
Abstract
The realm of alternative care for children covers a variety of care systems, which include residential care, small group homes, mother and child shelters, transit homes, adoption, foster care and kinship care. The United Nations General Assembly’s 2019 resolution on children’s rights emphasises the significance of family-based environments for children, particularly those without parental care, and underlines their right to grow up in a family setting. In light of this resolution, kinship care emerges as a crucial family-based care avenue for children lacking parental care.
In India, kinship care stands as the predominant form of care for children lacking sufficient parental support and is the most common form of care in almost all regions, religions, castes and ethnic groups due to the tradition of the joint family system and close ties among relatives. While this care option is the most common form of out-of-home care, it is also the least systematically recorded, monitored or supported structure. The study, through the lens of kinship carers, ward and village-level child protection committees and community workers, focuses on the important aspects of support, motivation, love, responsibility and challenges that underlie providing care for children without parental care.
This qualitative study employs ethnographic interview techniques to understand the most authentic experiences of kinship carers. Families were initially identified based on secondary data captured from the assessment and intervention planning done using the Thrive Scale™ tool as part of the case management process. Subsequently, semi-structured interviews were conducted with six families from two different communities (one urban community in the state of Maharashtra and one rural community located in the state of Gujarat in India) to assess the existing support structures available for kinship carers and their families, identifying gaps and measures being taken to address them to ensure meaningful well-being of children and kinship families. The study discusses various challenges of kinship families, from financial struggles to familial disconnection, lack of housing infrastructure or access to healthcare, family issues like alcoholism or child labour, lack of education or livelihood and social isolation. The study further recommends increased attention and resources directed towards supporting kinship carers, acknowledging their invaluable role in providing love, support and stability to children without parental care, and also emphasises the importance of recognising and formalising kinship care within a broader framework of alternative care for children.
Miracle Foundation India is committed towards ensuring that every child has an opportunity to grow up in a family, to become a healthy, happy, income-producing person and to experience a true sense of belonging. The paramount significance of kinship care is recognised by Miracle India in its sphere of both the prevention of child separation from family and reintegration work. After a thorough assessment of these families on the five key domains of well-being—physical and mental health, education, family and social relationships, household economy and living conditions—and continuous monitoring and follow-up, Miracle India provided a comprehensive support service to these families, strengthened them and ensured sustained access to support services, ultimately promoting child welfare. During this study, the focus remained on prioritising the implementation of supportive policies and resources for kinship caregivers to ensure that every child in vulnerable circumstances thrives within the warmth and stability of a loving and caring family.
Keywords
Introduction
One of the core and critical components of children’s rights is the right of children to be protected. This right is key to the growth and social development of a child. Children across the globe have been experiencing increased vulnerabilities as well as living in difficult circumstances. Very often, their circumstances can be a result of poverty, living in war zones, natural disasters, single parenthood, separation from family as well as loss of one or both parents. An inadequate care environment can impact the children adversely. Their growth and their socio-development can be hampered and can also lead to their abuse and exploitation. When these children do not have access to a family or parent(s), a continuum of care must be explored in alternate care arrangements to ensure the child/children’s best interests are protected and safeguarded.
The United Nations Guidelines for the Alternative Care of Children (United Nations Digital Library System, 2010) mention that alternative care is:
Where the child’s own family is unable, even with appropriate support, to provide adequate care for the child, or abandons or relinquishes the child, the State is responsible for protecting the rights of the child and ensuring appropriate alternative care, with or through competent local authorities and duly authorised civil society organisations. It is the role of the State, through its competent authorities, to ensure the supervision of the safety, well-being and development of any child placed in alternative care and the regular review of the appropriateness of the care arrangement provided.
Alternative care arrangements can be broadly categorised as residential care, small group homes, mother and child shelters, transit homes, adoption, foster care and kinship care. The resolution adopted by the UN General Assembly (UNGA) on the Rights of the Child in 2019 laid emphasis on children who were living without the care of parents and mentioned that, growing up, children, including those with any form of disability, have a right to a family (Better Care Network, 2019).
Kinship care has emerged over the years as one of the important alternative care arrangements globally. Kinship care can be defined as ‘Family-based care within the child’s extended family or with close friends of the family known to the child, whether formal or informal in nature’ (Family for Every Child, 2024).
Just as globally, kinship care is an important form of alternative care for children in India. In fact, it can very well be said that kinship care exists in the very DNA of Indian society. India has a history of kinship care being practised in traditional set-up without any formal legislative or operational framework in the communities (India Alternative Care Network, 2023).
