
Abstract
Before being marketed in the United States, novel drugs must undergo evaluation for abuse liability. Drugs with higher abuse liability are assigned a schedule associated with stricter regulatory controls. Behavioral economic demand techniques hold great potential for use as an abuse liability assessment in the scheduling of novel drugs. Advantages of demand analyses include (1) quantitative abuse liability results that allow for relative comparisons and ranking among drugs by abuse liability, (2) the ability to collect analogous measures of abuse liability in both preclinical and human clinical models, and (3) minimal extra work to add demand analyses to those analyses that are already recommended in Food and Drug Administration (FDA) guidance. Challenges primarily arise with the standardization of experimental protocols for such assessments, but these challenges may be resolvable with directed work to compare different methodological techniques. If successful, incorporation of these methods could help avoid scheduling errors that are costly to society.
Tweet
Behavioral economic demand techniques could improve drug scheduling classifications by the Drug Enforcement Agency (DEA) and Food and Drug Administration (FDA) and prevent mischaracterizations of abuse liability that can be costly to society.
Key Points
Behavioral economic demand holds great potential for use as an abuse liability assessment in the scheduling of novel drugs by the U.S. government.
Demand analyses allow for quantitative abuse liability results that enable ranking among drugs by abuse liability.
Demand analyses can be conducted with analogous procedures in both preclinical models and human clinical models.
Demand analyses would not require extensive additional work to add to those analyses that are already recommended for the assessment of abuse liability for novel drugs.
Demand analysis procedures could be standardized with directed work to compare different methodological techniques.
Incorporation of demand analyses into scheduling decisions could help avoid scheduling errors that are costly to society.
Executive Summary
The U.S. Food and Drug Administration (FDA) provide recommendations to the U.S. Drug Enforcement Agency (DEA) about the potential for novel drugs to be abused. Drugs with high abuse liability are more likely to be taken in greater amounts than prescribed or by people who do not have a valid prescription for those drugs. For all drugs with approved medical uses and some abuse liability, the DEA assigns a schedule under the Controlled Substances Act in accordance with the level of abuse liability. Drugs with minimal potential for abuse are assigned Schedule V, while drugs with an approved medical use and the highest potential for abuse are assigned Schedule II. Schedule I is reserved for drugs that are illegal and have no approved medical use. The assigned schedule for a drug dictates the control measures associated with accessing that drug, with Schedule II assigned the most stringent access controls (i.e., more tracking across pharmacies and providers, fewer refills allowed, etc.). Drugs assigned to an inappropriate schedule can have serious real-world consequences, as an overly restrictive schedule can create unnecessary barriers to obtaining medically necessary prescription drugs, while an overly lenient schedule can fail to prevent practices such as “doctor shopping” to obtain multiple prescriptions. For example, the initial choice to place medications containing hydrocodone, a synthetic opioid, into Schedule III has been cited as a major contributor to the opioid epidemic that is still destroying communities. Hydrocodone-containing drugs have since been rescheduled by the DEA into Schedule II, but only after many people had already obtained far greater quantities of these medications than intended. The FDA has established guidance for the experiments it requests to evaluate the abuse liability of novel drugs prior to and following release on the marketplace. This guidance is meant to thoroughly assess the safety profile of novel drugs and whether a novel drug has abuse potential, but it cannot always determine the degree of severity of that abuse potential. Abuse liability assessments that can better gauge the precise degree of abuse potential for novel drugs could help the FDA make more informed scheduling recommendations to the DEA, potentially helping to prevent future drug abuse epidemics. In this article, I review an abuse liability procedure called behavioral economic demand, which has the demonstrated ability to quantify and rank drugs based on abuse potential in both human studies and preclinical studies. In addition to determining whether or not a drug has abuse potential, I show here initial evidence that this procedure can rank drugs in terms of their current DEA schedule and known abuse liability. With some additional study, this procedure could be incorporated into the abuse liability assessments recommended by the FDA for novel drugs and thereby improve the accuracy of resulting drug scheduling recommendations. Improved drug scheduling accuracy could improve public health by preventing scheduling errors associated with abuse epidemics or unnecessary access restrictions for life-saving prescription drugs.
