
Abstract
Public health–related decisions are influenced by a variety of actors operating on local to global levels, including community leaders, educators, nongovernment organizations, government officials, donors, and researchers, many of whom may lack formal public health training. The provision of public health instruction to interdisciplinary professionals has the potential to strengthen the capacity of all stakeholders to make informed, evidenced-based decisions about health policies and programs. The use of online learning is emerging as a promising means of providing public health training, particularly among those living in geographically disparate areas and from multidisciplinary backgrounds. This article describes an online course created to teach participants in stakeholder teams from 14 low- and middle-income countries how to design and conduct qualitative research to understand girls’ challenges managing menstruation at school. The goal of the course was to strengthen each country team’s ability to conduct research by building the capacity of the members. Thus, completion of the course by all team members was an objective, but less of a focus than assuring that each team as a collective was gaining public health insights and working together to make informed decisions about their research goals. This course led to benefits beyond capacity strengthening, including the formation of a broader community of learning and practice that extended beyond country boundaries. We recommend embedding training opportunities for multidisciplinary stakeholders into research endeavors given the potential for positive effects on individual participants and overall policy decisions to improve community health and provide lessons learned for doing so.
Introduction
Public health–related decisions, including the development of policy, allocation of funding, and the development and dissemination of support programs and services, are influenced by various actors operating on local to global levels, including community leaders, educators, international and local nongovernment organizations (NGOs), government officials, donors, and researchers. This diversity of perspective is integral to solving complex public health problems (Albrecht, Freeman, & Higginbotham, 1998). While the diversity of perspective, background, education, and experience is critical, public health or related training can specifically enable stakeholders to rigorously assess the contribution of available evidence, how it was obtained, and if further research may be warranted.
Furthermore, the provision of public health instruction to multidisciplinary teams, including those with and without formal public health backgrounds, has the potential to create opportunities for collaboration, enable the exchange of ideas from varied perspectives, catalyze movement on a common agenda from multidisciplinary ends, and build or strengthen the capacity of stakeholders to make informed, evidenced-based decisions about public health policies and programs.
The use of online learning, defined here as per Ally (2008) as the use of the Internet to acquire knowledge, grow, and construct personal meaning by accessing learning materials, interacting with content, instructors, and learners, and gain support while learning, is emerging as promising means of providing public health training (McKinney, 2017; Mincey, 2015). The use of online teaching platforms can connect learners with instructors and subsequently has the potential to increase the size of the public health workforce (Rosenstock et al., 2008). In the United States alone, online course enrolment increased from 5.9% in 2000 to 32.1% in 2012 (Ortagus, 2017), demonstrating a growing acceptance of this form of learning. Moreover, online courses can connect learners with one another, resulting in the creation of networks and communities that can enable action learning and problem solving around common areas of interest (Finch, Burrell, & McAfee, 2012). Those with similar goals who are living in geographically disparate areas and/or lacking opportunities for in-person training or education may benefit the most (Stamatikos & Ratnapradifa, 2011), including professionals who engage in public health work but are not public health professionals in title. A review of e-learning initiatives specifically for medical education in low- and middle-income countries (LMICs) concluded that e-learning can result in increased learning opportunities for students, but cautioned that quality of instruction and Internet connectivity, computer availability, Internet bandwidth, cost-effectiveness, and faculty and student ability to navigate the e-learning platforms can present challenges (Frehywot et al., 2013).
The aim of this article is to describe the development, facilitation, and lessons learned of an online course created to teach participants in teams from 14 LMIC countries how to design and conduct qualitative research to understand girls’ challenges managing menstruation at school. The goal of the course was to strengthen the ability of each country team to carry out research by building the capacity of the members. By the end of the course, we wanted all teams to have (a) a common base understanding of how menstruation poses challenges to adolescent girls in school and why it is important; (b) a foundational understanding of principles and tools of qualitative research methods, including ethics; (c) strengthened multidisciplinary connections within their own country teams, as well as with teams from other countries; and (d) locally generated evidence to inform policy and program decision making. Thus, completion of the course by all team members was a hope, but less of a focus than assuring that each team as a collective was gaining insights and working together to make informed decisions and progress on their collective research goals.
In this article, we provide a justification for developing the course, describe course participants, provide an overview of content and delivery, outline key achievements of country teams, and provide recommendations and lessons learned for future online learning initiatives aimed at strengthening public health capacity, particularly among nonpublic health professionals in LMICs who share common objectives.