Objective of the Study
The objectives of the study include:
To understand the family strengthening journey of kinship care families through the lens of the case management process, leveraging the Thrive Scale™,
1
a family strengthening intervention planning tool covering the five well-being domains. To assess the existing support structures available for kinship carers and their families. To identify the gaps and the measures being taken to address those gaps so that meaningful well-being of children and kinship families can be ensured. Based on the findings, provide key recommendations that can help support kinship carers, acknowledging their invaluable role in providing affection, support and stability to children without parental care.
Literature Review
Across the globe, there have been very few but significant studies on kinship care. One such study mentions, through its primary research carried out in 40 high, medium and low-income countries, that kinship care is one of the most widely used options for those children who cannot be cared for by their parents (Family for Every Child, 2022).
Though there is a lack of adequate literature on kinship care and its nuances, and challenges in India, among other things, have not been documented well, it is a well-known fact that kinship care has existed in the country for a very long time and mostly as an informal set-up.
The child rights principles mentioned in the United National Convention on the Rights of the Child (UNCRC), as well as the UN Guidelines for Alternative Care of Children (the former ratified and the latter endorsed by India), set the tone for developing the narrative on alternative care and for developing family-based solutions for vulnerable children in India. This narrative was based on the child rights principles, which mention that a child’s development can happen successfully in a nurturing family environment.
Key Indian legislation for children, such as the Juvenile Justice (Care & Protection of Children) Act amended 2021, mentions that a child care institution (CCIs) should be considered as the last resort for children. Similarly, the Mission Vatsalya [formerly called the Integrated Child Development Scheme (ICPS)], which is to be implemented across the country at all levels—central, state, regional as well as at the district—is another key document that emphasises children living in the family set-up. In fact, in the vision statement, it is mentioned that Mission Vatsalya promotes family-based non-institutional care of children in difficult circumstances based on the principle of institutionalisation of children as a measure of last resort. This was indeed a significant moment when family-based alternative care was given a much-needed push in India.
During the COVID-19 pandemic, a large number of children were sent back from CCIs to their families as a precautionary measure following directives from the Supreme Court. The Supreme Court urged the state governments, as far as possible, to ensure safe and permanent reintegration with biological families, extended families and kinship care, such that children do not return to the CCIs.
In 2023, the India Alternative Care Network came up with a case study documentation with research done in Tamil Nadu, Jharkhand, Maharashtra and Assam, which was done with the support of four different Indian organisations. Two partner organisations supported the process of interviewing families, and the District Child Protection Units were also consulted during this study. This study highlighted the importance of nurturing family environments for all children. The study also advocated for family-based care for those without parental care and support (India Alternative Care Network, 2023).
Recently, the Government of India launched the revised Model Foster Care Guidelines 2024. While these guidelines did not mention kinship care, they did mention that the revised guidelines ‘have been framed to ensure clarity, efficiency and compliance amongst stakeholders about foster care to facilitate de-institutionalisation of children care’.
India is making slow but significant moves towards de-institutionalising children (as and where it is possible) and rehabilitating them in family-based alternative care systems, as well as working towards quality after-care for the care leavers.
Methodology
The study covers six families of kinship caregivers from the states of Maharashtra and Gujarat. Two families live in Warje Malwadi village in Haveli Taluka of Pune district, Maharashtra, while four families live in Khodivali and Gungawada villages in the Chota Udepur district of Gujarat. The locations for interviews were deliberately selected to be in rural and urban areas, given that the contexts were different and often the nature of support received could also vary.
The methodology consisted of:
Analysing the secondary data from the Thrive Scale™ tool on five well-being domains as part of the case management process towards strengthening the families. Primary data were collected through:
◦ Semi-structured interviews with selected kinship caregivers. ◦ Focus group discussions (FGD) with members of the village and ward-level child protection committee and community volunteers in both communities.

The data captured by the team in the Thrive Scale™ tool from May 2020 to July 2023 were analysed. Figure 2 shows a snapshot of the case management process followed by the team with these families, whereas the objective of collecting primary data was to broadly understand the nature of intervention, support services available to the kinship caregivers and their effectiveness, as well as the challenges faced, both from the lens of kinship caregivers and child protection committee members. The questionnaire created for the interviews and FGD are shown in Annexures A and B, respectively.

