
Abstract
Background
Gene polymorphisms can lead to differential production of inflammatory proteins associated with cancer development. Prior explorations of the association of single nucleotide polymorphisms (SNPs) of monocyte chemoattractant protein (MCP-1/CCL2) and its receptor, CCR2, to bladder cancer, yielded conflicting findings.
Objective
To analyze the distributions of the polymorphisms CCL2 rs1024611 and CCR2 rs1799864 between healthy controls and bladder cancer patients to determine if they are associated with bladder cancer risk in a cohort of Hispanic White and non-Hispanic White men.
Methods
DNA was isolated from blood obtained from healthy male controls (CCL2 n = 447; CCR2 n = 612) and from male bladder cancer patients (CCL2 n = 233; CCR2 n = 227). The CCL2 rs1024611 SNP and CCR2 rs1799864 SNP were genotyped using the TaqMan methodology. Multivariable logistic regression was used to determine associations between SNP genotypes and bladder cancer in Hispanic and non-Hispanic White men.
Results
There were no significant differences in the genotype frequencies for either the CCL2 or CCR2 SNP and bladder cancer risk was equivalent regardless of CCL2 (NHW AA vs AG/GG, p = 0.7232; H AA vs. AG/GG, p = 0.5187) or CCR2 genotype (NHW AA vs GG/GG, p = 0.6826; H GG vs. AA/AG, p = 0.2425).
Conclusion
Prior studies have shown conflicting results regarding the association between bladder cancer risk and the CCL2 rs1024611 and CCR2 rs1799864 polymorphisms. We were unable to validate significant findings regarding any relationship between these polymorphism distributions across individuals with or without bladder cancer in a cohort of non-Hispanic White and Hispanic White men, suggesting no role of CCL2/CCR2 polymorphisms in bladder cancer.
Introduction
Bladder cancer is the sixth most common cancer in the U.S. with more than 83,000 estimated new cases nationally in 2024. 1 It is four-times more likely to occur in men than women, 2 and typically affects individuals of older age, as more than 90% of cases are in individuals over the age of 55. 3 There are differences according to ancestry as the highest incidence of bladder cancer is observed in non-Hispanic Whites, followed by Black and Hispanic patients. 4
C-C motif chemokine ligand 2 (CCL2), also called monocyte chemoattractant protein 1 (MCP-1), and its receptor, C-C motif chemokine receptor 2 (CCR2), are inflammatory chemokines which are known to have several pro-malignant qualities. Physiologically, the CCL2/CCR2 axis regulates the infiltration of T-lymphocytes, monocytes, basophils, and natural killer cells to areas of active inflammation. 5 It also promotes pathological angiogenesis, recruits inhibitory immune cells, and upregulates tumor cell proliferation. 6 In light of these effects, the role of the CCL2/CCR2 axis has been explored in several types of cancer. In clear cell renal carcinoma, increased expression of CCL2 promoted tumor growth, angiogenesis, and macrophage infiltration. 7 In the setting of prostate cancer, serum levels of CCL2 were found to be significantly higher in men with cancer than in their healthy counterparts. 8
CCR2 is a transmembrane receptor protein to which CCL2 preferentially binds. CCR2 assists in immune cell infiltration and trafficking through its interactions with CCL2 and other chemokines. 9 The CCR2 rs1799864 single nucleotide polymorphism (SNP) is a position 64 substitution of adenine (A) for guanine (G), corresponding to isoleucine rather than valine (V64I), which has been shown to increase its half-life and subsequent levels of expression. 10 A population of 7808 Latin Americans of predominantly Native American and European ancestry had a higher prevalence of the rs1799864 A allele when compared to a population of 247,794 Europeans (22.1% vs. 9.2%) in studies pulled from the Allele Frequency Aggregator of the National Center for Biotechnology Information. 11 Previously, the rs1799864 AA genotype has been correlated with a 5.9-fold increased risk for developing bladder cancer in a population of Turkish patients. 12
The CCL2 promoter SNP variant rs1024611 (G2518A) has been analyzed for its involvement in bladder cancer as well. CCL2 rs1024611 has codominant inheritance with three distinct phenotypes. In response to inflammation, individuals with the G allele had increased levels of CCL2 present in serum. 13 Physiologically, subjects with the AA genotype produce the least amount of CCL2, followed by AG and then GG genotypes. 14 Healthy Mexican individuals had a higher frequency of the G allele (47%) when compared to healthy Caucasians (29%) and a prior study performed using a population of 47 bladder cancer cases and 126 controls from Mexico City, Mexico found that there was a significant decrease in the frequency of the G allele and the GG genotype in Hispanic White patients with bladder cancer.15,16 Those included in this study were all of Mexican Mestizo ancestry. Another study conducted in Turkey found that the rs1024611 GG genotype was associated with a 3-fold greater risk of developing bladder cancer using 72 cases and 76 controls. 12 Cases in this study were acquired from patients referred to a Turkish hospital and controls were random volunteers in the local area.
