
Abstract
Community colleges have long been recognized as essential collaborators in the training of frontline health care professionals. More recently, growing policy and programmatic interest has led to an increased emphasis on integrating health professions training at community colleges into the broader continuum of public health education, and creating viable professional pathways for students entering the field at all levels of the continuum. This study examined the specific role of community colleges in preparing graduates for the “health navigator professions” including community health workers, health care navigators, health insurance navigators, and similar professions. A national online survey was used to examine the current practices of community colleges regarding training for these professions, and perspectives on the Health Navigator curricular framework developed by the Framing the Future Task Force of the Association of Schools and Programs of Public Health. Data were collected from approximately 260 community college leaders engaged in health professions education. Results suggest a preference for flexible, credit-granting associate-degree programs that are heavily embedded in the community, and that integrate core community health, health care workforce, and health insurance needs. Respondents preferred applied associate degree programs as well as associate degree program designed for transfer. They also expressed interest in academic certificate program and online programs. Strategies for establishing sustainable community-based workforce partnerships and aligning with the state policy context for community health worker training are also discussed.
Introduction
This study examines the training and preparation of health navigator professions at community colleges in the United States. Community colleges have an established role in training frontline health care professionals such as paramedics and nursing or medical assistants and, more recently, have also become increasingly involved in the training of health care navigators, community health workers, and similar professions. Drawing on a national survey of community college leaders in the health-related disciplines, this article presents respondent perspectives on current training practices, as well as the broader potential for health navigator program growth in the community college context.
Definitions
The “health navigator professions” represent a host of interrelated professions or job titles that have traditionally been associated with frontline public health service. Community health workers (CHWs), health care or patient navigators, lay health advisors, and promotoras are but a few of the terms commonly used to define the distinct, yet potentially overlapping, duties and services performed by these frontline public health workers (Brownstein, Mirambeau, & Roland, 2013; Rosenthal et al., 2010; U.S. Centers for Disease Control and Prevention, 2011; U.S. Health Resources and Services Administration, 2007). To better align with the Association of Schools and Programs in Public Health (ASPPH) Framing the Future Task Force’s “Health Navigator” Framework described elsewhere in this special issue, the term “health navigator professions” is employed in this article as an umbrella term to refer to these varied professions, while other terms, such as CHW, patient navigator, or health insurance navigator, will be used when referring to a specific subset of the health navigator professions.
While recognizing that different terms are preferred or most appropriate in different settings, the “health navigator” term employed here is used to emphasize the fact that this research focused on formal academic preparation programs in the community college context and the potential applicability of ASPPH’s Health Navigator Framework. While these public health professionals may vary widely in terms of service area and focus, the ASPPH Framework provides a core set of content outlines for CHWs, health care navigators, and others, that can be further tailored to local needs and contexts. The aim of this research was therefore to test the perceived utility or desirability among community college audiences for providing a common academic framework for training these professions.
Public Policy Context
The current public policy landscape in the United States plays an important role in the consideration of community college training for the health navigator professions. The Patient Protection and Affordable Care Act (ACA) places an unprecedented emphasis on extending preventive health care and public health services to all Americans. Recent government figures show that upwards of 11 million enrollees have already signed up for insurance coverage in the new Marketplace, and an additional 4.8 new beneficiaries have been enrolled in Medicaid and the Children’s Health Insurance Program through expansion efforts since open enrollment under the federal insurance Marketplace began in October 2013 (U.S. Centers for Medicare & Medicaid Services, 2014; U.S. Department of Health and Human Services, 2015). Furthermore, the law emphasizes standard insurance coverage for new preventive services, expects health care organizations to play an increasing role in providing integrated community-oriented care, and provides quality initiatives whereby reimbursement is tied to specific outcome measures, further encouraging providers to support community health services (Alssid & Goldberg, 2013; Patient Protection and Affordable Care Act, 2010).
Grant funding for the training and employment of the health navigator professions has also increased. For example, the U.S. Department of Health and Human Services announced $67 million in grant funding for 105 health insurance navigator groups within 34 states with federally facilitated or state-partnership health insurance marketplaces, and the Health Resources and Services Administration has provided $150 million to support outreach and enrollment assistance activities in a total of 1,159 health centers (U.S. Department of Health and Human Services, 2013; U.S. Health Resources and Services Administration, 2014). Within this context, the U.S. Department of Labor predicts an increase of at least 25% in CHW-type positions from 2012 to 2022 (U.S. Department of Labor, 2013). While it is not likely that these national forecasts will apply to all regions and locales, these figures are suggestive of an overall positive trend in national job growth for the health navigator professions.
The growing emphasis on the training and employment of the health navigator professions provides an opportunity to examine the role of community colleges in supporting these workforce needs. The ASPPH Health Navigator Framework proposed one such avenue for formal academic training. The aim was not to replace the numerous other contexts in which the health navigator profession are, and will continue to be, trained—such as through area health education centers, nonprofit organizations, and other trainers and employers—but rather to better articulate the role of community colleges within the continuum of public health education and to establish a framework for competency-based, formal academic preparation for these professions and, potentially, future academic study or professional advancement (Framing the Future Task Force, 2013).