Data Analysis of Six Cases and Findings Based on Thrive Scale™
This section of the study delves into the lives of the six kinship families located in Warje Malwadi village in Haveli Taluka of Pune district, Maharashtra, and Khodivali and Gungawada villages in Chota Udepur district of Gujarat. The Thrive Scale™ leveraged in the process is a strengths-based assessment tool used to identify strengths and risks and address areas of support within a family home over time. Based on the assessment through the case management process as mentioned above, family strengthening interventions such as training parents on parenting skills, linking family with appropriate schemes and services, life skills training, health and hygiene, educational support, psychosocial support and career counselling were planned and carried out with the respective families, and progress is tracked. The tool draws special attention to critical safety concerns in the life situations of a child and family. These critical safety concerns (red flags) must be promptly addressed as an utmost priority.
The case management process for all six families was started in the year 2020, with five out of six families were identified, and one family was identified in 2023. In Maharashtra, the baseline assessment was done in May 2020, and the last monitoring visit was done in July 2023, whereas in Gujarat, the baseline assessment was done in June 2020, and the last monitoring visit was done in April 2023. Over the 3 years (2020–2023), on average, Thrive Scale™ assessment was done for each family once a quarter. The following graphs depict the aggregate score of the Thrive Scale™ for six families from the baseline done in 2020 to the last visit done in 2023. Interactions were done with the children and families, and using the Thrive Scale™, the situation was assessed across five well-being domains.
Family 1
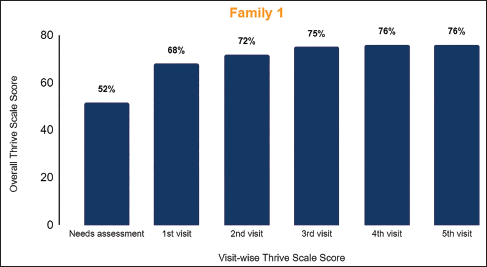
Mr Sharma (caregiver), the head of the family, lost his son-in-law 3 years ago, and his daughter got married to another man, which left his grandson, named ‘Prince’ (name changed), in his custody when he was just 11 years old and studying in fourth standard. The whole family runs a small home-based kirana shop. The grocery shop, on average, generates around ₹1,000–1,500 a month, and his wife’s housekeeping work earns them ₹6,000 a month; this makes the entire family income of ₹7,000–7,500. The family lives in their own house but with communal facilities, since their toilet is not complete. The school expenses of Prince are borne by the employer of the caregiver’s wife. Though Prince is an active boy, he is an introvert and also faces educational challenges with the problem of possible sponsorship. The family had strong social relations, but economic instability and tension between Prince and his mother resulted in a baseline score of 52 per cent, where the domain of health, mental health and education were also affected. After 3 years of targeted interventions and support, the family’s score improved to 76 per cent, reflecting significant progress and thriving.
Family and social relationships: Training grandparents on parental skills. Involvement of the child in Bal Panchayat activities to enhance social interactions.
Health and mental health: Psychosocial support and counselling sessions for the child to address his introverted nature and emotional needs, and for the family to cope with stress and trauma.
Education: Provided school materials and assisted with Balsangopan (Bal Sangopan Scheme, n.d.) scheme documentation to ensure child’s enrolment and continuation in school. Additionally, the child was linked with educational scholarships and got support in tabla training classes.
Household economy: Ration support was provided twice during COVID-19, and an old age pension scheme was explored for the caregiver. A public provident fund (PPF) account was opened for the child’s financial security, and financial documentation, including the income certificate, was facilitated.
Living conditions: Assistance in completing the application process for the ration card and addressing household economic challenges to improve living standards.
Family 2
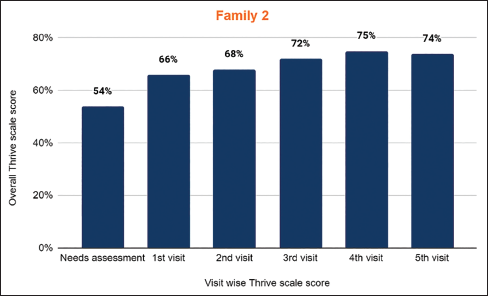
Amir (name changed), a 10-year-old boy studying in the fourth standard, was left alone with his grandmother when his father died and his mother ran away. Initially living with his grandmother after the death of his parents, Amir faced another loss when his grandmother was diagnosed with late-stage mouth cancer and ultimately passed away. Now, Amir resides with his uncle and aunt (caregivers). Amir’s uncle has taken him in, but he struggles with alcohol addiction and has little involvement with Amir’s care. The baseline score of Amir’s family was 54 per cent. Post-intervention and support, Amir is now actively pursuing his education, currently studying in the eighth grade and attending school regularly. Counselling has been given to his uncle about his alcohol addiction, and measures have been taken to inform him about support schemes and the process of documentation. The latest overall Thrive score of the family is 74 per cent, and the process of evaluation continues.