The Controlled Substances Act
The Controlled Substances Act replaced drug-specific laws and regulations with a common framework under which all drugs with potential for abuse would be regulated. This act established five schedules in which all current and future drugs with abuse liability would be placed. Drugs with the highest abuse liability and with no approved medical use are classified as Schedule I, and under federal law, are generally not allowed to be used for any recreational or medical purpose. Drugs with an approved medical use are placed in Schedules II through V based on abuse liability, with Schedule II drugs having the highest abuse liability and/or physical dependence potential and Schedule V drugs having the lowest abuse liability and/or dependence potential. The DEA is charged with enforcing schedules and making scheduling decisions, with the FDA recommending a schedule for each new drug. The strictness of regulations controlling drug access and tracking of the use of these drugs corresponds with the schedule. Each time a new drug is authorized by the FDA for use in a medical context, the FDA is responsible for making a recommendation for a specific schedule based on the degree of abuse liability. The DEA can also reschedule drugs if there is evidence that the original schedule was inappropriate, and an existing drug should have more or fewer restrictions on its use.
FDA Abuse Liability Assessment Guidance
The FDA has issued guidance regarding the type of experimental data it requests to facilitate evidence-based scheduling recommendations (Center for Drug Evaluation and Research at the US Food and Drug Administration, 2017). Prior to making scheduling recommendations, it requests preclinical and human clinical abuse liability data, and post-marketing data on illicit use patterns are also collected after a drug is available on the market.
Preclinical evidence consists of receptor binding studies and chemical structure analysis, as well as behavioral pharmacological studies in nonhuman animal models. Recommended behavioral pharmacology experiments include conditioned place preference, drug discrimination, and drug self-administration. Guidance for drug self-administration studies includes specific parameters such as self-administration acquisition on a fixed ratio (FR) 1 schedule of reinforcement, with modest response requirement increases after acquisition to no more than a FR 10. Progressive-ratio schedules (i.e., schedules of reinforcement where the response requirement increases following each drug infusion) are explicitly not requested as evidence.
The design of human clinical abuse liability studies must also adhere to a strict set of parameters to be considered evidence for scheduling recommendations. Human studies should be conducted among recreational drug users to increase the likelihood of detecting abuse liability. Additionally, investigational drugs should be administered double-blind double-dummy to ensure both researchers and participants do not have advance information about which drug is being administered, and investigational drugs should be compared to an active comparison drug with known abuse potential. Evidence for abuse potential primarily consists of subjective ratings by participants on visual analogue scales for “drug liking”. Additional subjective responses for “high” or other characteristics can also be used as secondary measures.
Drug Scheduling Errors and Requirements for Abuse Liability Assessment
The current drug scheduling process has room for improvement. While extensive, the current abuse liability testing protocol is not always able to distinguish fine gradations in abuse liability to align with the four gradations in schedules for drugs with approved medical use. Furthermore, drugs scheduled imprecisely can have drastic consequences. For example, the choice to place hydrocodone-containing medications into Schedule III contributed to the opioid epidemic, as Schedule III allows for prescriptions with multiple drug refills and little tracking of prescriptions and hydrocodone-containing medications were prescribed in very large quantities after their introduction to the market (Habbouche et al., 2018; Jones et al., 2016). Medications containing hydrocodone were rescheduled as Schedule II in 2014, but only after many people obtained much larger quantities of these medications than intended. Drug scheduling criteria that allowed greater precision during the initial abuse liability assessment could help to prevent drug scheduling inaccuracies.
Novel drugs undergoing abuse liability assessment may have a wide range of potencies and mechanisms of action making abuse liability difficult to predict without rigorous assessment. Therefore, common, reproducible procedures are necessary for abuse liability assessment that is appropriate for widely varied drugs with potentially unknown or unpredicted characteristics. For the purposes of this manuscript, an operating assumption will be that new abuse liability assessments for use in drug scheduling recommendations should have utility in providing abuse liability information for drugs with diverse and unknown properties, and maintain that utility with a reproducible set of experimental procedures that could be similarly employed across laboratories and contexts to produce comparable results.
