
Abstract
The community-based participatory research (CBPR) approach can be an innovative and effective way to address health disparities. Doctoral students in the health sciences can benefit through structured CBPR training experiences in learning how to engage with communities, build community capacity, share resources, and implement CBPR studies. The objectives of this case study are to demonstrate ways in which one doctoral student aligned with academic mentors and a funded CBPR project to develop and implement a CBPR-focused doctoral dissertation study. The student partook in formal and informal CBPR learning experiences, built community and academic relationships, developed a research plan in collaboration with members of the community/academic partners, identified an appropriate setting and methods for recruitment/data collection, and increased the capacity and resources for all partners (the first author, community, and academic). In conclusion, CBPR-focused doctoral experiences are novel, pedagogical, and professional approaches that can lead to successful and effective community-based health research.
Keywords
Background and Significance
Community-based participatory research (CBPR) has been demonstrated to be an innovative, practical, and successful way to address complex community health problems and health disparities among ethnic minority groups (Israel et al., 2006; Trinh-Shevrin et al., 2007). CBPR may be of particular interest to health science doctoral students who value social justice and are interested in a dynamic and action-oriented way to address health disparities and community health–related issues. Although there have been significant efforts to provide CBPR training to physicians and research investigators (Dalal, Skeete, Yeo, Lucas, & Rosenthal, 2009; Golden et al., 2014), little is known about how graduate students, specifically doctoral students, can apply these principles to a CBPR dissertation study and how that contributes to the development of professional and research skills as well as positive community outcomes.
There are multiple advantages for doctoral students who utilize a CBPR approach. These include an enhanced understanding of health issues salient and meaningful to communities, early skill development in learning how to design studies incorporating community input, and ways in which longer-term community relationships can facilitate studies of high quality and significance. Despite the potential benefits of training and immersing doctoral students in the CBPR approach, there is little data on how doctoral students can implement CBPR principles into their dissertation study plans. Therefore, the current case study builds on the CBPR-oriented training experiences of other health professionals (academics, physicians) as documented in the literature (Dalal et al., 2009; Golden et al., 2014; Khobzi & Flicker, 2010) and may provide innovative CBPR instruction–related ideas for doctoral students, academics, and communities.
Objectives
We use a case study approach to (1) describe how one doctoral student incorporated the CBPR approach into the development and implementation of her dissertation study and (2) describe how this educational activity benefitted the student, the community partners, and the academic partners of a CBPR study.
Initiating Contact With CBPR Researchers
The first step of a CBPR doctoral training experience can begin with choosing an advisor or organization that has expert CBPR knowledge and active, funded CBPR studies (Khobzi & Flicker, 2010). Attempting a CBPR-focused doctoral study can be challenging independent of academic mentorship and should ideally be facilitated by advisors who are immersed and experienced in the approach (Ahmed, Beck, Maurana, & Newton, 2004). Although it was extremely beneficial for the doctoral student to be linked with an advisor affiliated with CBPR projects, there may be alternative ways to initiate CBPR-oriented dissertation studies. For example, students may gain access to CBPR projects through community partners. Or students may seek out academic CBPR mentors in other institutions of higher education (Ahmed et al., 2004).
The ways in which faculty members can enable CBPR-oriented doctoral studies are summarized in Table 1. In this case study, the first author (doctoral student) identified an advisor who was connected to a funded and successful CBPR project. The advisor is an investigator with the Center for the Study of Asian American Health and introduced the first author to the principal investigators of several ongoing studies within the Center. One of the main Center studies is the New York University School of Medicine Prevention Research Center’s Project RICE (Reaching Immigrants through Community Empowerment) focusing on cardiovascular disease and diabetes among the South Asian community. Established in 2007, this CBPR study emerged as a coalition between academic partners and community partners (including social service agencies, advocacy groups, and health care providers) serving the South Asian community. After jointly conducting a series of needs assessments in the South Asian community, the coalition identified cultural and linguistic barriers to diabetes and cardiovascular disease prevention and management as major concerns for this population and worked together to seek and obtain funding, implement, and evaluate a diabetes prevention intervention. There were several South Asian American community partners associated with this project, and the first author was able to attend community–academic partnership meetings, volunteer for research-related activities, and build relationships with South Asians associated with Project RICE.
