
Abstract
The Affordable Healthcare Act has, among other changes, created greater incentives to reduce health disparities in low-income communities across the country, which heightened the importance and expectations of community health workers (CHWs) as part of the clinical care team. These heightened expectations have begun to transition what has historically been a paraprofessional role into one that involves more clearly defined competencies and development needs. In an effort to meet these needs in the city of Chicago, a CHW basic certificate program was developed and launched at Malcolm X college (one of the seven city Colleges of Chicago), in collaboration with several community partners. This article presents the experience of this program, the challenges faced in its implementation, and lessons from this experience that may be relevant to others involved in the professional preparation of CHWs.
Several trends in the United States are leading to a greater recognition of the important roles community health workers (CHWs) need to take in order to improve public health, as well as heightened expectations of people who take these roles. In this article, we describe our experiences developing and launching a formal academic program to enhance CHW skills. While the launch was successful in many respects, we experienced several important challenges. By sharing this experience, we hope to better equip other educators who may pursue similar programs in their own communities.
The role of CHWs in health care is receiving greater attention in recent years due to the introduction of the Affordable Care Act, which has allowed millions of uninsured adults to receive health care coverage. The legislation also offers incentives to health systems for improving the patient care experience and population health, as well as reducing the per capita cost of health care (McNeill et al., 2015). To achieve these goals, many health systems have begun to enlist CHWs, whose close community connections can be leveraged to help enroll new people into insurance products as well as better engage them in their own care (e.g., Blewett & Owen, 2015; Rosenthal et al., 2010; Uriarte, Cummings, & Lloyd, 2014).
There are an estimated 48,130 individuals in CHW roles across the United States, and these numbers are expected to grow 15% from 2014 to 2024, faster than the average for all occupations, according to the Bureau of Labor Statistics, U.S. Department of Labor (2015). The growth of numbers as well as the importance of the CHW have led to national efforts to raise its visibility and clarity.
The American Public Health Association (2015) has developed a standard definition for a CHW as follows: A community health worker is a frontline public health worker who is a trusted member of and/or has an unusually close understanding of the community served. This trusting relationship enables the worker to serve as a liaison/link/intermediary between health/social services and the community to facilitate access to services and improve the quality and cultural competence of service delivery.
A CHW also builds individual and community capacity by increasing health knowledge and self-sufficiency through a range of activities such as outreach, community education, informal counseling, social support, and advocacy (American Public Health Association, 2015).
CHWs in the State of Illinois
The role of CHWs as members of the care team was formally recognized recently in the state of Illinois, by House Bill 5412, which was signed into law in July of 2014. The bill recognized a set of competencies associated with CHW practice and called for the establishment of an advisory board to recommend rules to standardize the criteria and process to become a certified CHW (Illinois General Assembly, 2014). This provision opened the door for Illinois community colleges to develop new educational programs for CHWs. The opportunity found further support through a grant to Rush University Medical Center from BMO Harris Bank to accelerate partnerships for workforce development between Rush University Medical Center, Malcolm X College, and the Medical Home Network. The program, “Building Health Urban Communities,” was established to support the development of new and sustainable models of health care delivery that would address the care needs of underserved Chicago communities (American Hospital Association Community Connections, 2015). The architects of the projects recognized the critical role CHWs could play in these efforts and allocated a portion of the support for developing formal educational programs for CHWs.
Malcolm X College (2015), one of the seven public City Colleges of Chicago, was identified as an appropriate home for a new program addressing the learning needs of these emerging CHW roles. In addition to its proximity to Rush University Medical Center, Malcolm X College had recently been designated a health sciences focused college and was undergoing an expansion in health care career programs and a new multimillion dollar facility. The grant provided support for a team of Rush University Medical Center and Malcolm X College faculty to initially develop a basic certificate program for CHWs, and then to expand the program to include advanced certificate and associate degree offerings, creating milestones of educational attainment for CHWs as well as a pathway toward higher levels of education over time.
Program Development
A recent national study of CHW education at community colleges found that most of these programs are relatively new—indeed, over half were less than 2 years old (Johnson, 2016). The majority of these programs were limited to the academic (credit-based) certificate level, principally because there was not enough research to support the need for a degree in the field. For similar reasons, we started CHW education at Malcolm X College with just the launch of a basic certificate program, with an eye toward expanding programming once the career-related value of additional education could be clearly demonstrated.