Behavioral Economic Demand
Behavioral economic demand assessments quantify the relationship between the cost of a drug (or nondrug commodity) and consumption of that commodity and are readily assessed in both animal models and human clinical research (Bickel et al., 2014; Hursh & Silberberg, 2008; Koffarnus et al., 2022). The fact that highly similar models and outcome variables can be assessed in human research and nonhuman animal models is a characteristic of demand analyses that could be especially beneficial for making scheduling recommendations, as this would provide a direct link between abuse liability assessments conducted in the preclinical and clinical research phases of assessment. Typically, demand assessments quantify consumption over a wide range of costs. Consumption at minimal cost (also known as demand intensity) has been shown to correspond with measures of the quantity of drug used recreationally and severity of substance use disorder symptomology (Strickland et al., 2020), but is less useful as a metric to compare abuse liability across drugs as this outcome variable is in the unit (i.e., mg) of drug. Therefore, drugs with differing potencies can have vastly different demand intensities without reflecting different abuse liabilities. For an example of this from previous research (Koffarnus et al., 2012), mean demand intensity for the Schedule II synthetic opioid remifentanil was 0.015 mg/kg, while for the Schedule IV barbiturate methohexital it was 9.76 mg/kg. This difference reflects a vast difference in potency between these two drugs, not a difference in abuse liability.
Perhaps more relevant to scheduling decisions, however, is demand elasticity, or the rate of reduction in use as cost increases. Demand elasticity has been shown to be a robust measure of abuse liability that can quantify relative abuse liability across drug classes in both animal and human studies (Hursh & Winger, 1995; Ko et al., 2002; Koffarnus et al., 2012; Strickland et al., 2020). For example, Koffarnus et al. (2012) describes a preclinical self-administration experiment with multiple drugs with different mechanisms of action to determine if demand elasticity would correspond to known differences in abuse liability among the drugs (Koffarnus et al., 2012). Drugs assessed were the fast-acting opioid remifentanil, the psychostimulant cocaine, the barbiturate methohexital, the dissociative ketamine, and ethanol. In addition to identifying each of these drugs as having abuse liability compared to control injections of saline, demand elasticity assessment was able to order the drugs along the spectrum of abuse liability similar to that determined by the FDA and DEA in their scheduling decisions (Figure 1). Results show that cocaine (Schedule II) and remifentanil (Schedule II) were similar to each other in abuse potential and were higher than all other drugs assessed. Ketamine (Schedule III) and methohexital (Schedule IV) were similar to each other and intermediate in abuse liability. Ethanol (unscheduled) ranked lower than all other active drugs of abuse. Furthermore, a saline control condition was ranked well below all active drugs of abuse, allowing for a clear determination of any abuse liability for each while simultaneously ordering the drugs by abuse liability. These relationships were revealed with the relatively small sample size of n = 10. Similarly, other research has shown that demand elasticity measurement can order three opioids by duration of action, a known contributor to abuse liability (Ko et al., 2002), demonstrating that demand elasticity can also differentiate drugs within a similar mechanism of action.