Considering these conflicting results performed in populations of people with different ancestry, we assessed a Hispanic and non-Hispanic White population from South Texas to evaluate the possible associations between the CCL2/CCR2 rs1024611 and rs1799864 SNP genotypes and bladder cancer risk across ethnicity.
Materials and methods
All specimens were gathered with consent under an approved IRB approved protocol for a biorepository. The control cohort was part of the SABOR (The San Antonio center of Biomarkers of Risk for prostate cancer, IRB# HSC20000030H), study, designed to identify markers of risk for prostate cancer and consisting only of males. Cases were obtained from a bladder cancer repository under IRB# HSC20120159H. Both sources are localized to the South Texas area where non-Hispanic White and Hispanic are the predominant population ethnicities. There was inadequate volume of cases of other ethnicities, such as non-Hispanic Black or Asian, in the bladder cancer repository to perform an analysis in these groups
DNA was isolated from whole blood obtained from the SABOR cohort of non-Hispanic White and Hispanic White healthy men (CCL2 n = 447, 165 Hispanic and 282 Non-Hispanic Whites; CCR2 n = 612, 152 Hispanic and 460 Non-Hispanic Whites) using the Qiagen QIAamp DNA Maxi kit. DNA was isolated from peripheral blood mononuclear cells obtained from a cohort of non-Hispanic White and Hispanic White male bladder cancer patients (CCL2 n = 233, 56 Hispanic and 177 Non-Hispanic Whites; CCR2 n = 227, 56 Hispanic and 171 Non-Hispanic Whites) with stages ranging from Ta to T4 bladder cancer (TIS (n = 23), TA (n = 74), T1 (n = 52), T2 (n = 46), T3 (n = 21), and T4 (n = 5) with 12 unknown stages) using the Qiagen DNeasy Blood and Tissue DNA kit. The CCL2 promoter SNP rs1024611 and the CCR2-V641 missense mutation SNP rs1799864 were genotyped using the TaqMan Allelic Discrimination method (ThermoFisher) according to manufacturer instructions. Briefly, 10 nanograms of DNA were PCR amplified with the TaqMan assay mixes in 96 well plates and genotypes were determined using a BioRad CFX96 Touch Real Time PCR System.
Multivariable logistic regression, controlling for age and smoking, was used to examine the association of genotypes with cancer with examination in Hispanic and non-Hispanic White men. Fisher exact tests with calculated odds ratio (OR) and 95% confidence interval (95% CI) were used to analyze 2 × 2 contingency tables for allelic distributions and chi-squared tests were similarly used to assess variations in genotype distributions between non-Hispanic White and Hispanic White controls. Meta analysis was performed by pooling case and control volumes from the prior studies of Mexico City 16 and Turkey 12 with our own cohorts and using Fisher exact tests to evaluate the impact of AA or GG homozygosity on the risk of developing bladder cancer.