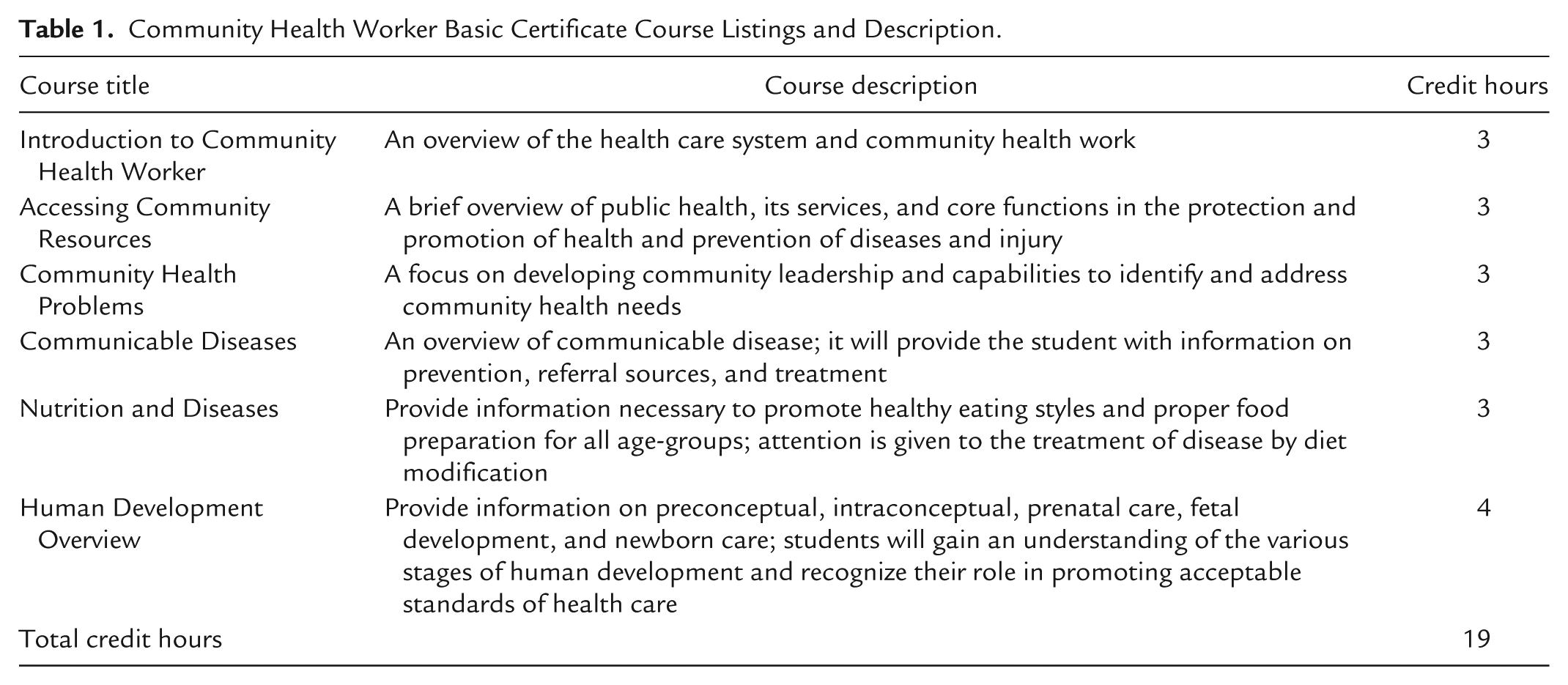
To develop the curriculum for the CHW basic certificate program, we started with a curriculum originally developed in August 2002 for use at another Chicago City College, based on assessments from working CHWs at 25 social and health care organizations. The draft curriculum was also systematically reviewed by experts and advisors from a variety of health care and social service organizations, including the Chicago Department of Public Health as well as two graduate colleges of nursing. Table 1 provides a list and description of the courses offered in the original basic certificate curriculum.
Community Health Worker Basic Certificate Course Listings and Description.
