
Abstract
Background
Neoadjuvant chemotherapy followed by radical cystectomy (NACT-RC) is the prevailing standard of care for muscle-invasive bladder cancer (MIBC), but trimodality treatment (TMT) using chemoradiation after transurethral resection of bladder tumor (TURBT) is an effective alternative in select patients.
Objective
This study examined patterns of care and impact of social determinants of health on the overall survival (OS) using the National Cancer Database (NCDB).
Methods
Data on patients aged ≥18 years with stage II-IIIA MIBC treated with TMT or NACT-RC during 2014–2021 were analyzed with propensity score matching. Logistic and Cox regression were used to evaluate the association of social determinants of health with patterns of care and OS.
Results
Among 18,072 cases (mean age 68.3 years), 77.1% received NACT-RC. TMT use increased from 18.4% in 2014 to 27.1% in 2021 (p < 0.001). The odds for receiving NACT-RC were higher for patients with stage IIIA (odds ratio (OR) = 1.21, 95% confidence interval (CI) 1.09-1.34). However, older patients (OR 0.86, 95% CI 0.87-0.88), those treated at comprehensive community cancer programs (OR 0.51, 95% CI: 0.46-0.55), or used Medicaid (OR = 0.48, 95% CI 0.39-0.61) had lower odds for receiving NACT-RC. In propensity score matching analysis, NACT-RC was associated with lower mortality compared to TMT (Hazard ratio (HR) = 0.66, 95% CI:0.59-0.73). Medicaid users receiving NACT-RC had the highest mortality risk (HR = 1.47, 95% CI:1.28-1.68, pinteraction=0.001).
Conclusion
TMT for MIBC has increased in recent years. Selection between NACT-RC and TMT was influenced by age, stage, diagnosis year, comorbidities, travel distance, facility, and insurance type, highlighting disparities in MIBC treatment.
Categories
Radiation Oncology, Oncology
Keywords
Introduction
Bladder cancer is the second most common genitourinary malignancy and the ninth most common malignancy worldwide. 1 Radical cystectomy (RC) with neoadjuvant cisplatin-based chemotherapy has been the gold standard treatment for patients with muscle-invasive bladder cancer (MIBC) with modern series demonstrating 5-year overall survival (OS) rates from 55% to 65%.2–5 Unfortunately, complications following RC increase morbidity and mortality as over 20–30% of patients experience grade 3–5 complications, which can result in substantial negative impacts on patients’ quality of life (QOL) and underscores the necessity of establishing alternative treatment methods.6,7
Advancements in oncologic treatment strategies over the last few decades have led to the rising adoption of organ-preservation approaches throughout various disease sites including head and neck cancer, anal cancer, as well as MIBC. Moreover, the significant morbidity and mortality risks associated with RC have propelled growing interest in the development of bladder preservation strategies, which utilize maximal transurethral resection of bladder tumor (TURBT) followed by radiation treatment (RT) with concurrent radio-sensitizing chemotherapy, often referred to as trimodality treatment (TMT).
While no randomized trials have directly compared neoadjuvant chemotherapy followed by radical cystectomy (NACT-RC) with TMT, several observational studies suggest that TMT offers comparable oncologic outcomes and improved QOL for carefully selected patients with MIBC.8–17 TMT is a suitable option for elderly or surgically ineligible patients.12,13 The most favorable outcomes were observed in patients with single, early-stage tumors that could be completely removed with TURBT. 11 Another review highlighted that TMT achieves excellent 5-year overall survival rates, regardless of whether treatment is administered continuously or in split doses. 14 Therefore, TMT might provide patients with a promising chance at long-term survival with a functionally intact bladder. 18 Since 2022, the National Comprehensive Cancer Network has endorsed TMT as a category 1 recommendation for select patients. 19 The purpose of this study is to gain a deeper understanding of patterns of care related to MIBC, to examine potential health disparities in relation to access to both treatments, and to investigate whether variances in treatment approaches impact the overall survival (OS) outcomes of patients using the extensive dataset provided by the National Cancer Database (NCDB).