Survey Design and Procedures
This analysis consisted of primary data collection through an online survey of community college leaders serving in health professions education. As health navigator training at community colleges is an emerging and rapidly evolving phenomenon, we learned that little published literature is available that explores, at a national level, the preferences of community college decision makers toward formal academic programming in this area. Some of the advantages of online survey design include its economic feasibility and relatively rapid data collection (Sue & Ritter, 2012). Online surveys may also engender higher response rates and be more effective at addressing potentially sensitive topics (Kays, Keith, & Broughal, 2013). The study design described below was submitted to the Institutional Review Board at George Washington University and was determined to be exempt research.
Survey Sample
The target audience of this survey was deans and directors of health-related programs at community colleges throughout the United States, and was administered in partnership with the League for Innovation in the Community College (the League). The League is a nonprofit organization providing leadership in academic innovation and program development for community colleges in the United States and around the world. To identify an appropriate survey sample, two related sources were used. First, the League’s membership database as of October 2014 was queried for individuals with the title of “dean” for allied health programs, as well as other individuals self-identifying with a “director” position title in allied health, such as academic vice presidents and divisional leaders. The League’s membership database returned 390 recipients. Second, non-League members were added to the survey distribution list using similar search procedures in distribution lists of allied health leaders at community colleges that were created or purchased by the League. Five hundred twenty-five recipients were added to the distribution list through these additional sources, for a total of 915 individuals on the final survey distribution list.
This two-pronged approach, including both League Alliance members and nonmembers, represents a convenience sample. The American Association of Community Colleges (2015) reports that there are approximately 1,100 community colleges in the United States; using this estimate, this convenience sample could represent approximately 80% of community colleges in the United States.
Survey Content
The survey was organized around four key content areas: (1) academic, college, and student characteristics of the respondents’ community college; (2) information regarding the provision of health navigator-type programming; (3) perspectives on the Framing the Future Health Navigator Framework; and (4) characteristics of the local environment. The majority of questions were collected as categorical variables, or ordinal variables on numeric Likert-type scales. The survey also included opportunities for free-response feedback.
To assure that the target audience was reached, screening questions were also included in the survey to ascertain respondents’ leadership role at their college, and their involvement in programmatic decision-making processes concerning health-related programs.
Survey Format and Distribution Procedures
The survey was adapted for online release by a computer-programming specialist at the League, and went through content and usability testing by individuals advising this project, including League research and technical staff and content experts affiliated with the ASPPH Framing the Future initiative. The survey was housed on the League’s secure server and was accessible by invitation only.
The initial survey invitation and informed consent documentation were distributed by the League via email, with a personalized link to the online survey platform, in October 2014. Personalized links were used to track respondent completion and to help assure that only those invited to participate had access to the survey. However, all sensitive data were encrypted on the server and removed before data analysis. The survey itself collected no sensitive information, aside from an optional question about the respondents’ college location (i.e., state).
Three follow-up invitations were sent to remaining nonrespondents at 2-week intervals over a period of 6 weeks from October through December 2014. At the close of this initial open period, a final, more personalized survey invitation was sent to all nonrespondents.
Finally, a targeted follow-up attempt to reach additional nonrespondents was conducted with a random sample of 100 nonrespondents in December 2014 and January 2015. These 100 nonrespondents received another personalized survey invitation, with options for survey participation via phone or email. This additional targeted follow-up approach was used in an effort to include as many perspectives from “nonrespondents” as possible, and to attempt to assess whether nonrespondents were different than respondents.
A total of 915 survey invitations were sent. Of these, 98 were undeliverable, having been sent to invalid email addresses and 580 were sent to nonrespondents. Of the remaining 262 successful invitations, 236 valid online responses were submitted. Removing undeliverable invitations from the denominator, the response rate to the online version of the survey was 29%, which could represent approximately 21% of the estimated 1,100 community colleges in the United States.
During the targeted outreach to nonrespondents described above, an additional 25 partial survey responses were obtained via phone and email, which were included in subgroup analyses only, as described below. While only 25 nonrespondents were reached through this targeted follow-up approach, many of these individuals were willing to provide additional background and perspectives that could not have been collected through the more structured online survey.
Statistical Methods and Analysis
The de-identified data set was imported into Stata 13 for analysis. Descriptive statistical procedures were used to characterize respondent feedback in the four content areas described above. This study proposed no causative model but instead sought to explore current practices and perspectives at community colleges.
A series of subgroup comparisons and tests of statistical significance were, however, identified pre hoc and incorporated into the analysis. As the variables of primary interest in this dataset were categorical and ordinal in nature, these analyses involved nonparametric measures such as Kruskal–Wallis one-way analysis of variance. The primary aim of the subgroup comparisons was to test the robustness of the descriptive findings by comparing respondent subgroups on a number of key variables, of which some were unique to individual respondents, and some state-level policy characteristics that were matched to respondents for analysis.
Results
Respondent Characteristics
The 236 online survey respondents come from community colleges across 42 states. Eight percent of respondents chose not to indicate a state. Of those providing location information, the states with the highest participation included California (10% of respondents), North Carolina (7%), Texas (6%), and Illinois (5%). Table 1 provides a summary profile of respondents. Due to privacy constraints, it was not possible to collect college-level data on nonrespondents to compare with these respondent characteristics, but as will be discussed below, subgroup analyses comparing survey respondents to individuals that were reached through targeted follow-up did not show any statistically significant differences between these two groups.
A Profile of Survey Respondents.