Results
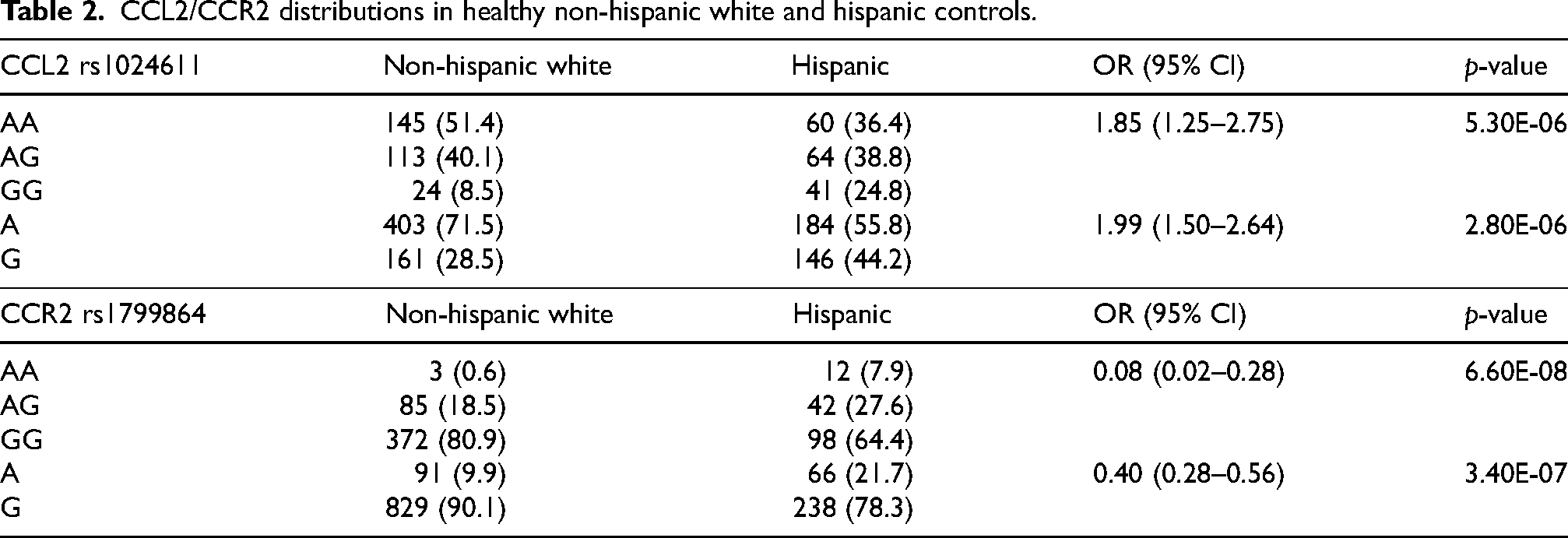
Population demographics are presented in Table 1. In the control populations (Table 2), the Hispanic White cohort compared to the non-Hispanic White cohort showed a higher frequency of the G allele (44.2% vs. 28.5%, OR (95% CI) = 1.99 (1.50–2.64), p = 2.80E-6) with a lower frequency of the AA genotype (36.4% vs. 51.4%, OR (95%) = 1.85 (1.25–2.75), p = 5.3E-6) at the CCL2 rs1024611 locus. For CCR2 rs1799864, there was a significantly higher frequency of the A allele in the Hispanic White controls when compared to non-Hispanic Whites (21.7% vs. 9.9%, OR (95% CI) = 0.40 (0.28–0.56), p = 3.40E-7), with a subsequent increase in AA frequency (7.9% vs. 0.6%, OR (95% CI) = 0.08 (0.02–0.28), p = 6.6E-8).
Population demographics.