Faculty Mentor Responsibilities in Facilitating CBPR–Focused Doctoral Studies.
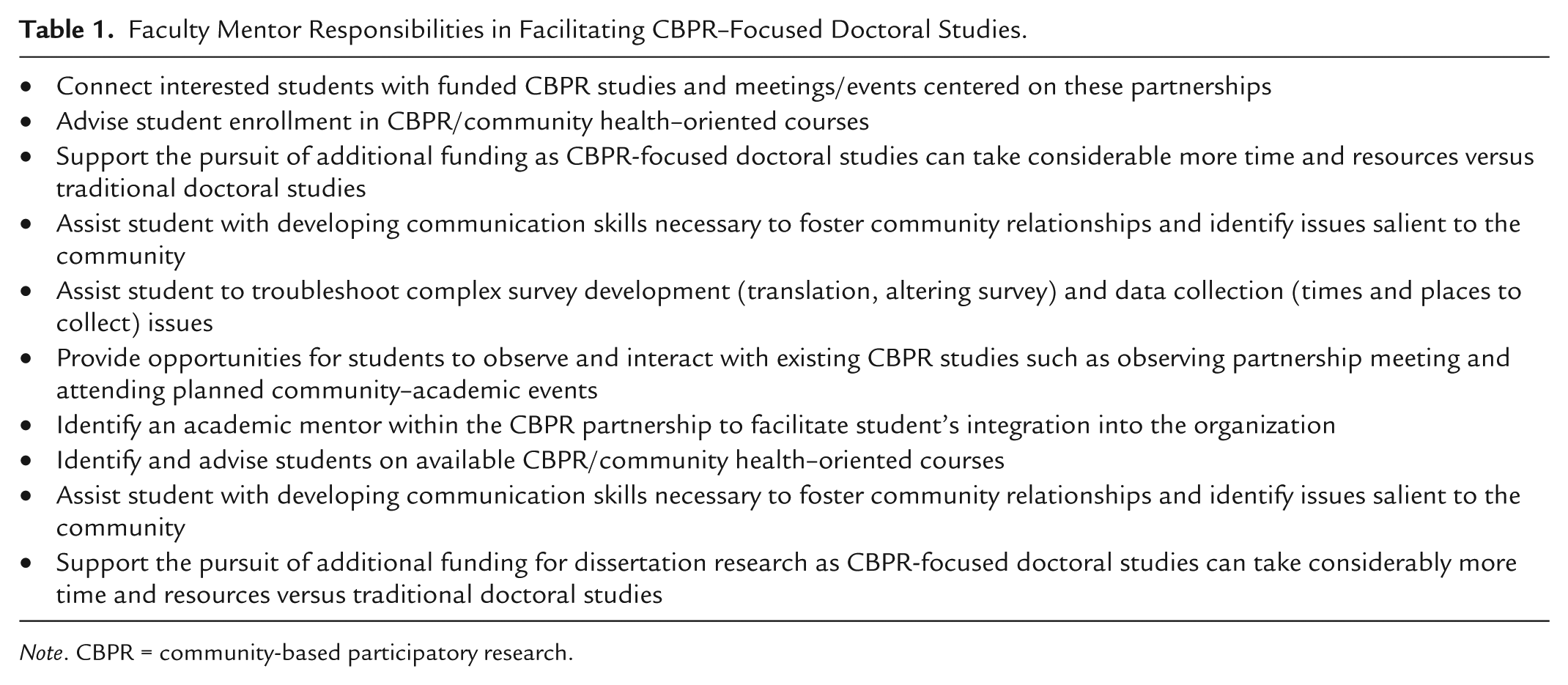
Note. CBPR = community-based participatory research.