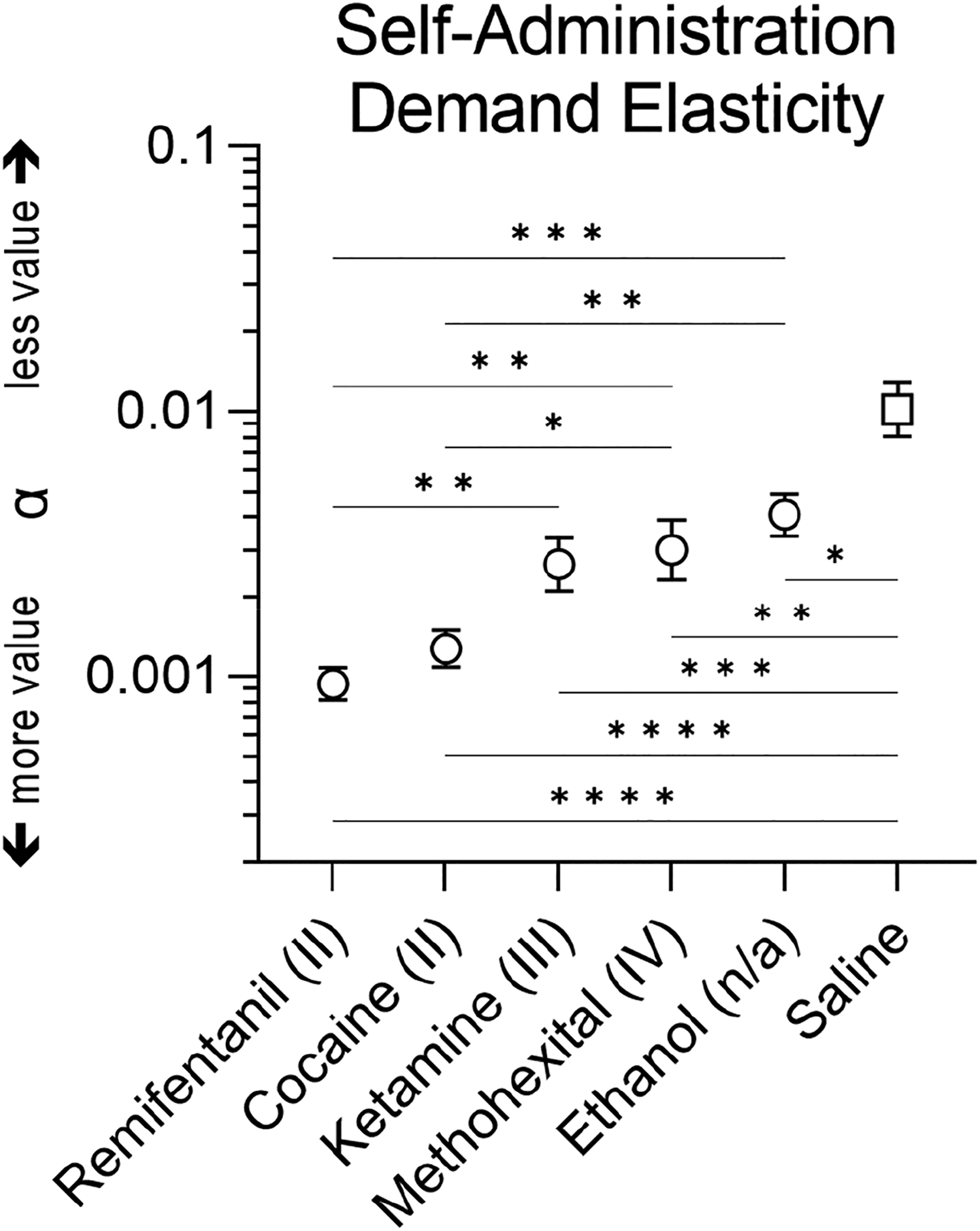
Reanalysis of data (n = 10) obtained from Koffarnus et al. (2012) demonstrates the ability of demand elasticity (log[α] ± SEM) to distinguish the degree of abuse liability among drugs of abuse with known abuse potential. Demand elasticity distinguishes all drugs including ethanol from saline and orders the abuse liability in alignment with drug schedule (schedule indicated in parentheses after drug name). Data consisted of log[α] derived individually for each experimental subject as described in the original manuscript (Koffarnus et al., 2012) analyzed with a one-way ANOVA and Holm–Sidak post hoc tests comparing all conditions to one another in GraphPad Prism 9.
An additional advantage of demand elasticity for the classification of drug abuse liability is that, over a range of psychoactive unit doses of a drug, demand elasticity is independent of drug dose. That is, demand elasticity is analyzed as a function of cost per unit of drug, and a statistically equivalent elasticity measure is typically obtained across all unit doses of a drug that are large enough to be psychoactive and below the cutoff for toxic effects (Hursh & Winger, 1995). For many drugs, this is an approximately 10-fold range of doses. The ability to evaluate a drug for abuse liability and get the same answer regardless of specific dose chosen is a key advantage over dose-dependent abuse liability assessments, particularly as the commonly abused doses of a drug may be higher than the dose that can be safely studied in a human laboratory setting.
Toward a Standardized Demand Elasticity Measurement for use in Drug Scheduling
Despite these advantages, some constraints would need to be in place for demand elasticity to serve as an abuse liability measurement that could be used to categorize a novel drug and rank its abuse liability among existing drugs. Demand elasticity measurement is reliant on nonlinear regression techniques and is therefore affected by analytical choices that are not uniform throughout the field. Furthermore, there are multiple nonlinear demand models that have been proposed to characterize demand data (Koffarnus et al., 2022). Because elasticity can be dependent on these analysis choices, a standardized elasticity-based abuse liability assessment useful for FDA scheduling recommendations would require a standardized experimental design protocol and standardized data analysis protocol. A standard experimental design and analysis protocol would allow FDA and others to gauge abuse liability of novel drugs independent of the laboratory conducting the testing. To achieve a standardized experimental protocol and analysis protocol, development work should be conducted to validate specific design choices.