To update the original curriculum, we conducted interviews and focus groups with staff from local clinics and nonprofit agencies that use CHWs on the South and West side of Chicago. The settings these CHWs worked in included public health departments as well as community centers, such as the Englewood Neighborhood Health Center, Lawndale Christian Health Center, and Rauner Family YMCA of Metro Chicago. We conducted semistructured interviews with each of the CHWs to collect input on each of the following areas: current job responsibilities; knowledge, skills, and prior experience required for the role; and any educational requirements. A total of 20 CHWs were interviewed during this step of the process.
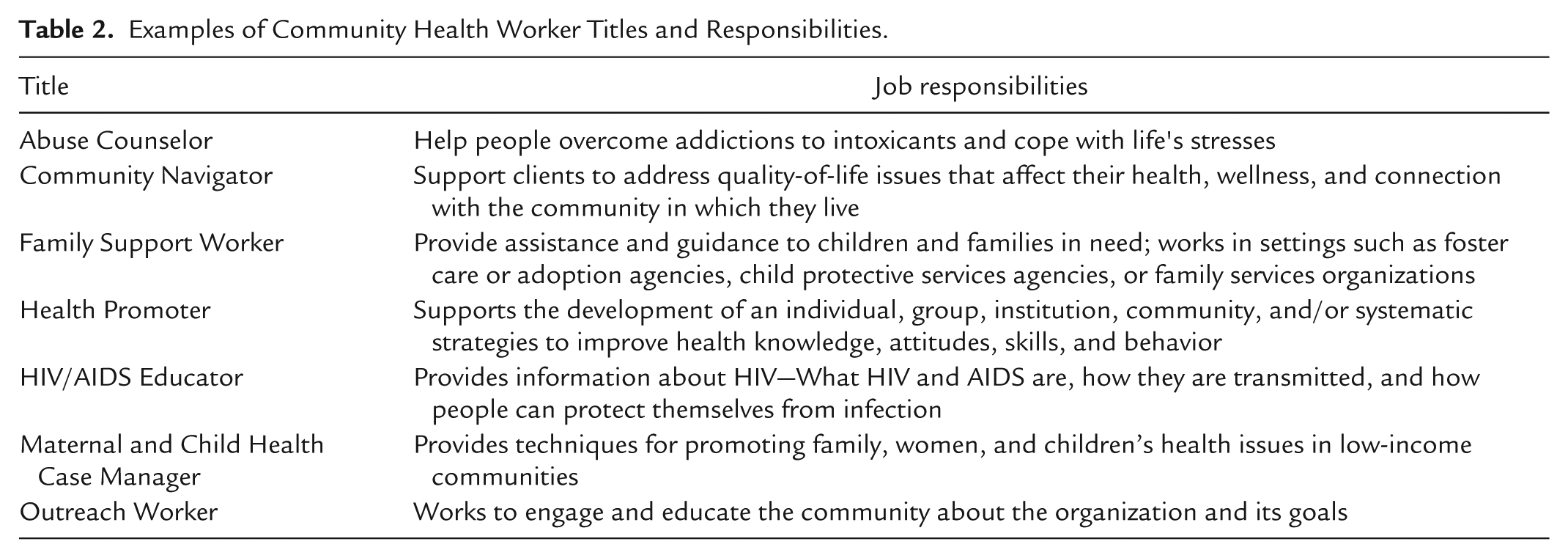
Through this process, we came to appreciate not only how varied the CHW roles were but also how many job titles were being used for these roles. For example, CHWs were classified as Communicable Disease Investigators at one health center and as Patient Navigators at a neighboring center. Table 2 provides examples of different titles and responsibilities we identified in this process.
Examples of Community Health Worker Titles and Responsibilities.
The focus group included CHWs, supervisors of CHWs, managers of organizations employing CHWs, and other individuals who work with CHWs. We provided the student learning outcomes and course objectives for the CHW curriculum to focus group participants in a checklist format. Participants in the focus groups were asked to assess the importance of each curriculum component, and provide any open-ended feedback that might be helpful. This feedback helped us ensure that the program’s learning outcomes were well aligned with the CHWs’ day-to-day responsibilities. For example, feedback from the focus group suggested that the curriculum should include a greater orientation toward working effectively in a team, as well as provide the computer skills necessary for tracking and analyzing client and performance information.