Didactic and Academic Exercises
While establishing relationships with academic and community partners of ongoing CBPR projects, doctoral students can simultaneously enroll in CBPR classes and develop an intellectual grasp of CBPR principles. In this case study, the first author learned CBPR principles through intensive one-on-one guidance from her CBPR research mentor and engaged in coursework where CBPR methodology and studies were discussed. Another practical experience that led to the development of the first author’s research plan was that completing her PhD required teaching residency in which an introductory level CBPR workshop for students, clinicians, and academicians of the New York University health studies community was developed. This online, web-based day workshop included several CBPR-oriented modules and provided necessary pilot data that were integrated into the wider curriculum of an interdisciplinary New York University CBPR course.
Method
As a result of connecting with a CBPR research team as well as independent didactic studies, the following steps were followed in developing the first author’s doctoral dissertation study:
Early relationship building: colearning and mutual benefits
Development of a research plan and community input
Establishing a setting, recruiting, and collecting data with CBPR
Capacity and resource building
Follow-up/sustainability beyond the dissertation study
Early Relationship Building: Colearning and Mutual Benefits
Early relationship building between academic and community partners is essential to building trust, facilitating communication, and establishing rapport with the members of a CBPR team (Islam, Kwon, Ahsan, & Senie, 2005; Savage et al., 2006). To build important relationships early on, the first author attended several coalition meetings and volunteer events to better understand the needs and issues of the Sikh Asian Indian (AI) community in New York City. For example, when one of the Sikh AI community partners received a national recognition, the first author was present at the ceremony to celebrate the significant achievement. Simultaneously, the coalition learned more about the first author’s doctoral study interests. These early relationship-building activities occurred over a 2-year period before the first author developed her dissertation study with the Sikh AI community. As a result, the first author gained invaluable knowledge and insight into the health challenges, struggles, and triumphs experienced by this community, which ultimately contributed to the joint identification of a doctoral dissertation topic for the first author.
Relationship building and colearning experiences shared between the community partners and the first author resulted in benefits for both sides (Minkler & Wallerstein, 2008). The first author volunteered her nursing services, and recruited other health volunteers including physicians and other nurses, to provide health services at various community partner health screenings. As a result, the first author developed a first-hand, enriched understanding of her dissertation topic. An early relationship with a community leader also led to collaborating on the writing of this article of which the community leader is a coauthor. In sum, relationships built early on led to the exchange of information and, ultimately, the sharing of benefits between the first author and the community partners.
Development of Research Plan and Community Input
Doctoral dissertation plans can be enhanced and more salient when incorporating the input of knowledgeable community members (Khobzi & Flicker, 2010; Minkler & Wallerstein, 2008). The first author was initially interested in the topic of interpersonal discrimination, or unfair treatment as typically based on race (Williams, Yu, Jackson, & Anderson, 1997), and how it may be related to the health of South Asians. Although a formal review of the literature signified a gap in this research area (Nadimpalli & Hutchinson, 2012), the first author was able to achieve firsthand knowledge about experiences related to discrimination from Sikh AI leaders at the partner agencies and incorporate this knowledge into the development of her dissertation study. Specifically, the first author met with several community leaders and asked them to describe their experiences with discrimination and how they coped with such experiences. The CBPR approach helped inform the development of the doctoral dissertation question: What are the relationships between discrimination and the health of South Asian Americans? As well as the aims of the study: to explore self-reported discrimination as measured by the Everyday Discrimination Scale (Williams et al., 1997) in relationship to several physiological (blood pressure, body mass index, waist-to-hip ratio) and self-reported mental and physical health outcomes (Ware et al., 2007). Community partners agreed that stress theory should provide the framework for the study in that chronic exposure to discrimination over the life course may trigger stress-related physiological health responses and result in poorer health (McEwen, 2004, 2005). Coalition partners were consulted when designing the study and for how it might be best to carry out the aims of the study. Key academic partners also helped facilitate dialogue with the community partner agencies and assisted with developing a recruitment strategy with Sikh AI partners. The New York University School of Medicine approved the Full Board Expedited Review Institutional Review Board application. Working with the coalition in developing the dissertation taught the first author how to include community input in all phases of development, from the research question to study design, and resulted in constructing a highly relevant study plan.