Justification for Course Development
Menstrual hygiene management (MHM) has been recognized as a public health issue that is gaining attention in the global sphere (Sommer, Hirsch, Nathanson, & Parker, 2015). Qualitative research from Bolivia, Ghana, India, Kenya, Mali, the Philippines, Sierra Leone, Tanzania, and elsewhere have found that girls lack practical knowledge about menstruation, access to appropriate water and sanitation facilities and materials for managing their periods, and social support for understanding what is happening to their bodies, leading girls to report confusion, shame, fear, stress, teasing, distraction, reduced participation during class, and missing school (Alam et al., 2017; Caruso et al., 2013; Ellis et al., 2016; Girod, Ellis, Andes, Freeman, & Caruso, 2017; Haver et al., 2013; Long et al., 2013; Mason et al., 2013; Phillips-Howard et al., 2015; Sommer, 2009; Trinies, Caruso, Sogore, Toubkiss, & Freeman, 2015; van Eijk et al., 2016). Yet, despite growing research around this emerging topic, it remains so nascent, and taboo (Sommer & Sahin, 2013), that research has not been undertaken in many countries for policymakers and practitioners to understand girls’ experiences in their own local context. Furthermore, NGO practitioners, policymakers, donors, and other actors have limited guidance for how to address girls’ challenges.
There is consensus that action needs to be taken to ensure that girls can manage their menstruation while at school in a comfortable, dignified, safe, and equitable manner, and that local research is needed to inform enabling strategies. A recent call to action article outlined key priorities for addressing girls’ menstrual hygiene needs in schools, including building a strong cross-sectorial evidence base of local research to understand the contextually specific needs of girls to inform policy and practice (Sommer et al., 2016). A subsequent article outlining research priorities highlighted the need for participatory qualitative methods to ensure girls’ voices are integrated into policy decisions that impact their lives (Phillips-Howard et al., 2016).
In 2012, Emory University and UNICEF collaborated to research girls’ menstrual experiences at school in Bolivia, the Philippines, Rwanda, and Sierra Leone to provide local actors with evidence to inform policy and programs, resulting in the development of an overarching research methodology, various reports and manuscripts, an open-source booklet of tools for adaptation to other contexts, and increased interest from other UNICEF offices to conduct similar research (Caruso, 2014; Caruso et al., 2013; Haver et al., 2013; Long et al., 2013). To address this interest, UNICEF led the “WASH [water, sanitation and hygiene] in Schools for Girls: Advocacy and Capacity Building for Menstrual Hygiene Management through WASH in Schools Programmes” (WinS for Girls) project with funding from the Government of Canada (Sinden, Sahin, & Francois, 2015). UNICEF approached Emory University to develop and facilitate the e-course described here to build in-country qualitative research capacity, strengthen local ownership and investment in the issue, and connect teams with various stakeholders from across the globe carrying out similar work. Both UNICEF and Emory University agreed that the e-course approach would have a more lasting impact in terms of capacity, agency, and collaboration, than if Emory University lead the research itself, as had been done previously.
Course Participants
Twenty-six UNICEF country offices applied to headquarters to participate in the WinS for Girls program. Based on demand and geographic representation, the UNICEF headquarters selected 10 country teams from Afghanistan, Bolivia, Burkina Faso, Eritrea, Ghana, Kyrgyzstan, Mongolia, Niger, Nigeria, and Zambia. Four additional country teams received partial funding to participate given they had ongoing funded MHM research activities: India, Indonesia, Nepal, and Pakistan.
All selected country offices were advised to establish working groups composed of UNICEF staff, local government officials, local university and practitioner partners, and hired research consultants. All country team members were eligible and encouraged to enroll in the online course.
One hundred and twenty-seven participants enrolled in the course in November 2014, representing all 14 countries. At a midpoint check-in in March 2015, only 81 indicated they were able to continue participation. Of the 46 participants who discontinued participation, 28 (61%) were from the four countries that had ongoing research activities on MHM and did not receive full funding to participate in the program. As a result, two countries (India and Indonesia) no longer had any participants in the course. Research in both of these countries was well underway when the course started and later modules were not as relevant as a result. Of the 81 that remained in the course until the end, 32 (40%) were UNICEF staff, 22 (27%) were government staff, 8 (10%) were local research partners, 15 (19%) worked for local partner NGOs, and 4 (5%) were hired consultants (see Table 1).
Participants Enrolled in the Course and Receiving Certificates of Completion by Affiliation.