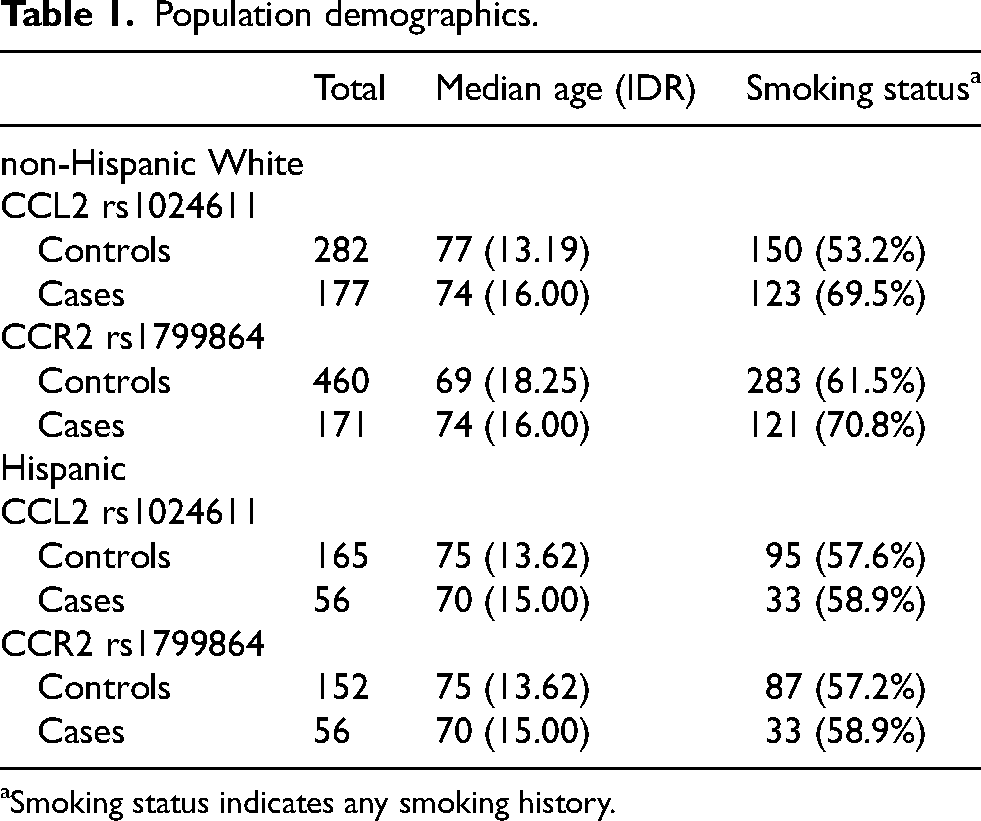
Smoking status indicates any smoking history.
CCL2/CCR2 distributions in healthy non-hispanic white and hispanic controls.
When comparing healthy controls to bladder cancer patients in the non-Hispanic White cohort, there was no significant difference in the allele or genotype frequencies for either the CCL2 rs1024611 or CCR2 rs1799864 locus (Table 3). Additionally, there were no significant differences in the allele and genotype frequencies when comparing the controls and bladder cancer patients in the Hispanic White cohort at either the CCL2 rs1024611 or CCR2 rs1799864 SNPs (Table 4).
Multivariate regression comparing genotypes for CCL2 rs1024611 and CCR2 rs1799864 between cases and controls.