Materials and methods
Study design
The NCDB is a joint project of the Commission on Cancer (CoC) of the American College of Surgeons and the American Cancer Society.20,21 The CoC's NCDB and the hospitals participating in the CoC's NCDB are the source of the de-identified data used herein; they are not involved in the statistical validity or data analysis of the present study. The present study is a retrospective study of the NCDB with minimal risk, de-identified data, and no internal or external sources of funding. Patients aged 18 years and older diagnosed with primary transitional or urothelial cell carcinoma of the bladder between 2014 and 2021, who received TMT or NACT-RC for stage II-IIIA bladder cancer were retrospectively analyzed (Figure 1). For those who received TMT, a minimum phase I dose of 4500 Gy was used to exclude palliative radiation cases.

Study design flow chart. National cancer database (NCDB). Gray (Gy).
Measures
The NCDB collects several variables relevant to demographic factors, treatment facility, cancer diagnosis, stage of disease, treatment details, all-cause mortality, and follow-up time. Demographic variables include age at diagnosis, sex, and race/ethnicity. Other variables include socioeconomic status (income, living in a metro area, and primary payer for health insurance), distance traveled to the treatment facility, and a measure of community education. The NCDB defines the community education measure as the percentage of adults aged 25 or older in the patient's zip code who did not graduate from high school. Medicare is a health insurance program in the United States for people age 65 or older or people under age 65 with certain disabilities. Medicaid is a health insurance program in the United States for certain people who have low income including individuals and families, including children, parents, people who are pregnant, elderly people with certain incomes, and people with disabilities. Clinical variables include the year of cancer diagnosis, clinical stage, initial tumor size, type of treatment facility, and the Charlson-Deyo score, which is a weighted score of comorbid conditions.
Radical cystectomy was defined as complete cystectomy or radical cystectomy per methods described in previous literature. 16 TMT was defined as cases that received TURBT, chemotherapy, and radiation therapy. TURBT was defined as having a surgical procedure of the primary site coded as local tumor destruction or local tumor excision per methods described in previous literature. 16 Chemotherapy and radiation therapy must have started after the date documented for TURBT. We included age, sex, clinical stage, initial tumor size, race/ethnicity, income, community education index, health insurance status, Charles-Deyo score, metro/urban/rural area, facility type, travel distance, chemo regimen, radiation fraction, radiation total dose, and modality of initial therapy in the descriptive statistics and evaluated normality for each continuous variable. The primary goal was to identify factors in social determinants of health associated with worse overall survival.
Statistical analysis
For descriptive statistics, Pearson's Chi-square test was used for comparing categorical variables. Mean, standard deviation, and independent t-tests were used for comparing continuous variables with normal distribution. For continuous variables without normal distribution, median, interquartile range (IQR), and Wilcoxon rank-sum test were be used. Logistic regression was used to estimate odds ratios (OR) and 95% confidence intervals (CI) for the association between each baseline characteristic and whether the patient received TMT or NACT-RC. Kaplan-Meier analysis was used to assess differences in overall survival. Cox regression was used to evaluate the risk of mortality. Interaction analysis and propensity matched pair analysis were used to account for baseline differences between those who received NACT-RC vs. TMT. Propensity scores were estimated by computing the probability of receiving or not receiving treatment using a logistic regression model. Variables included in the logistic regression model were age, sex, clinical stage, race/ethnicity, health insurance status, Charlson-Deyo score, metro/urban/rural area, facility type, and travel distance. Patients were matched 1:1 using the nearest-neighbor greedy matching algorithm. Patients were required to be matched exactly the aforementioned variables included in the logistic model. An absolute standardized difference of < 0.2 was used to represent negligible differences in the prevalence or mean distribution of covariates between matched pairs. All statistical analyses were performed using the statistical package Stata (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX, USA: StataCorp LLC.) and SAS software version 9.4 (SAS Institute, Inc., Cary, NC, USA). Statistical significance was defined as a p-value of less than 0.05.
Results
Descriptive statistics
The mean age of the cohort was 68.3 years (SD 9.9), with most patients aged 60–79 years (68.7%). Men comprised 76.3% of the population. For race/ethnicity, 87.3% were non-Hispanic White, 5.6% non-Hispanic Black, and 4.3% Hispanic/Latinx (Table 1). The percentage of patients treated with TMT increased from 18.4% (269/1464) in 2014 to 27.1% (732/2697) in 2021. Most patients lived in metropolitan or urban areas (91.6%). The majority were covered by Medicare (60.6%) or private insurance/managed care (29.8%). Approximately 59.1% of patients traveled less than 30 miles to treatment facilities, while 24.7% traveled more than 30 miles. The clinical stage was predominantly stage II (81.6%). As for comorbidities, 68.3% of patients had a Charlson-Deyo score of 0, indicating no comorbidities.