Survey Development
The survey development aspect of a CBPR-oriented dissertation study can also be enhanced through incorporating community knowledge and skills (Minkler & Wallerstein, 2008). The first author’s dissertation survey was developed in close collaboration with the coalition partners months prior to recruitment and data collection. First, major issues were identified; second, the first author compiled potential survey questions based on existing, validated constructs/measures; third, a review of potential measures was discussed with partners; and finally, the survey incorporated unique issues highlighted by partners. For example, several community partners stated that they believed that they experienced discrimination based on the way in which they spoke English (with an accent). Therefore, the first author included a survey item assessing whether participants felt that they were discriminated based on the way they spoke. The length of the survey also appeared daunting to many community participants, and therefore, the survey was shortened based on this feedback. Three community members pilot tested the survey, and the first author added a survey question based on feedback from the community members.
Given the high rates of limited English proficiency among the target population, the survey was translated into Punjabi and ultimately reviewed and approved by the community partners. Translation of the survey into Punjabi was a labor-intensive undertaking that involved surmountable networking and persistent efforts to find willing and capable translators. However, the first author was committed to translating the survey into Punjabi language as it would result in including a more broad and diverse sampling frame. Including questions relevant to the Sikh AI community and efforts to translate the survey promoted CBPR values of respect and inclusion (Minkler & Wallerstein, 2008).
ACASI has been found to be an extremely beneficial survey mode across several different ethnic groups, especially when surveying on sensitive topics, such as discrimination (Jones & Jedrasik, 2000). In the dissertation study, ACASI was used to maximally accommodate English- and Punjabi-speaking and reading Sikh AIs. Participants could choose either the English or Punjabi version of the survey in which survey questions were written out and read aloud through headset in the language of their choice. Answering ACASI questions involved minimal computer skills, such as moving a computer mouse to the desired response and clicking that response. The 69-question survey took the participants approximately 21 minutes to complete.
The use of ACASI reduced threats to validity related to response bias, skipping questions, and the ability to answer sensitive questions more honestly (Jones, 2003). The ACASI survey methodology has also been found to be a relatively straightforward, efficient, and user-friendly way to survey those who have lower literacy rates and writing skills (Jones, 2003). Therefore, the use of ACASI led to robust survey design and simultaneously facilitated sensitivity and respect toward the needs of the Sikh AI community.
Establishing a Setting, Recruiting, and Collecting Data With CBPR
Choosing a research setting that community members are comfortable and familiar with is a key way to fulfill CBPR principals of respect and incorporating community input. Community members can offer valuable input on when, where, and how a dissertation study can be most successfully implemented (Islam et al., 2005; Wang-Letzkus, Washington, Calvillo, & Anderson, 2012). After consulting with coalition partners regarding recruitment into the study, it was suggested that the ideal places to carry out data collection for the dissertation study would be at community centers that Sikh AIs frequent. Additionally, given the tremendous amount of language, ethnicity, and religious diversity among the South Asian community, the benefits of focusing on a particular language or religious groups became apparent. Consequently, data collection and recruitment occurred at two South Asian faith-based organizations in the Richmond Hills, Queens, New York City area serving a largely Punjabi-speaking, Sikh AI community. Dates and times that ideally accommodated the participants were also established by the community members. Following input from coalition partners, a $10 incentive was offered to participants to participate in the study. Ultimately, the number of participants who completed the study exceeded the original power requirements set forth in the dissertation plan. Recruitment and data collection were facilitated by accommodating participants in an environment in which they felt comfortable and by modestly incentivizing participation. Thus, participant satisfaction and dissertation implementation success can be substantial benefits of using the CBPR approach.
Capacity and Resource Building
CBPR is conceptualized as a colearning process where academic and community partners bring their unique skills sets and resources to a project (Islam et al., 2005; Minkler & Wallerstein, 2008; Trinh-Shevrin et al., 2007). Throughout the development of this dissertation study, there were instances of capacity and resource building that benefitted the first author, the community partners, and the academic partners as well. Thus, all parties received additional benefits compared with working on their projects in isolation. For example, developing the dissertation survey with those in the Sikh AI community provided an enriched understanding of the problem. The first author was also able to lead focused, productive data collection events based on advisement from both academic and community partners. In the survey development phase, the first author was able to share information on translation and ACASI resources as a result of the numerous hours spent on investigating and securing professional Punjabi translators and an ACASI programmer for the dissertation study. The first author’s volunteer efforts as a health professional, and the recruitment of other health professionals to assist in the health screening activities (blood pressure, weight, glucose measurements) at various Sikh AI events, was another way in which community capacity was enhanced. In summary, the development and conduct of this dissertation study involved resource sharing and capacity building between the first author, the community partners, and the academic partners (Minkler & Wallerstein, 2008).