Timing and Route of Administration
Existing FDA guidance (Center for Drug Evaluation and Research at the US Food and Drug Administration, 2017) has specific criteria for determining the route of administration and timing of outcome variable collection after drug administration. Demand analyses in preclinical animal models are extensions of the FR self-administration experiments already described in detail in FDA guidance, with the primary difference being that a range of FR values and/or range of doses are evaluated so that unit price of drug is parametrically manipulated. Demand experiment guidelines could likely use the existing self-administration timing and route of administration guidance for preclinical animal models.
For human abuse liability models, FDA guidance dictates that controlled double-blind double-dummy experiments are conducted with timing of dosing and route of administration determined based on the results of preclinical data. Human demand experiments have been conducted with self-administration models (Jacobs & Bickel, 1999; Johnson et al., 2004), purely hypothetical models in experienced users (Murphy et al., 2011; Reed et al., 2020; Strickland et al., 2020), and with a hybrid approach (Johnson et al., 2017; Kaplan et al., 2022). This hybrid approach involves an experimenter administering a blinded drug sample followed by a demand assessment asking the participant to indicate how much of the drug they would purchase and consume. This hybrid model, often called experiential demand, would be ideal for the existing protocol for human abuse liability assessment in FDA guidance, as it could be slotted in with the other self-report assessments collected following a controlled administration of the novel drug. Therefore, timing and dose determination for the demand assessments would follow existing guidance and be conducted along with existing measures in the existing experimental paradigm.
Dose(s) of Drug to be Evaluated
Demand analyses have the notable advantage of being robust to dose studied. In other words, the same demand elasticity measurement is obtained over a wide range of doses. For many commonly studied drugs (e.g., heroin and cocaine), this range of doses that result in the same elasticity measurement holds over a 10x range (Hursh & Winger, 1995). Current FDA guidance (Center for Drug Evaluation and Research at the US Food and Drug Administration, 2017) already prescribes procedures for determining the dose(s) of a drug to study for both preclinical and human clinical abuse liability experiments. These same guidelines should be appropriate for demand elasticity measurement in both preclinical and clinical studies, as they are already designed to study abuse liability at a dose that is most likely to have abuse potential.
Range of Costs Evaluated
Demand assessment relies on evaluating the consumption or purchasing of a drug across a range of unit price costs. Cost is operationalized as effort (i.e., lever presses) in animal studies and as monetary price per unit of drug in human studies. The range of costs assessed can impact abuse liability assessment if they do not capture the relevant changes in consumption necessary for resolving elasticity measurement. Therefore, these should be standardized (see also Kaplan et al., 2018; Reed et al., 2020). In human experiential demand models, prices are typically described as cost per dose of the novel drug administered by the experimenter and varied over a wide range from free or nearly free (e.g., $0.01) to a prohibitively costly amount (e.g., $1,000). For human studies, a set range of prices should be predetermined to standardize procedures. Similarly, in preclinical models, response cost is typically assessed from the smallest cost (e.g., FR 1) to a prohibitively high cost, which can be species-dependent. Among nonhuman primates, response requirements of FR 1,000 or more have been used (Koffarnus et al., 2012; Koffarnus & Winger, 2015), while rodent studies typically assess maximum response requirements that are no more than ∼FR 200 (Koffarnus & Woods, 2013; Soto et al., 2011). To standardize procedures, a set of FR values should be predetermined or criteria set for determining the range of FR values to use for a species/drug combination. For both human and animal studies, elasticity is conceptualized as proportional change in consumption over proportional (i.e., log-scaled) changes in cost. Therefore, evenly spaced costs would increase by an approximately constant proportional amount with each FR (e.g., FR 1, FR 3, FR 10, FR 32, FR 100, etc.) or monetary unit price (e.g., $0.01, $0.03, $0.10, $0.30, $1.00, $3.00, etc.). However, it may be beneficial to oversample portions of the demand curve by obtaining consumption estimates at additional costs.
Analysis Choices
Demand analyses are typically conducted with nonlinear regression techniques as the relationship between drug cost and consumption is nonlinear (Kaplan et al., 2021). As a complicating factor, multiple mathematical models have been proposed to describe the relationship between cost and consumption (for recent review, see Koffarnus et al., 2022). Furthermore, the adoption of nonlinear regression techniques is still far from universal, and specific analysis choices can affect outcomes (Kaplan et al., 2021). Demand analysis techniques have progressed enough to make decisions about best practices for individual experiments, but the development of a standardized analysis pipeline that could be employed across the diverse set of novel drugs under abuse liability assessment should be the subject of systematic study prior to implementation. The following are design and analysis choices that would likely need to be standardized prior to issuing guidance to use demand abuse liability assessment for drug scheduling purposes, ideally after dedicated study aimed at determining which choices yield the most predictive results.