Baseline characteristics of trimodality treatment vs. neoadjuvant chemotherapy followed by radical cystectomy.

SD: standard deviation.
Percent of adults age 25 or older in the patient's zip code who did not graduate high school.
Χ2 = Pearson's chi squared test.
t = Two-sample t test with unequal variances.
Impact of clinical factors and socioeconomic determinants on treatment decision-making
The choice of definitive treatment significantly depended on many demographic and clinical factors. Patients with the following characteristics: older age, being diagnosed in more recent years, coverage with private insurance/managed care, coverage with Medicaid, Charlson-Deyo score 2 or more, and treatment at a non-academic/research institution were more likely to have been treated with TMT (Figure 2). Since age at diagnosis and year of diagnosis were analyzed as a continuous variable, as the age and year of diagnosis increase, the odds of NACT-RC decreases, making TMT more likely for older patients and diagnosed in recent years. Patients with Stage IIIA or who travel more than 30 miles from home to treatment were significantly more likely to have been treated with NACT-RC.

Plot of odds ratios of factors associated with increased odds of treatment with NACT-RC (OR > 1) compared to TMT (OR < 1). Patients with clinical stage IIIA or traveled more than 30 miles to their treatment facility were more likely to receive NACT-RC. Patients with older age at diagnosis, more recent year of diagnosis, treatment at a community facility, treatment at a comprehensive community, treatment at a integrated network facility, used private/managed care insurance, used Medicaid, or had more comorbidities were more likely to receive TMT. Reference groups: Treatment at Academic/Research programs, Stage II, travel less than 30 miles to a treatment facility, Medicare-user, Charlson Deyo score 0.
Overall survival
Overall survival analysis demonstrated variations in 5-year overall survival rates by insurance status (Figure 3). Patients with Medicare insurance had the lowest unadjusted 5-year survival rate (53%, 95% CI 52-55%), (Table 2). Overall survival trends among different insurance groups differ based on whether they received NACT-RC or TMT. When stratified by treatment group, the Kaplan-Meier curves comparing private insurance, Medicaid, and Medicare display different patterns of overall survival. Although the private insurance group displays better overall survival regardless of treatment group, the Medicare group displays better overall survival than the Medicaid group when treated with NACT-RC at 20–60 months of follow-up while the Medicaid group displays better overall survival than the Medicare group when treated with TMT after 36 months of follow-up (Figure 3). In multivariable cox regression, each additional year of age was associated with a 2% elevated risk for mortality (HR: 1.02, 95% CI: 1.016-1.024) as well as clinical stage IIIA (HR: 1.35, 1.27, 1.44) compared to clinical stage II. There was a significant interaction between insurance and treatment when adjusted for age, race/ethnicity, sex, clinical stage, and insurance status (Table 3, p = 0.001). After propensity score matching (NACT-RC group = 1997, TMT group = 1997, Total sample = 5812), NACT-RC was associated with lower mortality compared to TMT (Hazard ratio (HR): 0.66, 95% CI: 0.59-0.73, p < 0.001).