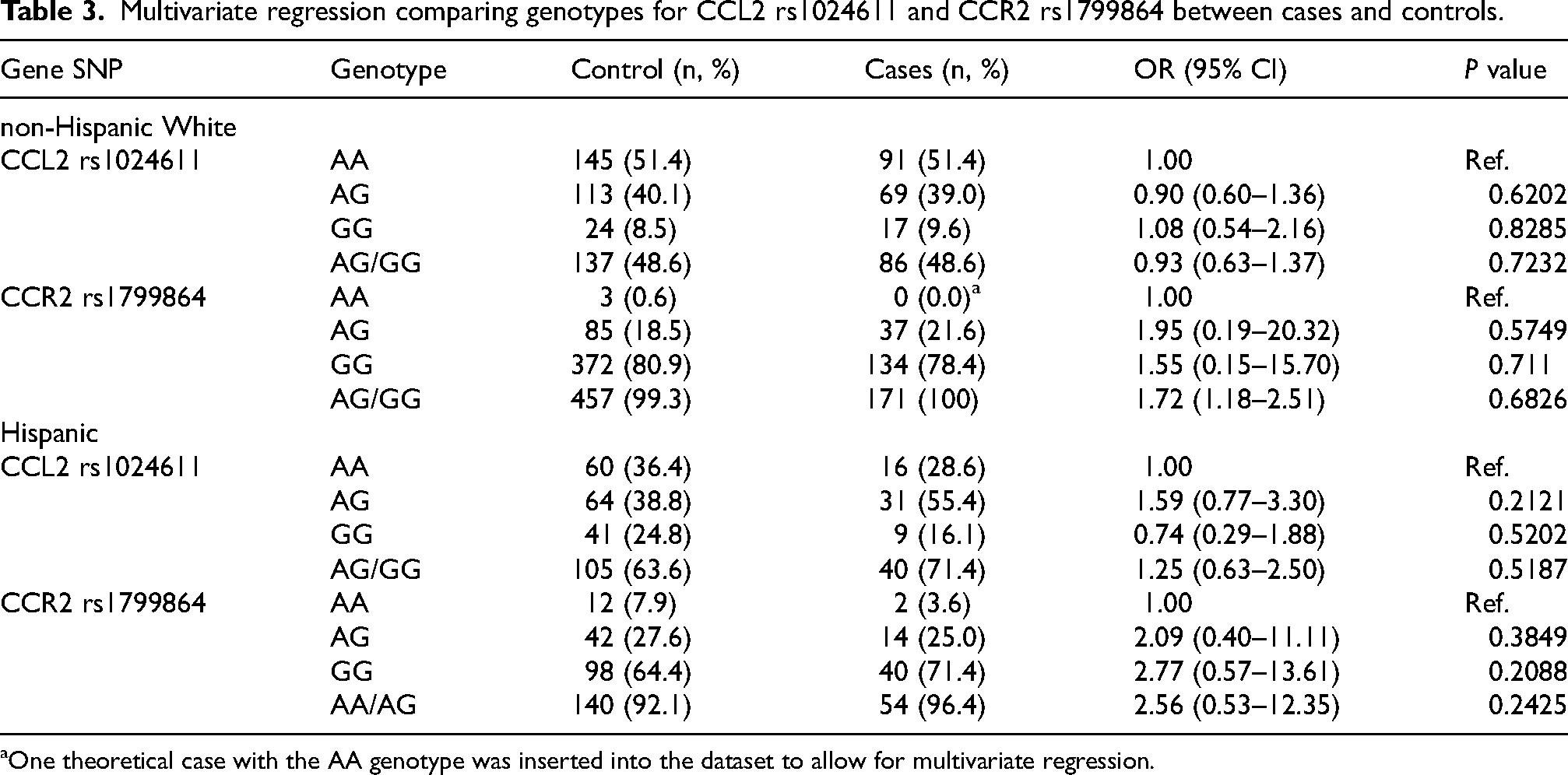
One theoretical case with the AA genotype was inserted into the dataset to allow for multivariate regression.
Meta analysis for CCL2 rs1024611 and CCR2 rs1799864 genotype distributions among bladder cancer cases and healthy controls.