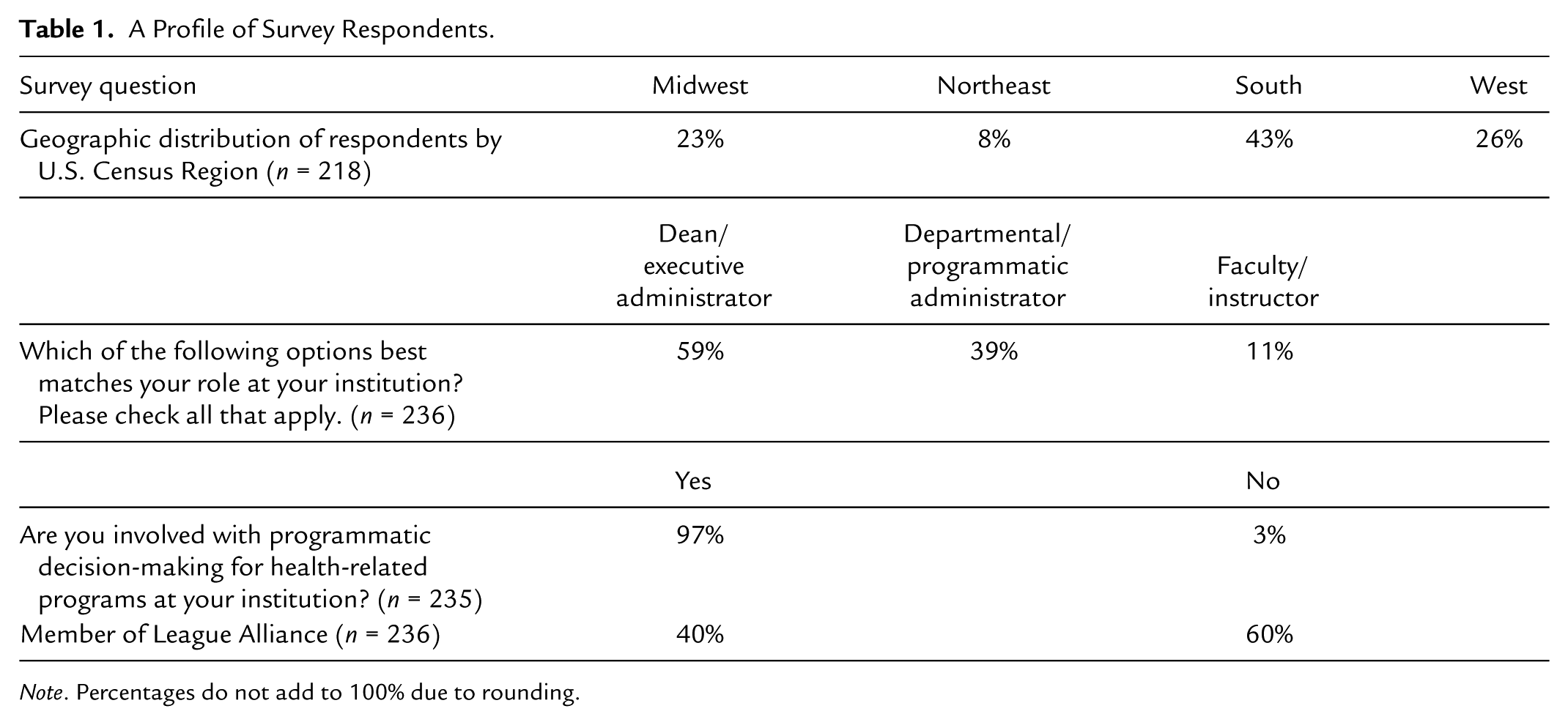
Note. Percentages do not add to 100% due to rounding.
Current Health Navigator-Type Program Offerings at Community Colleges
Respondents were asked to describe the broad categories of academic programs offered at their colleges as well as specific health-related professions (Table 2). More than 90% of all respondents reported that their colleges offer general arts and science disciplines for transfer to 4-year colleges, education-related disciplines, and allied health disciplines. Business and public administration offerings were also frequently reported (89%). Only one discipline group, environmental studies, was reported by a minority of respondents (48%).
Frequency (%) of Academic Program Offerings Reported by Respondents.