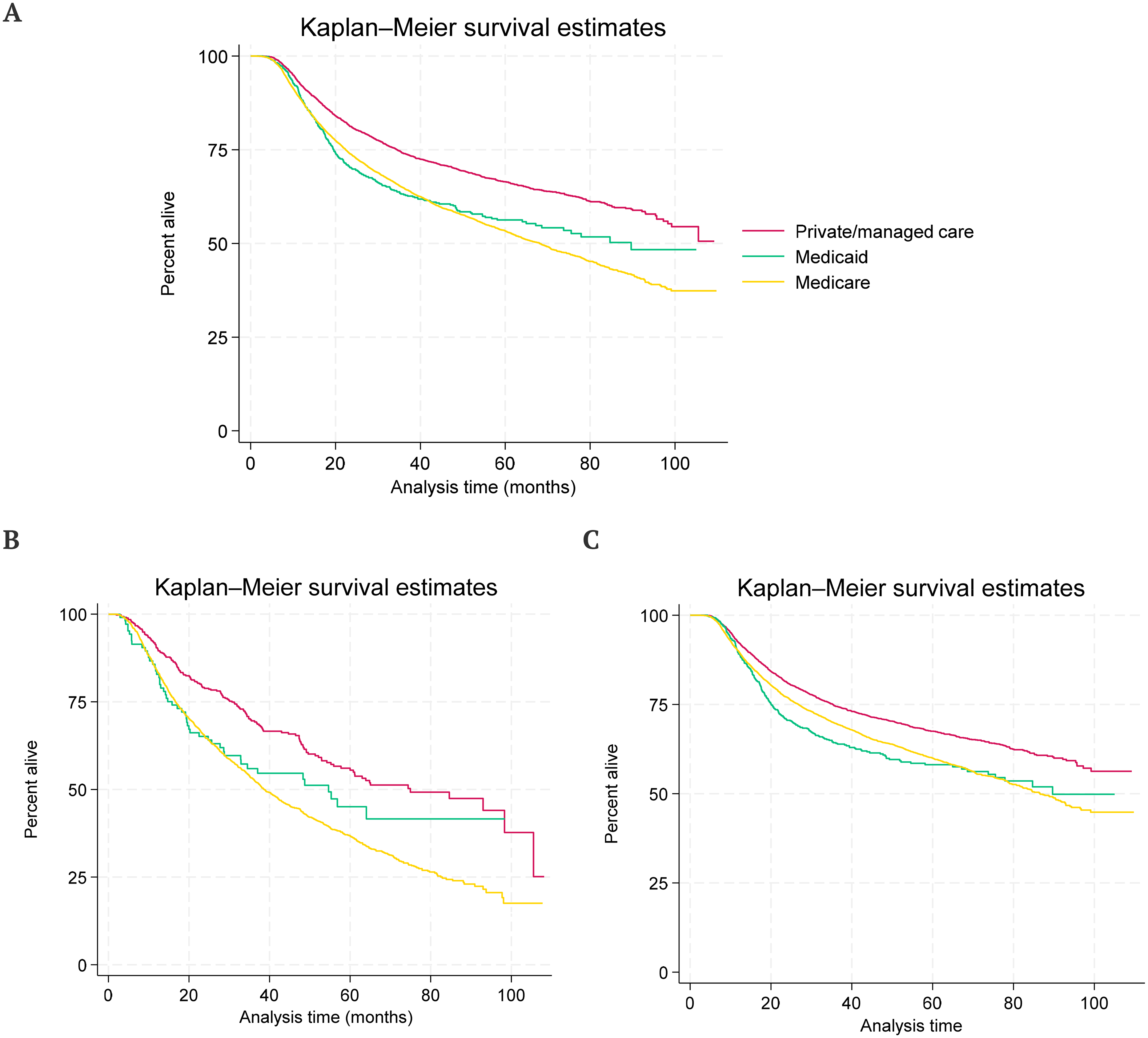
Kaplan-Meier curves of overall survival. A) Overall survival among different insurance groups. B) Overall survival among different insurance groups in TMT only. C) Overall survival among different insurance groups in NACT-RC only.
Overall survival rates at 5 years follow up. Confidence interval (CI).

Interaction analysis. Hazard ratios and 95% CI for comparing the type of insurance on the risk of mortality according to type of treatment (adjusted for age, race/ethnicity, sex, clinical stage, insurance status).

Discussion
This study provides valuable insights into the evolving patterns of care and the social determinants of health factors influencing treatment selection and survival outcomes in patients with MIBC. Our findings reveal significant trends in treatment preferences, as well as persistent disparities that warrant further investigation and targeted interventions.
The increasing adoption of TMT from 18.4% in 2014 to 27.1% in 2021 reflects a growing acceptance of bladder-preserving approaches, consistent with recent guidelines endorsing TMT as a suitable alternative to radical cystectomy for select patients. 22 This trend suggests the potential benefits of TMT, including growing interest in bladder preservation, improved quality of life (QOL), particularly for elderly or surgically ineligible patients. The shift also proposes advancements in multidisciplinary care and greater awareness of patient-centered treatment options among clinicians and patients. In a multi-institutional retrospective cohort study of MIBC cT2-T4N0M0 patients, there was no difference in cancer-specific survival and metastasis-free survival. 9 Although salvage cystectomy after TMT did not affect survival, TMT still had better overall survival than NACT-RC. 9 Despite propensity score matching, unaccounted confounding factors could increase the overall survival in the TMT group. Importantly, this retrospective study involved patients treated at high-volume academic cancer centers whereas our current study includes 53.7% of participants from non-academic treatment facilities. The difference in overall survival could be attributed to heterogeneity of post-treatment follow-up care. In another retrospective pooled analysis of multiple RTOG trials investigating different TMT regimens, a complete response to TMT was significantly associated with improved disease-specific survival and overall survival at five and ten years. 12 Of note, this pooled analysis showed that elderly patients (age ≥ 75) receiving TMT had similar disease-specific survival compared to younger patients. Our study findings reflected these results, which showed older patients were more likely to receive TMT than NACT-RC.