Participant instructions
For human experiential demand abuse liability assessment, a set of instructions is typically read to participants prior to their completing the demand assessment. These instructions are meant to prepare participants to respond in such a way that would reflect their own consumption preferences for the novel test drug, and specify the consumption period, the deprivation state, access to other drugs, and other relevant information. Standardized instructions have been proposed for use in demand assessments (Kaplan et al., 2018; MacKillop et al., 2008; Reed et al., 2020), and these should be validated and standardized for use in drug scheduling experiments.
Identification and management of outliers
Management of outliers in consumption data collected for demand analysis can be a critical decision as drug consumption data across a range of users is often positively skewed, with a relatively small subset of participants indicating consumption values far above the mean. This is perhaps unsurprising, as substance use disorders are often characterized by drug consumption far exceeding that of the general population. Therefore, analyses may need to avoid the censoring or removing of ‘outlier' values based on distance from the group mean as these values could conceivably represent possible consumption values (Rzeszutek et al., 2022) and removing them could artificially constrain the variability inherent in drug consumption data. Instead, outlier values could be operationalized as those consumption values that are impossible and could therefore be attributed to the participant misunderstanding the task instructions. For example, if a participant indicates a consumption amount of “1 million units” in a 24-hour period for a drug where a single unit produces a noticeable psychological effect for an hour, this amount is likely attributable to a misunderstanding of the task or exaggeration. However, the specific cutoff for determining unreasonable or impossible responses would likely require further study, as this could be an ambiguous point for novel drugs that participants have no prior history using.
Handling of missing data
In the highly controlled experimental context described for abuse liability assessment in FDA guidance (Center for Drug Evaluation and Research at the US Food and Drug Administration, 2017), missing data should be extremely rare. However, missing consumption data could arise in animal experiments if toxic effects occur, if an adverse event is experienced in human clinical experiments, or if a participant withdraws from a study after contributing partial data. Imputation methods can be problematic for drug consumption data due to the common occurrence of positively skewed consumption values, similar to the reason to avoid censoring outliers. Therefore, analysis techniques that rely on imputation for missing data should be avoided in favor of modeling techniques that rely on maximum likelihood estimation (e.g., mixed-effects models) or similar procedures that can accommodate missing data and appropriately apply a statistical inference penalty to datasets with missing data (Kaplan et al., 2021).
Treatment of nonsystematic data patterns
The concept of demand elasticity relies on the negative association between the cost of a commodity and consumption of that commodity. That is, consumption tends to decrease as cost increases. An algorithm to detect whether a series of data adhere to this general assumption has been proposed (Stein et al., 2015), and this algorithm is sometimes used to exclude data from further analysis. This algorithm is well-suited for identifying data that is atypical from a behavioral economic theory standpoint, but blanket exclusions of data based on adherence to a predetermined pattern have the potential to bias statistical analyses and artificially reduce variability inherent in the data. Robust statistical models like mixed modeling can be carried out without removing data based on adherence to predetermined patterns for datasets with modest degrees of nonsystematic data (Kaplan et al., 2021). Furthermore, as a method to screen novel drugs with unknown properties for abuse liability, presuppositions about what constitutes valid data should be kept to a minimum. Drugs that affect cognition or logical reasoning could conceivably result in “atypical” demand data, which would be an accurate reflection of the effects of these drugs.