Follow-Up on Results and Sustainability Beyond the Dissertation Study
Another hallmark of the CBPR approach is to ensure that study participants have access to study findings and opportunities to share their opinions on them (Minkler & Wallerstein, 2008). Therefore, the first author invited the community partners to the dissertation and public defense. In addition, the first author attended the two Sikh gurdwaras where data collection/recruitment took place and presented study findings through distributing a flyer with study results and small group presentations. Several small groups consisting of approximately 10 people listened to the author describe the study findings, read the flyer with study results, and shared their thoughts and ideas regarding the study.
Sustainability is another important consideration in the CBPR process (Islam et al., 2005). However, there has been little published on how partnerships between doctoral students, community, and academic partners can be sustained. The first author plans to continue to pursue studying the social determinants of health and how they may adversely affect the South Asian and other ethnic minority communities. The first author also plans to work with Sikh community members to disseminate results as a community brief/policy report that can be used by partner agencies in policy and advocacy efforts.
Summary
Doctoral students who are able to secure academic mentorship in CBPR and align with funded CBPR projects can partake in experiential learning in developing their dissertations. Doctoral students can actively incorporate CBPR principles into their research through relationship building, colearning and the sharing of benefits, developing a research plan, recruiting and collecting data, expanding capacity and building resources, and following-up with communities. Specifically, the first author began building relationships with the community early in her doctoral career (Year 1) through volunteering and attending community meetings. Recruitment and data collection for the dissertation study took place in community spaces that were comfortable and familiar for the participants. The dissertation study survey was developed and adjusted in consideration of community needs and desires. Community and academic partners facilitated many learning experiences for the first author, and the first author was able to share translation and volunteer resources with the CBPR partnership as well. Finally, the first author plans for an ongoing relationship with the community surveyed. Although there were several fruitful and rewarding aspects to the first author’s CBPR-oriented dissertation, there were many challenges encountered and are summarized in Table 2.
CBPR-Oriented Doctoral Study Challenges.

Note. CBPR = community-based participatory research; ACASI = audio computer-assisted survey interviewing.
Informal evaluations of this case study may include acknowledgment of the successful defense of the first author’s dissertation study, expressed satisfaction by research participants, and the ongoing, positive relationship the first author has with the partners of the CBPR project. However, a recognized weakness of this CBPR-oriented dissertation case study is its lack of formal evaluation. Future collaborations between doctoral students and CBPR coalitions can more formally examine the benefits and efficacy of such partnerships through pre- and posttest surveying of doctoral students and academic and community partners.
In sum, doctoral students can benefit greatly from CBPR immersion experiences, and in turn, these experiences can benefit academic partners through having an added academic resource and the potential to build capacity. Communities can ultimately benefit through having access to additional resources, potential advocacy studies, and meaningful, sustained relationships. Therefore, it is recommended that interested doctoral students pursue and academic advisors facilitate CBPR-oriented dissertation studies to ensure the future of novel and effective community health research and interventions.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was primarily supported by the National Institute of Nursing Research Ruth L. Kirschstein National Research Service Award for Individual Predoctoral Fellows in Nursing Research (1F31NR013830-01A1) and an American Nurses Foundation 2013 Nursing Research Grant. This work was partially supported by the following research grants: P60MD000538 from the National Institutes of Health, National Institute for Minority Health and Health Disparities; UL1 TR000038 from the National Center for Advancing Translational Sciences, National Institutes of Health; and 1U48DP001904-01 from the Centers for Disease Control and Prevention; and The National, Heart, Lung, and Blood Institute of the National Institutes of Health under Award Number T32HL069771.