Once we revised the curriculum in light of the focus group feedback, we were ready to move forward with implementation of the CHW program. To select appropriate course materials, we conducted an extensive search for all of the CHW programs we could find across the country, and then reviewed their selection of books, materials for courses, and qualifications for instructors to teach in the program. This review helped us identify an appropriate core textbook and also suggested to us that the instructors we had identified would be appropriate for these new instructional roles.
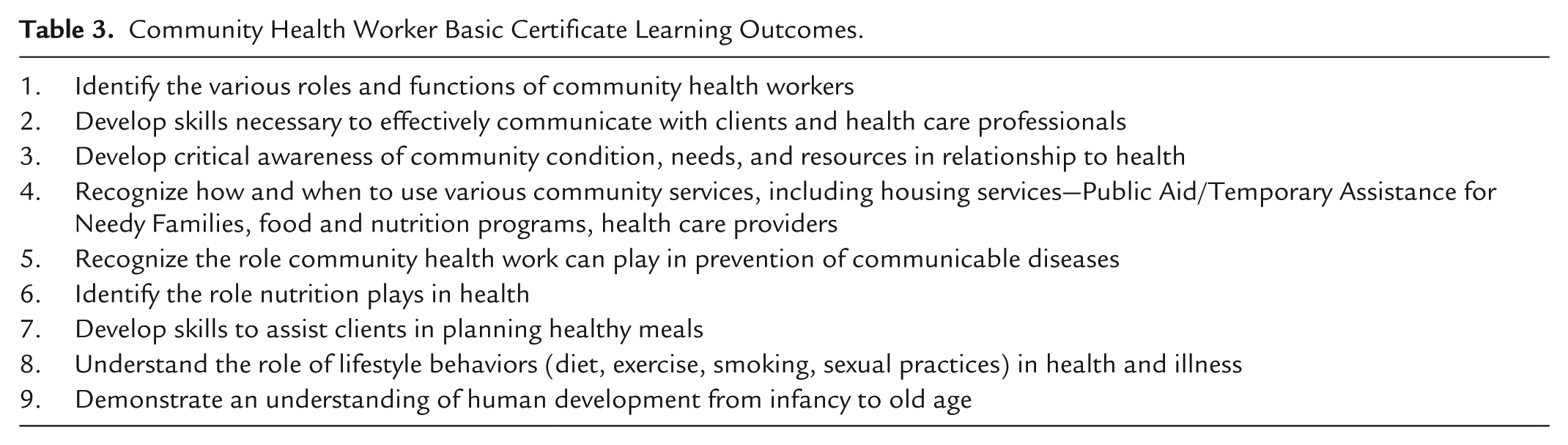
The overall goal of the CHW basic certificate program is to give each student a background in essential knowledge and competencies required for primary and preventive health care as a CHW. The curriculum focuses on student development in the following areas: health education, health promotion, knowledge of community services, effective communication, advocacy, cultural competence, and professionalism. The CHW basic certificate program is composed of 6 courses totaling 19 credit hours. In Table 3, we list the student learning outcomes for the CHW basic certificate program.
Community Health Worker Basic Certificate Learning Outcomes.
Program Outreach
To market the CHW program and garner enrollment, we distributed marketing materials to local clinics, hospitals, and community-based organizations. To extend our outreach, we also attended meetings conducted by the local CHW network in Illinois. Our greatest success came from partnerships we developed directly with the employers themselves. In particular, the community center agreed to enroll a number of their current CHWs in our first cohort for the CHW program. The community center provides treatment for HIV and AIDs patients with the utilization of patient navigators. Patient navigators are often characterized as a form of CHWs given the scope of their work.
Program Implementation
We enrolled our first cohort into the new CHW program in the fall of 2014. A total of nine students enrolled in the new, 19–credit hour basic certificate program, which was designed to be completed over a two- to three-semester period. Each semester at Malcolm X College is equivalent to 16 weeks. In the interest of piloting the program carefully, we began the first semester with a single course offering, the “Introduction to Community Health Worker” course. In the second semester, three courses were offered, and in the third semester, two courses were offered.
All courses took place during evening hours, and all nine students were working in a CHW capacity, either in a paid position or as a volunteer. A grant provided by the Illinois Department of Public Health to the community center provided funding for tuition, books, and fees, so that all the 9 students had minimal out-of-pocket costs.