Family and social relationships: Counselling sessions were provided to strengthen Amir’s bond with his grandmother, his primary caregiver. Amir was involved in community activities like Bal Panchayat groups to enhance his social connections.
Health and mental health: Asha workers and auxiliary nurse midwife (ANM) raised awareness about healthcare services, insurance and emergency facilities, while Amir’s grandmother received counselling on child care and follow-ups for her health needs. Financial support was sought for her medical treatment, including chemotherapy, and arrangements were made for Amir’s medical needs.
Education: Support included ensuring Amir’s regular school attendance, providing coaching classes and study materials, and linking him with educational schemes like Bal Sangopan. Efforts were made to involve the child in extracurricular activities to enhance his learning experience.
Household economy: Ration support was provided to the family to alleviate economic burdens. Efforts were made to link the family with schemes like the Pradhan Mantri Bima Yojana for insurance coverage and to facilitate the issuance of essential documents like the ration card and income certificate.
Living conditions: Immediate needs like issuing caste certificates and facilitating access to basic amenities were addressed. Counselling and follow-up sessions were conducted with the caregiver to address issues like alcoholism.
Family 3
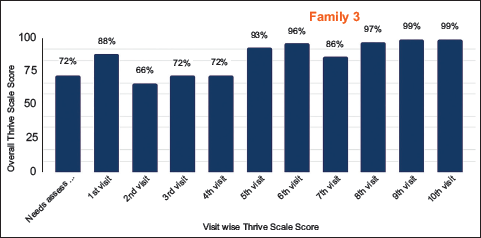
This is the case of Radha, whose parents passed away when she was very young, and her grandmother came forward to care for and support her in the absence of Radha’s mother. Currently, Radha lives with her uncle and aunt (caregivers), their two children and her grandmother. The family faces serious economic problems, with an uncle addicted to alcohol and the responsibility of single parenthood. Socially, the grandmother has good social relationships, having stayed in that village for the last 30 years. She maintains good relations with neighbours and community people. The family has a good bond among themselves, and the caregivers support the child as their own child. The family’s overall thrive score improved from 72 per cent during the baseline to 99 per cent at present due to tailored support, planning and interventions addressing their specific needs.
Family and social relationships: Parenting training sessions were conducted to improve parenting skills and strengthen the bond between family members.
Health and mental health: Awareness programmes were conducted on health insurance (MA card) and hygiene practices. Further counselling was done to address stress management and emotional expression, considering the family’s challenging circumstances.
Education: Efforts were made to ensure the child’s regular attendance at the Anganwadi centre for early childhood education, and further support was provided to prepare linkages with educational schemes and entitlements.
Household economy: The family was linked with the Pradhan Mantri Pragati Yojana (PMPY) and Palak Mata Pita Yojana (Palak Mata Pita Yojana, n.d.) for financial support and got assistance in opening a joint bank account and guidance on managing finances effectively.
Living conditions: Families were linked to the Swachh Bharat campaign to improve living conditions, while interventions like the Pradhan Mantri Awas Yojana (PMAY) scheme addressed housing needs. Further support in providing death certificates and income certificates facilitated access to entitlements.
Family 4
The young girl named Kiran went through massive upheavals after the death of her father. Her mother got married, but her stepfather refused to take care of her. Later, the stepfather died, and at that time, her grandfather, through the support of panchayat members, took Kiran under their custody. Kiran was 3 years old when she started living with her grandparents. The grandparents initially struggled to take care of the small child, but with their determination, they were able to raise the child, providing all possible needs and support to the child. When the family was identified by the project team, their overall thrive score was 67 per cent, and support was required under the domains of health, household economy and living conditions. After successful linkages and support to family, the overall thrive score is 98 per cent.
Family and social relationships: Parenting training sessions were conducted to improve parenting skills and strengthen the bond between family members. Dialogues were held with relatives and neighbours to foster a supportive environment for the child.
Health and mental health: Counselling and issuance of health insurance card (MA card) promoted the child’s physical and mental well-being.