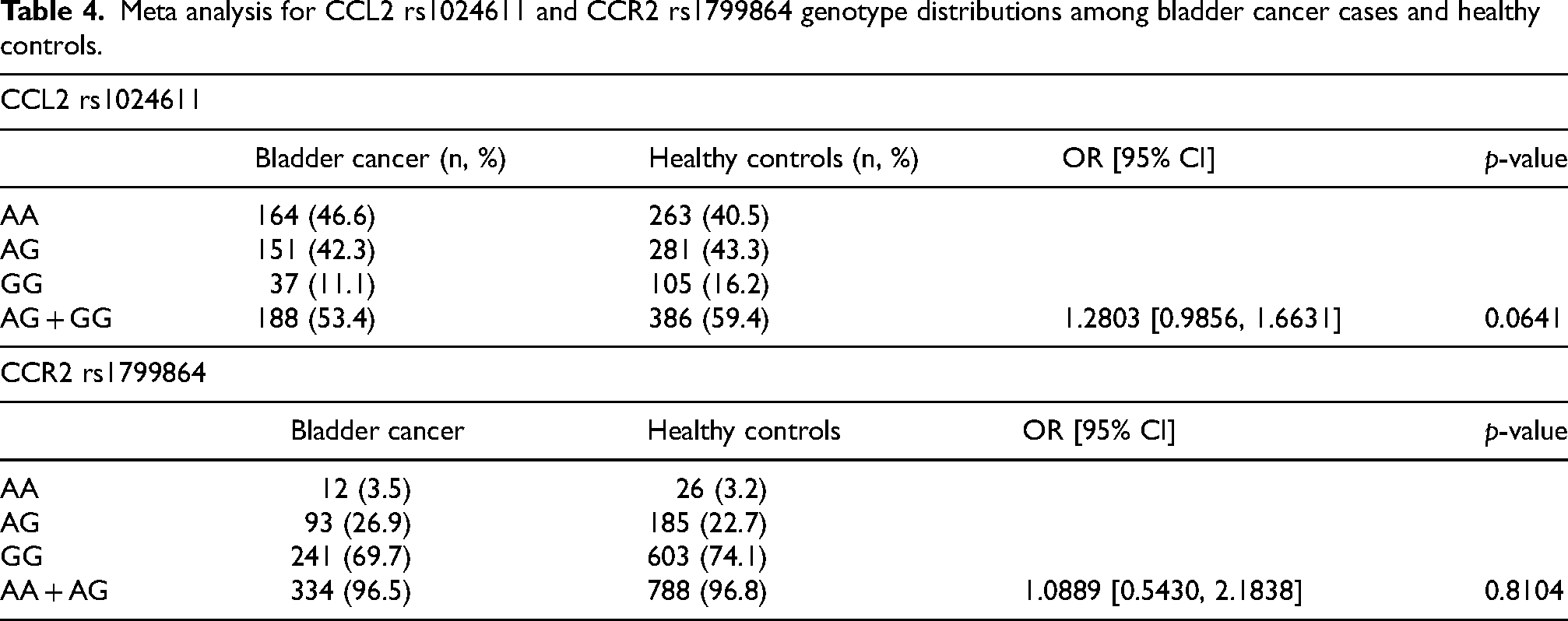
Meta analysis combining the volume of cases and controls from two prior studies showed no significant impact when comparing the AA genotype to AG + GG for CCL2 rs1024611 (OR (95% CI): 1.28 (0.99–1.66, p = 0.0641) or the GG genotype to AA + AG for CCR2 rs1799864 (OR (95%CI): 1.09 (0.54–2.18), p = 0.8104.
Discussion
Prior studies reported on the association between the genetic variants in the genes CCL2 and CCR2 and the risk of developing bladder cancer. These studies were performed in populations with different ancestry and showed conflicting results. First, a study based on a cohort from Mexico City, Mexico found an association between the G allele of CCL2 rs1024611 and a decrease in risk of bladder cancer. 16 A subsequent study from Turkey found that the rs1024611 GG genotype frequency was significantly higher in bladder cancer patients compared to controls, a finding which conflicted with that of the Mexico City population. 12 The authors from the study in Turkey also demonstrated that there was an association between the CCR2 rs1799864 polymorphism and bladder cancer risk, and the AA genotype was associated with an increased risk of developing malignancy. 12 These conflicting findings demonstrate that more work is needed in this area to understand the association of this polymorphism with risk of developing bladder cancer.