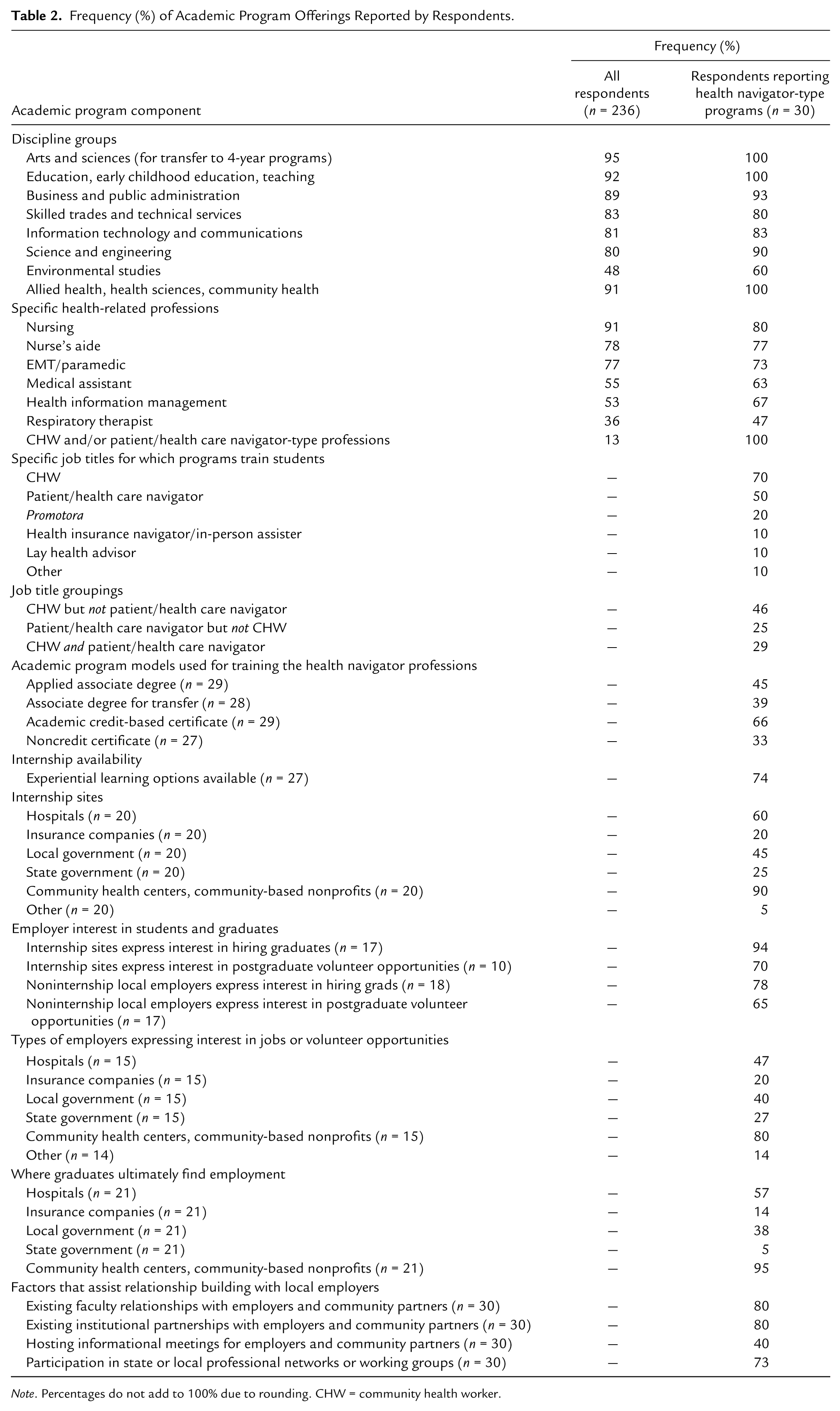
Note. Percentages do not add to 100% due to rounding. CHW = community health worker.
Among the health-related disciplines, nursing programs were most commonly reported (91%), followed by nurse’s aide (78%), EMT/paramedic (77%), and medical assistant programs (55%). Thirteen percent of respondents reported that their colleges offer health navigator-type training programs.
Of the respondents reporting health navigator-type training programs, 73% indicated that their colleges offer five or more of the seven health-related professions listed in Table 2. As with the broader pool of respondents, nursing, nurse’s aide, and EMT/paramedic programs were also the most commonly reported disciplines among respondents with health navigator-type training programs at their colleges.
Respondents were asked to use the terminology of their colleges to describe the profession(s) or job title(s) for which their health navigator-type programs provide training. Respondents were allowed to select as many terms as applicable. Community health worker (70%) and patient/health care navigator (50%) were the most commonly reported terms. Except for two respondents who did not identify with any of the job titles provided, all respondents selected at least one of the two above-mentioned terms.
As respondents were able to select more than one term, it is also possible to look at common job title groupings that were reported. Using CHW and patient navigator as organizing terms, we see that 46% of respondents indicated that their programs train for CHWs but not patient navigators. Twenty-five percent reported training for patient navigators, but not CHWs, and 29% reported training for both CHWs and navigators (Table 2).
Among the respondents reporting health navigator-type training programs at their colleges, over half (57%) noted that these programs were no more than 2 years old, with 40% reporting that their programs have been in operation for less than 1 year. The online appendix (available at http://php.sagepub.com/supplemental) provides further details of these findings.
Academic (credit-based) certificates were the most commonly reported program format for health navigator-type programs (reported by 66% of respondents with existing programs), followed by applied associate degree options (45%), associate degrees for transfer to 4-year programs (39%), and noncredit certificates (33%). Respondents were able to select more than one academic program model, and the majority did so. However, 13% of respondents with existing health navigator-type programs reported offering noncredit certificates only, with all others reporting at least one credit-based option. Seventeen percent of respondents reported offering academic certificates only.
For those colleges with an applied associate degree program option, respondents were asked to provide the academic department(s) linked to those degrees. The most common department affiliations were community health (46%) and human services (23%), though responses ranged from health technology and respiratory therapy to business, design and workforce.
Experiential Learning and Community Partnerships
Seventy-four percent of respondents reported that the health navigator-type training programs at their colleges included options for experiential learning. While responses ranged from one to four or more, two semester credit hours was most commonly reported (41%). Two respondents reported that experiential learning opportunities were available but not required.
The most common internship site reported by respondents was community health centers (federally qualified health centers) or other community-based organizations (reported by 90% of respondents). Hospitals or hospital networks was the second most common response (60%), followed by local government agencies (45%), state government agencies (25%), and health insurance companies (20%).