In our study, age emerged as a significant factor in treatment selection, with older patients less likely to undergo NACT-RC. This trend may reflect concerns about surgical morbidity and postoperative complications in this population or a clinical preference for bladder-preserving approaches tailored to their overall health status and QOL. Although the NCDB does not collect QOL metrics, it's important to consider the QOL implications with age. A cross-sectional QOL study of patients previously treated for MIBC revealed that TMT had better general QOL than NACT-RC, considering no differences found in age, gender, comorbidities, and performance status. 7 Although the current study does not focus on QOL, further longitudinal studies are needed to better assess QOL as it relates to a widely variable age range observed in MIBC. Nevertheless, the age disparity found in our study raises questions about potential biases in treatment recommendations related to insurance coverage and disparities in overall survival directly related to healthcare costs.
Our analysis uncovered disparities in treatment selection, not addressed in the previously mentioned retrospective TMT studies. The impact of travel distance further emphasizes disparities in access to specialized care. 50.7% of NACT-RC patients were treated at an academic/research program while 68.6% of TMT patients were treated at a non-academic/research program. Patients who traveled over 30 miles to treatment facilities were more likely to receive NACT-RC, suggesting that proximity to high-volume centers is critical in determining the type of treatment offered. While radical cystectomies are more often done at tertiary care centers, radiation and chemotherapy may be more accessible for patients. However, for those who live far from a treatment center, a one-time surgery may be more convenient than coming for several weeks of chemoradiation. This finding highlights the importance of regional cancer centers and raises concerns about the availability of high-quality care for patients in rural or underserved areas. Ensuring equitable access to these centers is essential to addressing these geographic disparities.
In our study, patients with Medicaid were significantly less likely to receive NACT-RC than those with Medicare insurance. Additionally, patients with Medicaid had better overall survival than those with Medicare on Kaplan-Meier analysis when treated with TMT after 36 months of follow-up. Although this Kaplan Meier analysis does not adjust for age because it cannot account for more than one variable at a time, the Cox regression analysis conducted showed NACT-RC was significantly associated with lower mortality compared to TMT (Hazard ratio (HR): 0.66, 95% CI: 0.59-0.73, p < 0.001) adjusting for age and insurance status. This disparity likely reflects broader systemic issues, including limited access to specialized care, financial barriers, and differences in provider availability across healthcare networks. In a cross-sectional study of people with breast, ovary, endometrium, cervix, colon, lung, or gastric cancer, individuals with Medicaid had a worse overall quality of care compared to those with private insurance. 23 Although this study did not include bladder cancer, the issue of cancer disparities remains a challenge for all types of cancer due to healthcare costs. Such inequities may delay diagnoses or restrict access to comprehensive treatment options, disproportionately affecting economically disadvantaged populations. These findings could partially explain the overall survival differences found in our study, however many confounding factors exist between patients who use Medicaid vs. Medicare and private insurance vs. Medicare. The observed disparities in overall survival based on insurance status are particularly concerning. Patients with Medicaid demonstrated a higher risk of mortality compared to those with Medicare in the NACT-RC group while no significant differences were observed in the TMT group. This disparity shows the critical influence of social determinants of health on cancer outcomes, including access to timely and comprehensive care, quality of follow-up, and support systems during and after treatment. Additionally, this finding may be confounded by baseline comorbidities and performance status between the two groups. Addressing these inequities requires systemic efforts to improve healthcare access, reduce financial barriers, and promote patient education across all socioeconomic groups.