Education: The child was encouraged to participate in the Bal Panchayat to receive moral support from peers and enhance her educational experience.
Household economy: The family was linked with the Mahatma Gandhi National Rural Employment Guarantee Act (MNREGA) for financial support and with Palak Mata Yojana for financial support to cover child’s expenses.
Living conditions: The family was assisted in accessing housing (AWAS) and sanitation (Swachh Bharat) facilities to ensure a safe and hygienic living environment.

Family 5
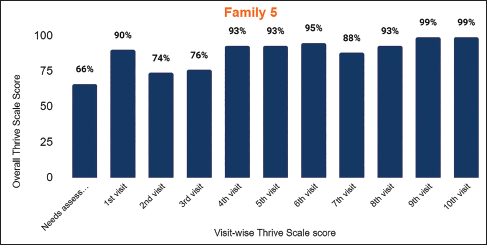
Mahesh, an orphaned child, faced familial disruptions when his mother remarried, leaving him under the care of his grandparents due to his stepfather’s refusal. The family grapples with economic hardship following the demise of their primary breadwinner. Their house is located outside the main village. Mahesh spends much of his time alone, isolated from friends and relatives. Their household lacks basic amenities like electricity and proper sanitation, with Mahesh’s education suffers due to the remote location of his school and a lack of academic engagement. Both the grandparents are addicted to alcohol. The extended family members live nearby, hence providing care and support to the child in the absence of primary caregivers and creating a familial environment. The overall thrive score of the family improved from 66 per cent to 99 per cent in the span of three interventions. The highlights of the support provided are as follows:
Family and social relationships: Parenting training sessions were conducted to improve parenting skills and strengthen the bond between family members.
Health and mental health: Health hygiene counselling sessions were conducted, and the child was enrolled in the MA card scheme for healthcare support. Further counselling sessions were conducted for the grandparents’ alcohol addiction.
Education: The child was engaged in the Bal Panchayat for moral support from peers and also received financial aid.
Household economy: The family was linked with schemes like Madhya Gujarat Vij Company Limited (MGVCL) and Palak Mata Pita Yojana to alleviate financial strain.
Living conditions: Efforts were made to improve sanitation through the Swachh Bharat initiative.
Family 6
Kaveri, a 4-year-old child who lost her parents in an accident in 2023, now lives with her grandparents (caregivers). Her grandparents are deeply concerned about Kaveri’s well-being. Currently, Kaveri does not attend Anganwadi and stays at home. The family is yet to obtain death certificates for the deceased family members, although Kaveri’s name has been added to the ration card. Kaveri was seen as heartbroken and is still struggling to cope with her loss. Whenever someone mentions her parents; name, Kaveri breaks down in tears. Her grandparents, aware of her fragile emotional state, avoid speaking her parents’ names during conversations to shield her from further pain. The current overall thrive score of the family is 89 per cent. The specific support identified for the family is:
Family and social relationships: Counselling for the caregiver to maintain a nurturing environment for her.
Health and mental health: Monitoring and guidance for the grandparents to ensure Kaveri’s physical and emotional health are prioritised.
Education: Though the child does not currently attend Anganwadi, discussions and plans are in place to ensure she receives proper educational support.
Household economy: The family is connected to Palak Mata Pita scheme to alleviate financial pressures and support Kaveri’s upbringing.
Living conditions: To ensure the home environment is safe and conducive to Yashvi’s well-being.
The targeted interventions and support extended to these families indicate tremendous trends and key findings on addressing socio-economic and educational challenges, particularly amidst the COVID-19 backdrop. The average baseline scores for the families ranged between 52 per cent and 72 per cent, pointing to huge battles with health, mental health, education and the household economy. Over time, the said scores increased dramatically, ranging between 74 per cent and 99 per cent, because of the key interventions, which included family and social relationships—improved through training and community involvement, psychosocial support and counselling, continuity in education through material support and schemes and an improved household economy through financial support and documentation.
Notably, the COVID-19 relief measures, including ration support and economic links, have been of critical significance in terms of stabilisation during that period for families.
Findings from Interview with Kinship Caregivers
The focus of this data collection was on the kinship care arrangement for a child, specifying in depth their placement and how the child has been cared for. The child’s age during the time of placement in kinship care and its reasons highlight the thoughts that could have occurred to the caregivers when they took up such a role of primary caregivers. The study also finds out who approached the caregivers to seek help for the child, and how difficult it was to adjust to new conditions, and how they now feel about it.