Ninety-four percent of respondents reported that experiential learning sites had expressed an interest in program graduates for post-graduate employment. Furthermore, 78% of respondents reported that other local organizations not currently providing experiential learning opportunities for their programs’ students had expressed an interest in potentially hiring program graduates. Respondents also noted that more than half of all internship sites, as well as other local employers not hosting interns, had expressed an interest in providing volunteer opportunities for program graduates (Table 2).
Respondents were also asked to describe the most important factors in establishing and maintaining effective employer relationships for their health navigator-type training programs. Respondents were asked specifically about the importance of four specific factors, including (1) existing faculty relationships with employers and community partners, (2) existing college partnerships with employers and community partners, (3) hosting informational meetings for employers and community partners, and (4) participation in state or local professional networks or working groups. Respondents were also given an opportunity to identify other factors not specifically queried.
Existing faculty relationships, and existing college partnerships, with employers and community partners were both reported by 80% of respondents. Seventy-three percent of respondents reported that participation in state or local professional networks or working groups was also important, and 40% identified hosting informational meetings for employers and community partners as an important factor (Table 2).
Perspectives on Framing the Future’s Health Navigator Program Framework
Beyond studying the current state of practice at community colleges regarding health navigator-type training programs, this survey also aimed to assess respondents’ perspectives toward the adoption of new health navigator training programs, and the potential barriers and facilitators that may influence these perspectives. All online survey respondents, regardless of whether they currently have health navigator-type programs, were asked to share their perspectives on the ASPPH Health Navigator curricular framework. The Framework includes foundational and public health core courses; coursework in the content areas of prevention and community health, health care delivery, health insurance, as well as accessing and analyzing health information; and opportunities for experiential learning and health-related electives. The Framework is designed primarily as an applied associate degree that can be adapted to local needs and preferences (Riegelman, Wilson, Dreyzehm, & Huffard, 2014).
Respondents were asked a series of questions as to whether their interest in developing a health navigator training program based on the Framing the Future Framework would increase if certain factors were in place. These questions fell in two broad categories: factors pertaining to the curricular content of the program itself, and external factors that may impact program implementation or desirability (Table 3).
Extent to Which Specific Factors Would Increase Interest in Offering Framing the Future’s Health Navigator Program and Specific Program Model Recommendations.

Note. Percentages do not add to 100% due to rounding.
Curricular Factors Affecting Respondents’ Interest in Health Navigator Framework
When asked if their interest in the Framework would increase if it focused only on a specific content area or disciplinary track (prevention and community health, health care delivery, or health insurance), 75% expressed a strong preference for keeping all three tracks in the framework, compared with 30% of respondents, if the program focused only on community health; 42% if it focused on health care delivery only; and 23% if on health insurance only. Disinterest in specific program emphases echo these findings, with only 9% of respondents indicating that they would “not at all” be interested in the Framework if it were to include all three content areas (Table 3).
In terms of degree formats, respondents expressed the strongest interest in applied associate degree options (68% being greatly interested), followed by associate degrees for transfer and academic certificates (53%). In contrast, the majority of respondents were not interested in noncredit program options, with 59% indicating that they would not at all be interested in a noncredit program model. Online learning also attracted considerable interest, with a majority of respondents (62%) stating that including options for online or distance learning would increase their interest in offering the program at their colleges.
External Factors Affecting Respondents’ Interest in Health Navigator Framework
There were four external factors that more than 85% of all survey respondents indicated would greatly increase their interest in offering the Health Navigator Framework at their colleges. Of these, three were directly related to local employers: local employers expressing an interest in potentially hiring program graduates; needs assessment or employer survey data demonstrating job availability; and local employers expressing interest in providing experiential learning opportunities for students. The other very highly ranked factor was sufficient student interest from students to suggest that enrollment needs would be met.
A majority of respondents also answered positively to the remaining factors queried in the survey, including national employment statistics indicating at least 15% job growth in the program area in the next 5 years (81%); professional or trade association recommendations (67%); and successful program modeling from other community colleges (58%).
Small but consistent minorities indicated that the seven above-mentioned factors would not at all increase their interest in offering the framework (representing 6% to 14% of respondents, depending on the specific variable).
Respondent Recommendations
The above-mentioned internal and external factors described above can be helpful in understanding the degree to which specific components of the Health Navigator Framework appeal to survey respondents. To better understand how these preferences translate into specific program recommendations, respondents were then asked more directly which types of academic program models they would recommend, if their college were to adopt such a program. Responses mirrored the preferences expressed above, with applied associate degrees being highly recommended by 65% of respondents, followed by associate degrees for transfer to 4-year colleges (57%), academic certificates (50%), and noncredit certificates (14%; Table 3).
Naming Academic Programs
The survey also asked all respondents, including those at colleges with existing programs, to react to the proposed name of the Framework. As the health navigator professions include a variety of job titles and service areas, respondents were asked to rate the term “health navigator,” as adopted by ASPPH, as well as “community health worker” as potential titles for these academic training programs.