Outcomes
From the original nine students who were in the cohort, four (44%) continued with the program to completion of the basic certificate. This completion rate compared very favorably to college-wide for the comparable period (City Colleges of Chicago, 2015). Of the five students who did not complete the program, three reported experiencing barriers due to family obligations, changes in work schedules, and/or personal reasons unrelated to school. The remaining two students returned to the program in the summer semester of 2015 to continue their certificate training but still have a few classes to complete at this time.
The four students who were successful in completing the basic certificate attributed their success to utilization of support resources such as the Level Up program (City Colleges of Chicago, 2015), dedicated instructors, and support staff. Several quotes from students during an exit interview were illustrative. One student said, “This class has encouraged me to continue to learn about other cultures and the disparities people face each day of our lives. I hope to go on to new levels of advocacy for people and communities.” Another student stated, This has been a learning experience for me. I never really thought I would attend college, but I am here and this was one of the best decisions I have ever made. Our professor is a wonderful educator. Thank you.
The students’ feedback spoke to the success of the program in terms of building a valuable educational experience that the students can use in their field of work.
Despite its early success with respect to program completion, the program was placed on hold after the first cohort completed the program, due to a lack of concrete data substantiating the job prospect for titles associated with CHWs in the Chicago land area. Plans to relaunch the program are under way as City Colleges of Chicago is seeking commitments from employee partners for CHW roles in the near future.
Challenges/Lessons Learned
One of the most crucial lessons we learned from the launch and discontinuation of the program was the importance of understanding how educational programs in the community college system are evaluated. The College to Careers initiative was designed to provide students with credentials of economic value and employability. Each program annually goes through a systematic review based on job outlook, accrediting body requirements, enrollment trends, and employer demand. Although the Affordable Care Act and local legislation implied that the CHW profession was likely to grow, we were not able to secure specific estimates of job needs from our community partners and other local employers. With the lack of confirmed job prospects and labor market statistics for the CHW profession, enrollment for the CHW program was limited to existing CHW workers only for the first cohort. There was consideration given to identify by what method the CHW certificate credential could align with other disciplines at community college to receive stackable credentials; however, there was no definitive congruency aligning CHW learning outcomes with those of the other professions. Without the ability to demonstrate specific hiring needs for graduates or a clear alignment to higher education pathways, college leadership decided we would need to postpone future offerings of the program until more concrete demand data were available.
Another important outcome community colleges track is career progression. Although our community partners consistently expressed interest in opportunities for their CHWs to expand their skills, the higher skill levels provided by the Basic Certificate program were not associated in any specific way with a career path for the enrolled CHWs. The success of the college under the City College of Chicago system was judged heavily on its success in moving students out of unemployment and into gainful employment, as well as moving students into higher levels of education. Because many of the students enrolled in the program were already working, their skill development, while important to the public health goals of the project sponsors, was not as well aligned with the employment goals of the College.
In addition to the importance of outcomes, we also learned the importance of consistent leadership to the success of new programs. As a low-enrollment pilot program, the CHW program did not have a dedicated program director, which created confusion regarding roles and responsibilities associated with program implementation and management. Without a dedicated program director to assist with recruitment, class scheduling, financial aid assistance, faculty assignment, and/or ordering of books, many of these core responsibilities were split among project participants, creating coordination challenges. Much of the efforts to coordinate the program were led by people who were often unfamiliar with the requirements and expectations to successfully conduct the program.
A final lesson learned related to how we developed relationships with the employer community. In the beginning, we established a committee to review the curriculum and outcomes for the program comprised of organizations that hire CHWs, supervisors, and people who work as CHWs. However, we did not maintain ongoing communication with the advisory committee once the program was launched. Regular communication with the advisory committee could have helped us improve numbers in recruitment and build more connections to possible job openings for the students in the program.
Conclusions
As health reform continues to change the health care employment landscape, it will be important for higher education institutions generally, and community colleges in particular, to continue monitoring these changes to ensure their portfolio of educational programs remain current to these evolving needs. It is also important to gauge timing of new programs, so that graduates of these programs can be assured they are entering a job market with needs that match their educational accomplishments. By providing the case study of community college’s CHW program, we hope to assist other educational program leaders in considering some of these complex issues as they prepare their own programs to meet these changing needs.
Footnotes
Authors’ Note
The content of this article is solely the responsibility of the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the Building Healthy Urban Communities Project funded by BMO Harris Bank.