Nonlinear demand model chosen
Koffarnus et al. (2022) chronicles common proposed models to characterize demand, detailing advantages and disadvantages of each. For the purpose of screening for and ranking the abuse liability of a novel drug compared to known drugs of abuse, a demand model that can isolate and accurately assess demand elasticity for a wide range of drugs from different drug classes would be ideal. The popular demand model proposed by Hursh and Silberberg (2008), as well as variants of that model (Gilroy et al., 2021; Koffarnus et al., 2015), were explicitly designed to isolate the demand elasticity parameter and provide a method to calculate this parameter in varied contexts (Koffarnus et al., 2022). These models contain a single fitted parameter (α) that characterizes the demand elasticity of a drug independent of the potency of the drug or specific dose chosen for assessment. The original model and the proposed variants differ only in the scale on which elasticity is measured and optimized. The original Hursh and Silberberg (2008) model and exponentiation of this model (Koffarnus et al., 2015) assess demand elasticity as proportional change in consumption on a logarithmic scale, while Gilroy et al. (2021) assess change on the log-like inverse hyperbolic sine scale that is similar to a proportional log scale at large consumption values, but differs from this scale for smaller consumption values. Each model differs in the scale over which curves are optimized. Hursh and Silberberg (2008) optimize curves on a log scale, which precludes the inclusion of consumption values of zero in the analysis. Koffarnus et al. (2015) and Gilroy et al. (2021) avoid this limitation by optimizing data on a linear (Koffarnus et al., 2015) or log-like inverse hyperbolic sine (Gilroy et al., 2021) scale, respectively. See (Koffarnus et al., 2022) for an in-depth review of these models, as well as others that have been proposed. Ultimately, however, the ability to compare abuse liability results of novel drugs to historical experiments conducted for other drugs requires that analysis procedures remain consistent over time. For an important use case as an abuse liability assessment for scheduling novel drugs, the practical utility of each model for that specific outcome should be further studied before an analysis pipeline is codified.
Constraints for fitted parameters
In addition to the free parameter for demand elasticity (α) for the demand models discussed above, these models include free parameters for the estimated maximum consumption when the cost is unconstrained (Q0) and the span or range of the function (k). Typically, Q0 is estimated as a free parameter along with α (although this may not be necessary if only demand elasticity outcomes are important for the experimental aims). This parameter can be useful for estimating the absolute quantity of drug that may be used, but is less useful for estimating the abuse liability of a drug. The k parameter is necessary for fitting, but hasn’t been shown to have interpretive or theoretical utility to help understand the properties of a novel drug. Additionally and problematically, the k parameter and α parameter are also dependent on one another (i.e., the choice of k parameter affects the value of α while holding abuse liability constant). To resolve this, an analytical combination of α and k has been proposed, deemed “essential value”, to quantify abuse liability across a range of k values chosen for specific analyses (Hursh & Silberberg, 2008). Alternatively, a constant k value can be used across all analyses, although this would result in poor curve fits in some cases where the predetermined k value is a poor fit to the data. Note that fixing k to the value of Q0 has also been proposed as a method to reduce the influence of k (Gilroy et al., 2021), but that does not resolve the issue of varying k values affecting the interpretation of α or abuse liability. Instead, this just replaces the conflation of k and α with a conflation of Q0 and α and would still require an additional step to resolve. These analytical issues are an ongoing area of study and require additional validation work to determine which set of analysis choices would be optimal for the estimation of abuse liability across drug classes, species, and laboratories.
Analysis summary
The above issues are common to any statistical analysis, but have not been universally agreed upon for demand analyses given the complexity of nonlinear regression and diversity of proposed demand models. A reproducible and standardized choice for each of the above would likely need to be refined and tested with purposeful parametric work aiming to validate the resulting protocol as a tool for making abuse liability assessments for novel drugs. Ideally, this validation would be done with data collected for this purpose with a wide range of drugs across drug classes with known abuse liability under comparable experimental procedures.
Conclusions
Behavioral economic demand holds great potential for use as an abuse liability assessment in the scheduling of novel drugs with abuse liability. Advantages of demand analyses include (1) quantitative abuse liability results that allow for relative comparisons and ranking among existing drugs with known abuse liability, (2) the ability to collect analogous measures of abuse liability in both preclinical and human clinical models, and (3) minimal extra work to add demand analyses to those analyses that are already recommended in FDA guidance (Center for Drug Evaluation and Research at the US Food and Drug Administration, 2017). Challenges primarily arise with the complicated nonlinear regression analysis techniques associated with this method, and the need for standardized design and analysis choices that would allow for abuse liability comparisons across drug classes and laboratories that conduct the experiments. These challenges are resolvable, however, and directed work to compare different methodological techniques could help to standardize an experimental protocol and analytical pipeline for the rigorous incorporation of behavioral economic demand techniques into FDA scheduling recommendations.
Footnotes
Acknowledgements
The author would like to thank Brent A. Kaplan for helpful comments in preparing this work. All opinions expressed are the author's alone and not necessarily reflective of these entities. MNK has no other conflicts of interest to report.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MNK receives funding for his work from the National Institutes of Health and the University of Kentucky.