In both instances, respondents tended to express a sense of ambivalence or indifference toward program names (Table 3). Only 32% of respondents indicated that “community health worker” was a highly appropriate name, and for “health navigator,” only 30% indicated the same. Respondents were given the opportunity to provide open-ended feedback at the conclusion of the survey, and some took this opportunity to discuss the question of naming. The following quotations provide examples of respondents’ diversity of opinion: In this region there is much confusion about the term “community health worker.” Most people in this area consider it to be a short-term training program for lay people. I think using this as a generic term would make it hard to market a credit program. (Anonymous survey respondent) I would be concerned regarding the title of the program especially for Community Health Worker. If the term Health Navigator was used, I would make sure this is the same term used by employers and within the community. I think the program is a great concept. (Anonymous survey respondent) When I hear the term “health navigator” I think of the ACA, and the public might as well. Therefore, I believe a better name is needed. (Anonymous survey respondent) This is an interesting program but I’m not sure of the title. Is there an SOC code for Health Navigator yet? (Anonymous survey respondent) [SOC refers to the Department of Labor’s Standard Occupational Classification system]
Subgroup Analyses
To test the robustness of survey results across subgroups of respondents, 10 core survey questions were selected pre hoc to examine potential variation across subgroups of respondents:
Program focused only on community health (traditional community health worker core competencies)
Program focused only on preparing students to work in health care delivery settings
Program focused only on preparing students to work in health insurance settings
Program included all three content areas (community health, health care delivery, health insurance)
Program included an applied associate degree option
Program included an associate of arts degree option (for transfer to 4-year program)
Program included an academic (credit-based) certificate option
Program included noncredit certificate options
“Health navigator” program title
“Community health worker” program title
As all of the above questions were assessed on a numeric Likert-type scale, the Kruskal–Wallis test was used to individually test these questions (as the dependent variable) across nine consecutive specific subgroup comparisons (as the independent variable). The specific groups were identified using five survey-specific (individual-level) variables inherent to the dataset and four external (state-specific) variables that were matched to survey respondents. For each specific comparison, the null hypothesis tested was that the subgroups were statistically equivalent to each other, at the 95% confidence level.
Individual-level variables that were tested were based on survey respondents’ answers related to the following: (1) the presence of existing health navigator-type training programs, (2) their personal leadership role on campus, (3) their involvement in programmatic decision making for health-related programs, (4) whether their colleges are League Alliance members (as the survey was sent under the auspices of the League to its members as well as nonmember community college partners), and (5) the date on which the survey was submitted (comparing subgroups of survey respondents by week, including the so-called “nonrespondents” who were reached through phone and email follow-up after the online submission period had passed).
State-specific variables, that were also individually matched to respondents, included Medicaid expansion status and Health Insurance Marketplace type in the state, as well as two final variables measuring the presence of formal legislation regarding the training and certification of community health workers. The aim of including these additional variables was to ascertain if state-level policy decisions, that could potentially affect the workforce and training environment for the health navigator professions, could suggest any relationship with respondent preferences.
Table 4 provides a summary of findings for Kruskal–Wallis tests run on each of these nine variables. While the p < .05 threshold was used as a measure of statistical significance in this table, it is important to note that due to the multiple hypothesis tests performed on this sample, there is the possibility of type I errors, i.e., falsely identifying findings as statistically significant. If the Bonferroni correction is applied, a p value of .005 would be necessary to confirm statistical significance (α/n, or .05/10). The following discussion highlights all findings that are statistically significant at the p < .05 level, but p values of less than .005 may therefore be of special interest. The online appendix (available at http://php.sagepub.com/supplemental) provides a raw numeric version of Table 4, which includes p values for all test statistics that were performed.
Summary of Findings From Nine Consecutive Subgroup Comparisons of Survey Respondents Using Kruskal–Wallis One-Way Analysis of Variance.
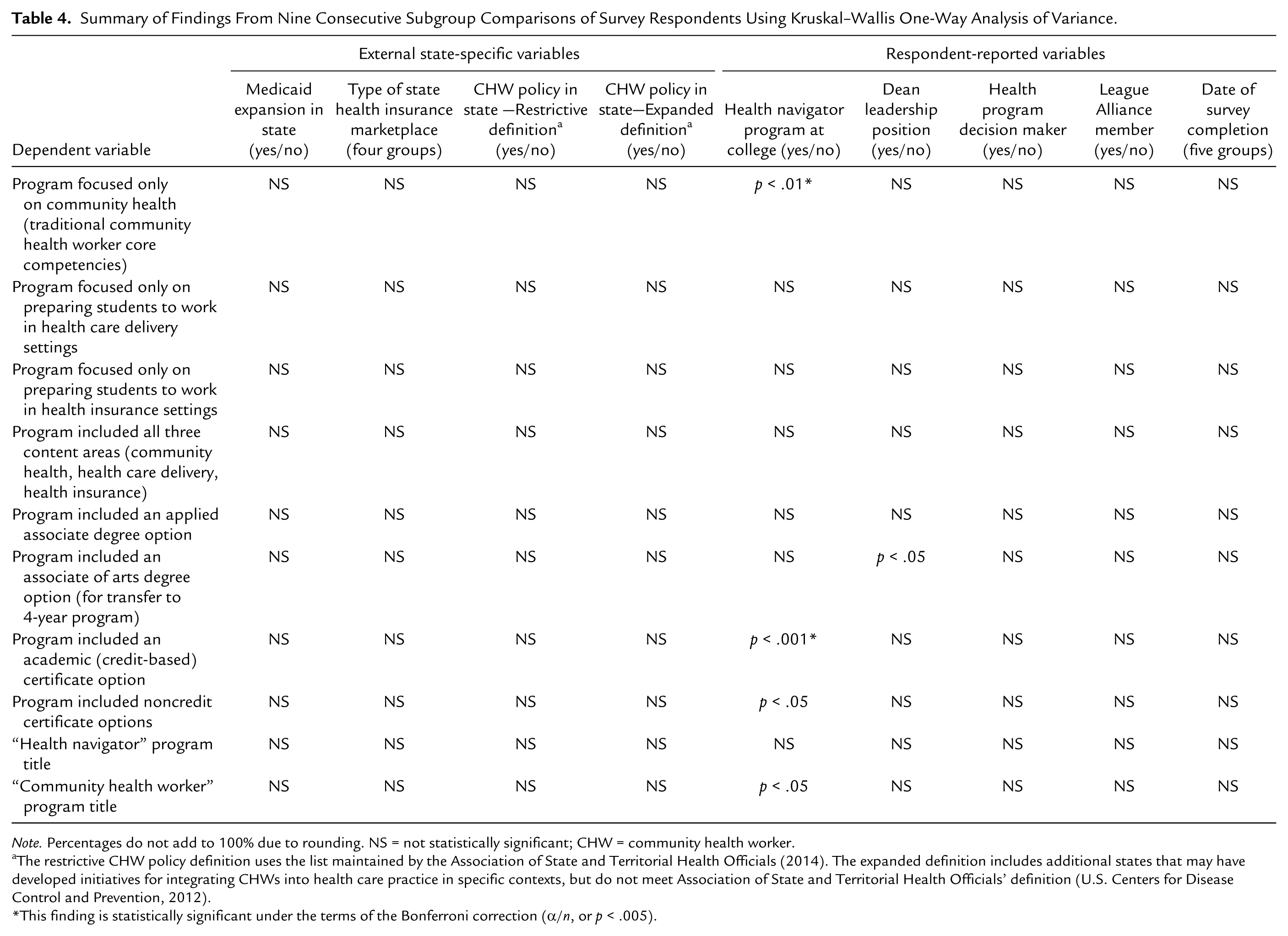