Child’s age when the child was placed in kinship care arrangement:
In three out of six families, children came into kinship care at a relatively young age. The child in family 1 and the child in family 2 were 1 year old, and the child in family 4 was 1.5 years old. This suggests that infants and toddlers are more likely to be placed in kinship care due to their vulnerability during this age bracket and the immediate need for caregiving by the nearest family member. Furthermore, from the point of view of caregivers, accepting such young children under their care evinces a strong sense of family bonding, but on the other hand, this would also be equally challenging to take care of the development, attachment and adjustment of these young infants and toddlers. Younger placements potentially lead to stronger bonds but also raise challenges associated with early childhood care.
Reason for a child to be placed in kinship care arrangements:
In three out of six families, the reason for the child to come into kinship placement was familial disruptions due to parental death. In the other three families, remarriage by the mother after the father’s death is a common reason for a child to come into kinship care.
Initial feelings and motivations for taking on the responsibility of caring for the child:
Positive feelings:
Strong emotional bonding, family bonding and a sense of responsibility to provide a secure future to the child despite facing financial constraints. Community support: For example, in the case of family 4, the panchayat played an important active role in ensuring the welfare of the child and facilitated kinship care arrangements. Major concerns:
Caregivers were stressed and apprehensive about meeting the child’s needs concerning finances. The caregivers were emotionally disturbed when they lost their wards’ child’s parents in the accident. A complex interplay was visible between the caregivers’ emotional well-being and their ability to provide effective care for the child. In the event of the mother’s remarriage, caregivers were apprehensive about the likelihood of the child experiencing feelings of abandonment and rejection.
The caregiver was approached to take care of the child.
In all cases, it was the grandparents who came forward to take care of the children. No external individuals or agencies approached them. In all cases, a sense of responsibility and commitment to make sure the well-being and stability of the grandchildren were found.
Reasons for accepting the child into their care:
The biggest driving force was the strong sense of family bonding and responsibility towards the child. Each caregiver felt a duty to ensure the child’s well-being and to provide a stable and nurturing environment within the family. All caregivers were emotionally connected with the child, and this strong personal connection drove their decision to take on the caregiving role.
Other people in the household and the type of relationship the child has with other members:
In two families, other people in the household live together with the caregivers and the child. In both families, the child is well accepted by the other members and has good relationships with them. In one family, the child has a strong sibling relationship and love with the biological children of the caregivers. This proves that a responsive and friendly family environment is essential for the child’s life and adjustment to the kinship care arrangements.
Rearing your birth child differs from raising this child:
In five out of six cases, the child’s primary caregivers were grandparents who provide care to the child, and the caregivers are raising the children as if they were their own, not just being grandparents to the child. In one family, the child is being raised by the primary caregiver as if they were their own. The child calls the kinship caregivers (uncle and aunt) as ‘papa’ and ‘maa’ (father and mother). The aspect of raising non-biological children evidences the strong level of responsibility and emotional connection that the caregivers have with all the children under their care.
Support from extended family members or from the community:
In all families, extended members stay next door to the caregivers and children. The support they get from them is mostly regarding time and kind. The extended family members do not support or contribute financially but take care of the child in the absence of a primary caregiver. They create familial environments for the child’s well-being. Caregiving, therefore, is also influenced by the proximity of the extended family and the existence of close-knit family networks. The practical and emotional support extended by the extended family allows the child to be consistently taken care of and feel that they belong to an extended family unit. This further leads to the creation of a community-like atmosphere, fostering a sense of belonging and stability for the child.
Awareness and support of the child’s aspirations:
Four out of five kinship parents are fully aware of their child’s aspirations and dreams. For one family, the child is just 5 years old and does not have any aspirations yet. Here, the caregivers just focus on providing a nurturing and supportive environment until the child develops specific aspirations. It is evident that caregivers are actively engaged in understanding and supporting the aspirations of the children, which shows the caregivers’ deep commitment to the children’s personal development and future success. In one family, the caregiver has enrolled the child in tabla classes, which shows that caregivers are facilitating not only academic and career aspirations but also personal interests and hobbies, contributing to the child’s happiness.
Current difficulties in caring for the child:
The majority of caregivers have highlighted issues concerning the child’s education. Emotional issues are also significant in some instances. Caregivers are also concerned about external influences, especially in cases where the mother has remarried.
