for patients having shoulder surgery. Several issues have been identified which may improve patient care, including the need to pre-operatively acknowledge patients’ relevant experiences in relation to drug history, and how their views may influence their preferences in respect of pain management. Participants valued social support by expressing a wish for their pain to be understood by family and friends involved in their post-operative care. Therefore, postoperative analgesia management should focus on the management of pain from different perspectives, and include the involvement of relatives, friends and clinicians in teaching and education. Such an approach would aim to understand what it means to be in pain after surgery and offer beneficial social support that would change adherence to pain medication positively. Social support has long been recognized as a very important factor in recovery and treatment adherence (Alatawi et al., 2024; Shahin et al., 2021). Patients who have day case shoulder surgery need accurate and timely pre-operative information so that they know what to expect during recovery and understand their post-operative analgesia and its role in supporting rehabilitation. There is evidence that the use of a preoperative patient information and educational program has promoted better outcomes after hip and knee replacement surgeries (Moulton et al., 2015); a pre-operative “shoulder club” could be an effective vehicle for addressing patient concerns and setting expectations in relation to elective shoulder surgery.
Strength and Limitations
This nurse-led hermeneutic phenomenology study has prioritized participants’ voices and has added to the qualitative evidence that can help nurses and other clinicians involved in care to better support patients undergoing day case shoulder surgery. The study has produced knowledge that generates new understanding and points the way toward future follow-up research, for example, the introduction and evaluation of a pre-operative “shoulder club” to better prepare patients for surgery and set realistic post-operative expectations.
There are some study limitations. Participants were recruited from those undergoing day case surgery in one UK hospital; experiences may have been different in other locations, and for other patients. There is a possibility that having to collect data remotely via telephone or video-conferencing calls due to Covid-19 restrictions may have reduced the richness and depth of data that can be better obtained via in-person interaction. Non-English-speaking patients were not invited to participate in the study as the use of a translator could have affected the expressive element of a participant’s story; it would have been challenging for the translator to decipher the emotion expressed within the spoken language and to share this with the researcher, for the researcher to understand participant’s meaning. Future qualitative research could further explore the experiences of diverse cultural and ethnic groups undergoing shoulder surgery.
Trustworthiness
Throughout this study, trustworthiness, credibility, and dependability were supported using numerous techniques including clear explanation of study processes, thus demonstrating robustness. Having enough participants to address the research question and generate rich, deep data supports transferability of findings and enables readers to judge relevance to their clinical population. Team contribution to early theme development and analysis, common in hermeneutic phenomenological research, enhanced credibility and trustworthiness by reducing individual influence on analysis, and by enriching interpretation (Crist & Tanner, 2003); benefits include guarding against misinterpretation (Cornish et al., 2014; Morse, 2015). There is philosophical and methodological diligence in data collection, analysis and reporting techniques; the findings are evidenced through use of verbatim data extracts so that the reader can have confidence in the accuracy of reporting, and the recommendations made. Reflexivity was practiced throughout, encouraging researchers to step back from taken-for-granted assumptions and increasing transparency (M. Clancy, 2013; Cornish et al., 2014).
Conclusion
This study has contributed to the nursing research about understanding the meaning and management of shoulder pain that occurs after discharge from day-case surgery. The hermeneutic phenomenological approach has revealed the core meaning of the experience as “unhomelike,” adding to the clinical knowledge and understanding of patients’ experiences of living with postoperative shoulder pain. In this study, the significant findings were patients’ concerns as they found themselves suffering in perpetual pain, living in unfamiliar bodies due to not being themselves after surgery, their unwanted and unexpected reliance on support from families and friends, and the poor quality of pre-, peri- and post-operative information which compounded these challenges. Better information strategies, including a pre-operative shoulder club, may reduce post-operative anxiety and consequently, reduce post-operative pain. Such approaches could reasonably be considered for appropriateness in this setting, as the current framework of day surgery is not sufficient to address these concerns.
Footnotes
Acknowledgements
The authors extend their thanks and appreciation to the study participants for sharing their valuable experiences with us. Their insights were instrumental in enhancing the quality of the study. We also appreciate the transcription service for their vital role in accurately converting the patients’ voices into text.
Ethical Considerations
Ethical approval for this study was given by the National Research Ethics Committee (Oxford C): Ref: 14/SC/1121. All participants provided informed consent prior to interview.
Author Contributions
Study conception and design: Isa Makama Muazu, as a PhD student. Study supervision: Terence Ferns, Trevor Thompson, Lesley Dibley. Recruitment and data collection: Isa Makama Muazu. Data analysis and preliminary development and finalizing of themes: Isa Makama Muazu. Agreement of final themes: all authors. Original manuscript writing: Isa Makama Muazu. Revisions during manuscript preparation: all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PhD program that enabled this study was supported in part by King’s College Hospital NHS Foundation London, University Hospital Lewisham, and The Association for Perioperative Practice. Data collection and transcription were partly self-funded by the first author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Study participants did not give consent for use of their anonymized data beyond this study.