Note. Percentages do not add to 100% due to rounding. NS = not statistically significant; CHW = community health worker.
The restrictive CHW policy definition uses the list maintained by the Association of State and Territorial Health Officials (2014). The expanded definition includes additional states that may have developed initiatives for integrating CHWs into health care practice in specific contexts, but do not meet Association of State and Territorial Health Officials’ definition (U.S. Centers for Disease Control and Prevention, 2012).
This finding is statistically significant under the terms of the Bonferroni correction (α/n, or p < .005).
There were no statistically significant (p < .05) findings for any of the state-level variables. Regarding the individual-level subgroup analyses, four of the nine test statistics were statistically significant (p < .05) when respondents with existing health navigator-type training programs at their colleges were compared with the broader group. Two of these tests concerned the theme of program identity and curricular content. The first was the dependent variable concerning whether interest in the health navigator framework would increase if it focused only on community health (H statistic = 8.265, 1 degree of freedom, p = .004), and the second was the perceived appropriateness of the “community health worker” program title (H statistic = 5.127, 1 degree of freedom, p = .024).
In both instances, respondents with existing programs ranked higher than expected, more often indicating a greater interest than expected in the program only focusing on community health and in the “community health worker” program name. Respondents with existing programs indicated that the most common professional job title for which their programs train is the community health worker title, so it follows that they may also have a preference for a community health program emphasis and name. Similarly, it is likely that the broader pool of respondents, lacking this program-specific context, may be less attracted to the notion of programs emphasizing the “community health worker” only.
The two remaining statistically significant (p < .05) findings within this subgroup analysis concern academic program model. Both dependent variables related to whether interest in the framework would increase if it included options for academic (credit-based) and noncredit certificates showed a statistically significant difference in distributions across these populations (for academic certificates: H statistic = 14.849, 1 degree of freedom, p = .0001; for noncredit: H statistic = 6.168, 1 degree of freedom, p = .0130).
Once again, the subset of respondents with health navigator-type programs ranked higher than expected, when compared to the larger pool of respondents. It is not surprising that respondents with existing programs would value credit-based or noncredit certificates more than other respondents. While the broader literature on community colleges suggests a general preference for degree programs over certificates, the respondents with existing health navigator-type programs in this sample reported academic certificates as the most common program element. It seems plausible, therefore, that they would have a stronger preference for nondegree programs than the broader sample.
There were no statistically significant (p < .05) findings for comparisons involving the early and later respondents or League Alliance members versus nonmembers. When deans were compared to non-deans, one statistically significant (p < .05) finding emerged. Deans ranked lower than expected, in reported interest for transfer degrees, compared to the broader population (H statistic = 4.772, 1 degree of freedom, p = .029).
It is not immediately clear why this effect was observed. One potential explanation is that because this survey targeted allied health deans, and most allied health professions at the community college level emphasize career and technical training for immediate entry in the workforce, these deans would be less inclined to express interest in transfer programs. As the health navigator framework presented in this survey is anchored as an applied associate degree, this finding is not particularly concerning.
Discussion
This survey explored the current role and future prospects of community colleges in training health care navigators, community health workers, and similar professional roles serving in the frontlines of public health and health care. This survey, while relatively small in scope, is the first national snapshot of community college preferences toward the adoption of formal academic programs for the health navigator professions. Although a minority of community colleges currently offer health navigator training options, the number of programs is growing. According to survey results of these college representatives fully half of their health navigator programs were developed within the past year. Furthermore, while the majority of existing health navigator training programs are based on a certificate model, survey respondents expressed a preference for developing associate-level program options (for direct employment, and for transfer to 4-year programs) over certificate and noncredit options; and for integrated program models training across the health navigator professions, instead of more focused programming around specific CHW or patient navigator workforce goals.