Looking for alternative care arrangements:
All caregivers wish for the child to remain with them and do not seek alternative care arrangements, which clearly depict their commitment. One caregiver admits that, ideally, the child would benefit more from living with his mother, indicating awareness of the potential gains of care from the mother despite the current arrangements.
Analysis and Findings from the FGD with Village Child Protection Committee (VCPC) and Ward Child Protection Committee (WCPC) and Community Volunteers
Approximate number of kinship care cases in both communities (Gujarat and Maharashtra):
In the last 3 years, there have been interventions in kinship care arrangements involving 6–7 families across 6 villages. The majority of these families in communities consist of single parents, where the primary caregivers in these kinship care set-ups are often the grandparents (grandmothers or grandfathers). This highlights a significant trend where grandparents are stepping in as primary caregivers.
Nature of interventions provided to families by VCPC and WCPC:
Interventions in Maharashtra by WCPC included addressing documentation [families receive help with preparing and obtaining important documents such as ration cards, identification cards, E-shram cards and ABHA cards (Ayushman Bharat cards)], awareness, linkage to schemes, counselling, health support and education. This holistic approach aims to support both the practical and emotional needs of the families. More focused support and intervention was seen in Gujarat, emphasising the identification of such vulnerable families and children, linking them to schemes, providing mental health support and making decisions in a collaborative manner involving both sides of the family. The VCPC’s active role in child protection is a notable aspect of the support provided. Common interventions: Both states prioritise helping families obtain necessary documents and linking them to government schemes. Counselling and mental support are also crucial components in both regions. It can be also seen leveraging local non-governmental organisations (NGOs) for educational and mental support, highlighting utilisation of resources. In Gujarat, there is a significant focus on considering the child’s preferences and involving extended family members in decision-making, which ensures a child-centric approach to care and protection.
Current role of social worker/CPC/community workers in kinship care cases:
Advocacy and meetings: Both WCPC and VCPC actively advocate for kinship care in meetings and discussions with local committees and government officials. Regular monitoring structure
Challenges faced by VCPC and WCPC members:
In Maharashtra, the absence of essential documents such as ration cards, Aadhar cards and income certificates makes it challenging for the members to create linkages. In spite of support, there is a high risk of child labour in kinship families due to the additional economic burden. Members face challenges in approaching the other relatives of the child for their support and care, as they often show less commitment. Some kinship caregivers live outside the community, and it is difficult to make regular follow-ups and monitoring. In Gujarat, the lack of documents and unawareness of schemes among family members are issues in creating a proper support structure and intervention for the families. Preference based on gender: Male children are typically taken by the paternal side, while female children are taken by the maternal side, often due to inheritance issues related to land property. VCPC members sometimes have to spend their own money to support families, which can be financially burdensome, and sometimes they face hostility, such as having doors slammed in their faces or being insulted during follow-ups and visits.
Relevant schemes available in the community and challenges faced to create linkages:
In Maharashtra, two major schemes were known: The Bal Sangopan Scheme and the PPF. Challenges in implementation: Lack of necessary documents. Reluctance to share documents due to trust issues or fear of corruption. Time-consuming processes: These discourage families from prioritising kinship care processes over their daily wage work. Economic burden: Families are concerned about the potential loss of a day’s wage and the need to pay bribes to officials to expedite the process, which they can ill afford. In Gujarat, several schemes were known: Palak Mata Pita Scheme PMAY Pandit Deen Dayal Yojana Old Age Pension Widow Pension NGO Livelihood Support Tie-ups Ayushman Bharat Atal Pension Yojana Sant Soordas Scheme (for disability) Saraswati Sadhan Sahay (provides cycles to girl children for school) Kisan Yojana Antyodaya Anna Yojana Sukanya Samriddhi Yojana Challenges in implementation: Non-availability of important documents (essential documents like death certificates, birth certificates, remarriage certificates, Aadhar cards and PAN cards) are often missing, which hinders the linkage process. Applications require both time and money, which families may not be able to afford. The process can also be delayed due to families’ financial constraints and the requirement to attend to their immediate economic needs. Discouragement from other family members. Delayed visits and approvals by the District Child Protection Committee (DCPC) slow down the process of linking families to the schemes. Opening a bank account for the child linked with a guardian is a lengthy and complex process, further delaying access to benefits.
Challenges faced by caregivers in kinship arrangements:
Kinship families sometimes fail to allocate sufficient time to the child, which leads to a lack of emotional bonding and connection between the child and the family.