A difference in genotypic frequencies for the CCL2 rs1024611 polymorphism has been previously reported in Hispanic White subjects compared to non-Hispanic Whites. Our control population confirmed these findings, as the G allele was the most abundant allele in the Hispanic population, while in non-Hispanic whites the A allele was the predominant one. 15 Similarly, the control population had findings consistent with the known distribution of the CCR2 rs1799864 polymorphism by ancestry. Healthy Hispanic White controls showed an increased incidence of the A allele compared to the non-Hispanic White controls.
Compared to the findings of two other studies evaluating CCL2/CCR2, our data revealed no significant correlation between any specific CCL2 or CCR2 genotype and presence of bladder cancer. The distribution of genotypes of the control population closely resembled that of the bladder cancer patients and furthermore yielded no statistical significance when accounting for age and smoking. Further, after evaluation with meta-analysis of the aforementioned studies, there still lacked any significant relationship between CCL2 or CCR2 and the risk of bladder cancer. With the knowledge that both variants we studied have been associated with increased serum levels of the respective chemokine, this study suggests that modifications to the CCL2/CCR2 inflammatory response had no effect on the risk for developing bladder cancer in our population.
Though our study offers an analysis with adequate statistical power on a larger cohort of both Hispanic and non-Hispanic White bladder cancer patients, it is not without its limitations. Due to significant differences in the genotype distributions of CCL2/CCR2 across ethnicity, there are likely variations in local populations. This may exhibit significant influence on direct comparisons between differing geographical regions. Thus, while we did not find any significant association between CCL2/CCR2 and the risk of developing bladder cancer, we cannot definitively compare any results between two geographical areas. There is also a possibility of additional polymorphisms in the CCL2/CCR2 coding or regulatory regions which have a confounding influence on chemokine function. Other variants, such as CCL2 A2076T, have been recognized, though this polymorphism did not show any altered production of CCL2 when prompted to enact an inflammatory response. 15 When considering variable acquisition, our method for classifying an individual as Hispanic or non-Hispanic White was based on self-reporting and our Hispanic White bladder cancer patient sample sizes (n = 56 for both CCL2 and CCR2) would have greater statistical power with increased patient recruitment. Both characteristics could contribute to potential inconsistency and statistical limitation in our study.
There are ways our study differs from that completed in Mexico City and Turkey which could have contributed to differing results. Regarding methodology, we genotyped our biological specimens using the TaqMan methodology while both the study from Mexico City and from Turkey utilized genotyping accomplished by digestion of the DNA with the restriction enzyme, PvuII (Invitrogen). Further, our cohort consists entirely of male patients which presents an intrinsic difference in our dataset as prior studies were performed on a mixed cohort of men and women, though they were predominantly male. The CCL2 rs1024611 SNP has been suggested as being phenotypically different between genders, so the exclusion of female patients should be considered as a confounding factor between this study and those before it. 17 Beyond men having a three to four times higher risk of developing bladder cancer, many clinical parameters differ between men and women with bladder cancer, such as stage at diagnosis, mortality, and tumor invasiveness, and including women in this study could have had a significant impact on the results.14,18 However, excluding women from our cohort may have created a more specific analysis of the impact of CCL2 and CCR2 on bladder cancer incidence since we are removing a potentially unmatched variable between cases and controls. Considering these differences, our study does not refute any prior investigations but rather contributes further to the discussion of the role of CCL2 and CCR2 in the risk of developing bladder cancer.