Related to comprehensive multidisciplinary care, the first provider a patient encounters plays a pivotal role in shaping their treatment trajectory, as recommendations often reflect the provider's expertise and familiarity with certain treatment modalities. While this expertise is invaluable, it may inadvertently lead to more conservative recommendations or delayed referrals. In the absence of multidisciplinary discussions, patients may not have the opportunity to fully understand the risks and benefits of all available treatment approaches. This trend emphasizes the importance of ensuring timely referrals to multidisciplinary teams to provide patients with a comprehensive evaluation and access to the full spectrum of evidence-based care options. Strengthening these collaborative efforts is essential to optimizing treatment outcomes and addressing disparities in care.
Together, these findings highlight both progress in treatment strategies for MIBC and the persistent challenges posed by geographic disparities and social determinants of health. Expanding access to specialized care, addressing systemic inequities, and fostering multidisciplinary treatment approaches are essential steps toward ensuring optimal outcomes for all patients. Future research should focus on identifying and mitigating barriers to care, particularly for vulnerable populations, to create a more equitable healthcare system.
This study has notable limitations. Retrospective cohort studies are susceptible to information bias, variability in the quality of data among patients, and limited follow-up data. Information bias in the form of missing data can be challenging when using large databases. As the percentage of missing data increases, results become difficult to interpret. For this study, if the missing/unknown subgroup was greater than 10%, it remained in the statistical analysis as a way to evaluate whether the variable was missing at random. In prospective studies, greater efforts would be made to minimize missing/unknown data and variability in data reporting. Although the NCDB collects massive amounts of data from thousands of patients annually, many patients do not have complete follow-up on overall survival data, contributing to information bias. The NCDB is not systematically linked to the National Death Index, therefore the vital status follow-up variable is not standardized from one data source contributor to another. 24 Another major limitation of the NCDB is lack of recurrence data collection, which would allow investigators to analyze treatment failure as an important primary outcome in cancer treatment research. And although the Charlson-Deyo score is reported by NCDB, other measures of performance status, such as Karnofsky Performance Status (KPS) and Eastern Cooperative Oncology Group (ECOG) Performance Status are widely used to help clinicians evaluate cancer patients. Performance status data would allow investigators to better account for factors that affect overall survival in addition to age and comorbidity burden. Despite these limitations, the NCDB provides valuable information in a well-designed study with strict inclusion and exclusion criteria and thoughtful interpretation of results.
Conclusions
This study sheds light on the dynamic landscape of treatment strategies for MIBC, highlighting both encouraging advancements and persistent disparities that demand attention. The increasing adoption of TMT with complex interactions on overall survival highlights a growing demand for multidisciplinary, patient-centered care, with growing recognition of bladder-preserving approaches as suitable alternatives to radical cystectomy for carefully selected patients. However, the disparities in treatment selection and survival outcomes based on geographic factors and social determinants emphasize the need for targeted interventions.
Efforts to address inequities in access to specialized care, financial barriers, and disparities in provider availability are critical for achieving equitable outcomes. Moreover, a focus on patient education, particularly among vulnerable populations, is essential to ensure informed decision-making and access to comprehensive care. Future research and policy initiatives must prioritize mitigating these barriers while promoting widespread adoption of evidence-based, individualized treatment approaches. By addressing these challenges, the healthcare system can make meaningful changes toward improving the care and survival of patients with MIBC.
Disclosures
Footnotes
Acknowledgments
We would like to thank the National Cancer Database (NCDB) for providing access to the data used in this study. We also acknowledge the support and guidance from the Department of Radiation Oncology at University Medical Center and the Department of Public Health at Texas Tech University Health Sciences Center.
Ethical approval and informed consent statements
This study was deemed exempt from formal IRB review by the Texas Tech University Health Sciences Center Institutional Review Board under 45 CFR 46.104(d). Informed consent was not applicable due to the use of de-identified, retrospective data.
Author contributions
Conceptualization, M.M., Z.S., and D.A.; methodology, M.M., Z.S., and D.A.; formal analysis, M.M. and D.A.; investigation, M.M., Z.S., V.T., A.Z., and D.A..; resources, M.M., Z.S., and D.A.; data cu-ration, M.M. and D.A.; writing—original draft preparation, M.M., Z.S., V.T., D.A. and A.Z.; writing—review and editing, M.M., Z.S., D.A., V.T., A.Z.; visualization, M.M. and Z.S; supervision, Z.S. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data used in this study are available through the National Cancer Database (NCDB) and are accessible only to institutions accredited by the Commission on Cancer of the American College of Surgeons and the American Cancer Society.