The results also emphasize that that internships are an important component of training programs, and occur in a variety of settings, from community health centers and nonprofit organizations, to government agencies and hospitals. This research shows that there is considerable overlap between the organizations where students complete program internships, and where they ultimately work. The ability of program staff to forge connections with community partners and employers is thus critical.
For colleges that may wish to develop future programming in this area, factors such as hiring program staff who bring strong professional connections with the health navigator professions, drawing on existing college relationships with community partners in related allied health fields, involving community actors in all stages of program development, and participating actively in state and local workforce alliances for the health navigator professions, are among the considerations that may be conducive to building successful programs. For example, colleges with existing nursing, EMT, and human services programs may find “win-win” opportunities for expanding existing college partnerships that provide opportunities for health navigator students, and cost-effective workers for employers. Similarly, colleges can hire program directors or key faculty that bring their own professional connections.
While the survey did not directly illuminate potential barriers to successful program development, write-in feedback from survey respondents suggests two potential challenges, which potential future adopters should consider. First, related to those students who seek to enter the workforce directly, there were some mixed perceptions of the necessity for 2-year degrees. While not negating the value of credit-based (as opposed to noncredit) certificates that can articulate with 2- and 4-year degree opportunities for future development, write-in survey feedback suggested that in some cases, the current salary range for CHWs does not justify making a 2-year degree the standard of practice for working in the community.
The second potential barrier affecting associate-level program development relates to state-specific legislation concerning CHW certification. While a minority of U.S. states currently have state-mandated certification practices, those states stipulate certificate-level training for CHWs working in the community. It will therefore be important for community colleges in those states to create certificate- and associate-level programs that complement existing state requirements. Based on existing program models throughout the United States, one option in these contexts may be to include both certificate- and associate-level academic options to give students additional options.
Limitations of the Study Design
It is important to acknowledge that while the survey provides useful insight into the perspectives of community college leaders toward the adoption of health navigator training programs, the findings may not be representative of the broader community college population, or to health navigator training in other settings (such as workplaces or training centers).
The aim of the survey design was to accurately measure the intended content areas and concepts, and to yield consistent results that could be replicated if the survey were to be re-administered within the same sample of respondents (Creswell, 2014; Newcomer, 2011). However, as the survey sought to collect new knowledge on formal academic training programs for the health navigator professions, and as these professions are quickly emerging and evolving, it is possible that certain survey measures were operationalized inappropriately. To address these concerns, the following steps were taken: (1) The survey was developed with feedback from subject-matter experts on survey content and the appropriateness of questions. (2) All potentially unfamiliar terms were defined in the survey instrument, and multiple examples were given of potentially ambiguous concepts, such as the professional titles which could be associated with health navigator-type training programs. Numeric Likert-type scales were also used in place of ordered adjectives like “good, better, best” to address related measurement reliability issues. (3) The survey was also pilot-tested in the community college environment to ascertain if end users in the target population interpreted specific questions as intended. (4) Respondents were given an opportunity to refrain from answering survey questions with a “don’t know” option, which may help address inappropriate operationalization, but also addresses other measurement validity concerns such as accidental misrepresentation.
Another concern in this survey-based design is the possibility of selection bias and nonresponse bias. The following steps were taken to mitigate this concern: (1) The survey sample was selected from League and non-League members alike, to increase the number and diversity of respondents from around the country invited to take the survey, and to address potential inherent differences between League and non-League members. (2) The survey invitation and follow-up emails during the open period were sent under the auspices of the League, in an effort to encourage survey participation within this sample. The invitations also included background information, a website link for more information, and information about the professional endorsements and interest from reputable sources, once again in an effort to increase the likelihood that individuals in this sample would agree to take the survey. (3) The subgroup analyses described above, including data from the targeted follow-up effort with nonrespondents, were conducted to ascertain if respondents within this sample varied on key variables. While the online response rate was relatively low, this low response rate is less of a concern, because these analyses showed no statistically significant variation between online survey respondents and those participants who were reached through targeted follow-up efforts. The fact that only 25 individuals were reached after extensive follow-up efforts suggests that these individuals may simply be more difficult to reach, instead of statistically different in their response patterns to the survey. While the possibility of validity concerns can never be fully removed, these issues are less concerning in light of the findings of the subgroup analyses.
Although the findings of this study may not reflect the broader community college audience, this research provides promising data on the growing role of community colleges in health navigator training. For community college leaders beginning the decision process about whether to adopt new health navigator programming, this research provides insight into key factors that may help to make new programs successful. As community colleges become more fully integrated into the continuum of public health education, it is hoped that health navigator training programs can provide opportunities for students to begin their academic and professional journey, fill local workforce needs, and help to address enduring health disparities through their work as in the community.
Footnotes
Acknowledgements
The author gratefully acknowledges the valuable feedback on this research provided by Richard Riegelman, Cynthia Wilson, Kathryn Newcomer, and Yuyi Chen.
Authors’ Note
The contents of this article are solely the responsibility of the author and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Association of Schools and Programs of Public Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported under a cooperative agreement from the Centers for Disease Control and Prevention through the Association of Schools and Programs of Public Health, Grant Number 5U36OE000002.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.