Even though our data did not show that variants in CCL2 and CCR2 are associated with bladder cancer risk, it may be beneficial to evaluate the effects of these chemokines on aspects of bladder cancer treatment, specifically the use of immunotherapy. BCG (Bacillus Calmette-Guerin) is an intravesicular therapeutic option for non-muscle invasive bladder cancer. Treatments rely on the patient's innate immune response to destroy neoplastic cells; thus, variations in one's immune system could have drastic downstream implications for treatment efficacy. In a small sample size from an earlier study, every patient with the CCL2 rs1024611 GG genotype, which correlates with increased serum levels of CCL2, showed responsiveness to BCG treatment, 16 suggesting that the capability to mount a robust chemokine response is crucial in patients receiving BCG. Evaluating the frequency of these CCL2/CCR2 SNPs in a statistically large population of BCG-responsive and -unresponsive patients could give insight into any prognostic capabilities of the CCL2/CCR2 axis. This potential study would be limited by similar factors mentioned above: ancestral differences in CCL2/CCR2 frequencies, confounding chemokine polymorphisms, and recruiting adequate statistical power as the AA genotype of CCR2 is rare amongst non-Hispanic whites.
Conclusion
CCL2 and CCR2 have been studied extensively for their role in cancer development and several studies have assessed the association between the CCL2 rs1024611 and CCR2 rs1799864 SNPs and bladder cancer risk. However, these studies have yielded conflicting results. An analysis exploring the differences in genotype distributions between healthy non-Hispanic and Hispanic White men was conducted, and between non-Hispanic White men with and without bladder cancer and Hispanic White men with and without bladder cancer. Hispanic White men had a higher frequency of the CCL2 rs1024611 G allele and the CCR2 rs1799864 A allele compared to non-Hispanic White men, which is consistent with prior studies. Hispanic Whites also had a higher frequency of CCL2 GG and CCR2 AA genotypes than non-Hispanic Whites. When comparing patients with and without bladder cancer, there were no significant differences in genotype or allele distributions in either Hispanic or non-Hispanic White men when controlling for age and smoking.
Footnotes
Acknowledgements
Genotype data was gathered with support from the University of Texas Health Science Center Biospecimen and Translational Core Laboratory.
Ethical considerations
All specimens were gathered with consent under an approved IRB approved protocol for a biorepository. The control cohort was part of the SABOR (The San Antonio center of Biomarkers of Risk for prostate cancer, IRB# HSC20000030H), study, designed to identify markers of risk for prostate cancer. Cases were obtained from a bladder cancer repository under IRB# HSC20120159H.
Consent to participate
Not Applicable
Consent for publication
Not Applicable
Author contributions
Jackson Harmon – performance of work, interpretation of data, writing the article
Dr Robert Svatek – conception, performance of work, interpretation of data, writing the article
Dr Johnson-Pais – performance of work, interpretation of data, writing the article
Dr Robin Leach – performance of work, interpretation of data, writing the article
Dr Neelam Mukherjee – conception, performance of work
Dr Jonathan Gelfond – performance of work, interpretation of data
Elizabeth Santos – performance of work
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported in part by (1) the Roger L. And Laura D. Zeller Charitable Foundation Chair in Urologic Cancer, (2) the Glenda and Gary Woods Distinguished Chair in GU Oncology, (3) the Ron and Karen Herrmann fund, (4) U01CA086402 from the NCI Early Detection Network, (5) the American Cancer Research Scholar Grant (RSG-23-1148519-01-IBCD), and (6) National Cancer Institute Grant 1R01CA281726-01A1.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Robert Svatek, MD, is an Editorial Board Member of this journal, but was not involved in the peer-review process nor had access to any information regarding its peer-review.
Data availability
The data used for this project will be included alongside manuscript submission. This includes the complete dataset utilized for the analysis of this project, with associated age and CCL2/CCR2 genotypes. There are also added controls for the CCR2 rs1799864 polymorphism for Non-Hispanic White controls to produce adequate statistical power.