When there are biological children in the families of kinship caregivers, then in such cases, prioritising the needs of biological children over those of the kinship care child is expected.
If the family relationship and bonding are not strong, then in that case, children in kinship care arrangements may feel like an added burden to the family. Such children experience a lack of freedom in expressing themselves.
Economic and financial constraints make it challenging for caregivers to provide adequately for the child’s needs.
Caregivers often lack motivation or awareness to seek support from government schemes.
The nature of support needed for positive outcomes in kinship care arrangements:
Continuous emotional and psychological support for both the children and caregivers to ensure a healthy emotional connection and to address any mental health issues. Provision of financial assistance to help meet the basic needs of the child and to reduce the economic burden on caregivers. Consistent monitoring and follow-up visits by social workers and community volunteers to ensure the child’s well-being and proper care. Ensuring that caregivers have the support needed to provide a nurturing and supportive environment.
Recommendations
The recommendations that would strengthen the support framework for children and families in kinship arrangements are as set out below:
Plan and implement specialised programmes or early intervention programmes to support infants and toddlers who are placed in kinship care. Offer training programmes for caregivers on effective caregiving practices, child development and accessing government support. Encourage and facilitate the involvement of extended family and community members in caregiving to create a supportive network for the child and the primary caregivers. Focus on a child-centric approach. Understand the child’s preferences and aspirations, and encourage caregivers to support the child’s interests and dreams, including non-academic pursuits like music or sports. Extended family members play a prime role and should be considered as important stakeholders while working with primary caregivers, so as to ensure a broader family support system for the child. Where possible, involve both sides of the family (paternal and maternal side) and consider the child’s preferences in care decisions to create a more inclusive and supportive environment. Organise regular meetings and forums for kinship care parents, facilitated by NGOs and local government stakeholders, to share experiences, challenges and best practices. Ensure that both children and caregivers have access to regular counselling services to address emotional and psychological needs. Incorporate counselling on the importance of education, health and holistic development as part of the support provided to kinship care families. Streamline the process of obtaining important documents for families so that there is no delay in linkages to schemes. Strengthen the process in the community for the identification of vulnerable families and link them to appropriate government schemes such as Palak Mata Pita Yojana, Ayushman Bharat and Atal Pension Yojana. Enhance the capacity of VCPC members and community workers to assist families in procuring necessary documents and navigating application processes. Empower local bodies such as VCPC, Bal Panchayat and PRI members to take an active role in supporting kinship care families. Gender-inclusive policies and schemes: Extend the applicability of the Palak Mata Pita (PMP) scheme to include single fathers and single mothers who do not remarry, ensuring they receive the same financial and social support as other caregivers, irrespective of their marital status. Regular and systematic monitoring of kinship care families by local child protection stakeholders such as WCPC members, social workers and Anganwadi workers is necessary to ensure the well-being of the children.
Conclusion
The present study gives a nuanced understanding of the challenges and resilience inherent in kinship care arrangements across various regions of India. Caregivers, most of whom are grandparents, have showcased unwavering commitment despite significant financial and emotional hurdles. The targeted interventions and support systems have given positive results, which can be witnessed by the increase in Thrive Scale™ scores. The active role played by the village and ward-level child protection committees in offering comprehensive support underscores the importance of a collaborative approach towards addressing the needs of kinship families and children under kinship care. The study calls for gender-inclusive policies, streamlining procedures to obtain basic identity documents and continuous support for caregivers and children—emotional and financial. Using a child-centric approach and involving extended family and community, this study argues for a holistic strategy to improve the well-being and stability of children in kinship care so that they are raised in nurturing and supportive environments by kinship caregivers.
Annexure A

Annexure B
Questionnaire for FGD with VCPC
How many cases of kinship care arrangements have the social worker/CPC/community workers intervened in (in the last 3 years)?
What has the nature of the intervention been?
a. What is the current role of social worker/CPC/community workers in cases of kinship care?
b. What do you envision is the role of CWC and DCPU in strengthening kinship care?
What are the challenges that social worker/CPC/community workers face in cases of kinship care?
Are the children and families linked to any schemes/services? Please mention the names of the schemes. What are the challenges in the implementation of the scheme?
What are some challenges faced by children and caregivers in kinship care arrangement?
What is the nature of support children and caregivers need for children to have a positive outcome in kinship care arrangement? Who are the other stakeholders who can play an important role in this?
What are the policy recommendations that you would suggest for children to have positive outcomes in kinship care arrangements?
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.