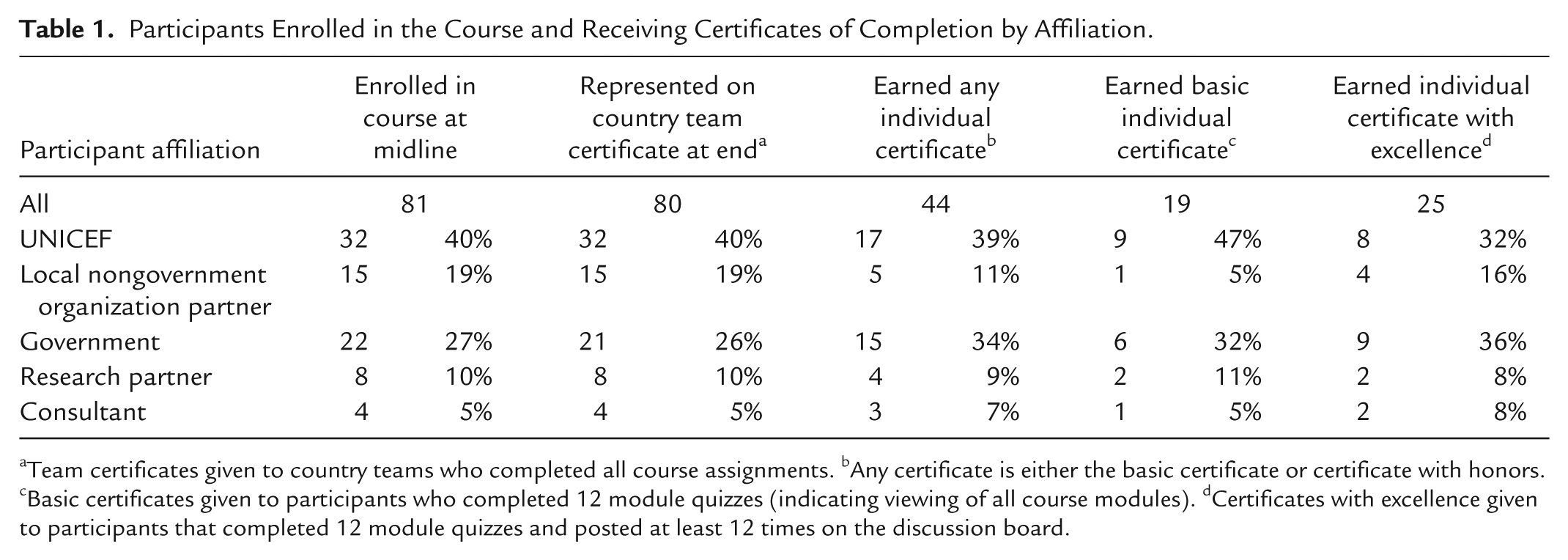
Team certificates given to country teams who completed all course assignments. bAny certificate is either the basic certificate or certificate with honors. cBasic certificates given to participants who completed 12 module quizzes (indicating viewing of all course modules). dCertificates with excellence given to participants that completed 12 module quizzes and posted at least 12 times on the discussion board.
Course Content and Delivery
Modules
The course included 13 modules taught live online at the same time for all participants approximately every 2 weeks from 20 November, 2014, to 28 May, 2015. It was intentionally spread over several months to provide sufficient time for participants to apply knowledge gained from class sessions between modules. Coauthors BAC, AE, and MS designed the outline of the course anticipating participants had little to no previous research experience or understanding of girls’ experiences of menstruation in school settings.
The course provided topical background and addressed three distinct research phases: preparation, execution, and application (see Table 2). Background modules (1-3) provided a broad overview of research on MHM in schools, water, sanitation, and hygiene (WASH) in schools, and key concepts in gender research. Research preparation modules (4-8) introduced participants to research ethics; described the fundamentals of research planning, with emphasis on working with multiple stakeholders; discussed the strengths and weaknesses of qualitative and quantitative research methods, particularly for taboo subjects like menstruation; and instructed participants on how to adapt and develop research tools. Research execution modules (9-11) covered data collection and management, research assistant training and piloting, and data analysis. Last, the research application modules (12 and 13) covered advocacy and application of findings for program planning. Modules and associated assignments covered several global health competencies expected of master’s-level students as recommended by the Association of Schools of Public Health at the time (see Table 2; Ablah et al., 2014). A syllabus with in-depth descriptions of each course module (Caruso, Ellis, & Sahin, 2015) and associated slides and materials (UNICEF, 2015) are available online for public use.
Course Modules and Associated Learning Objectives, Discussion Board Questions, Assignments, and Competency Domains.
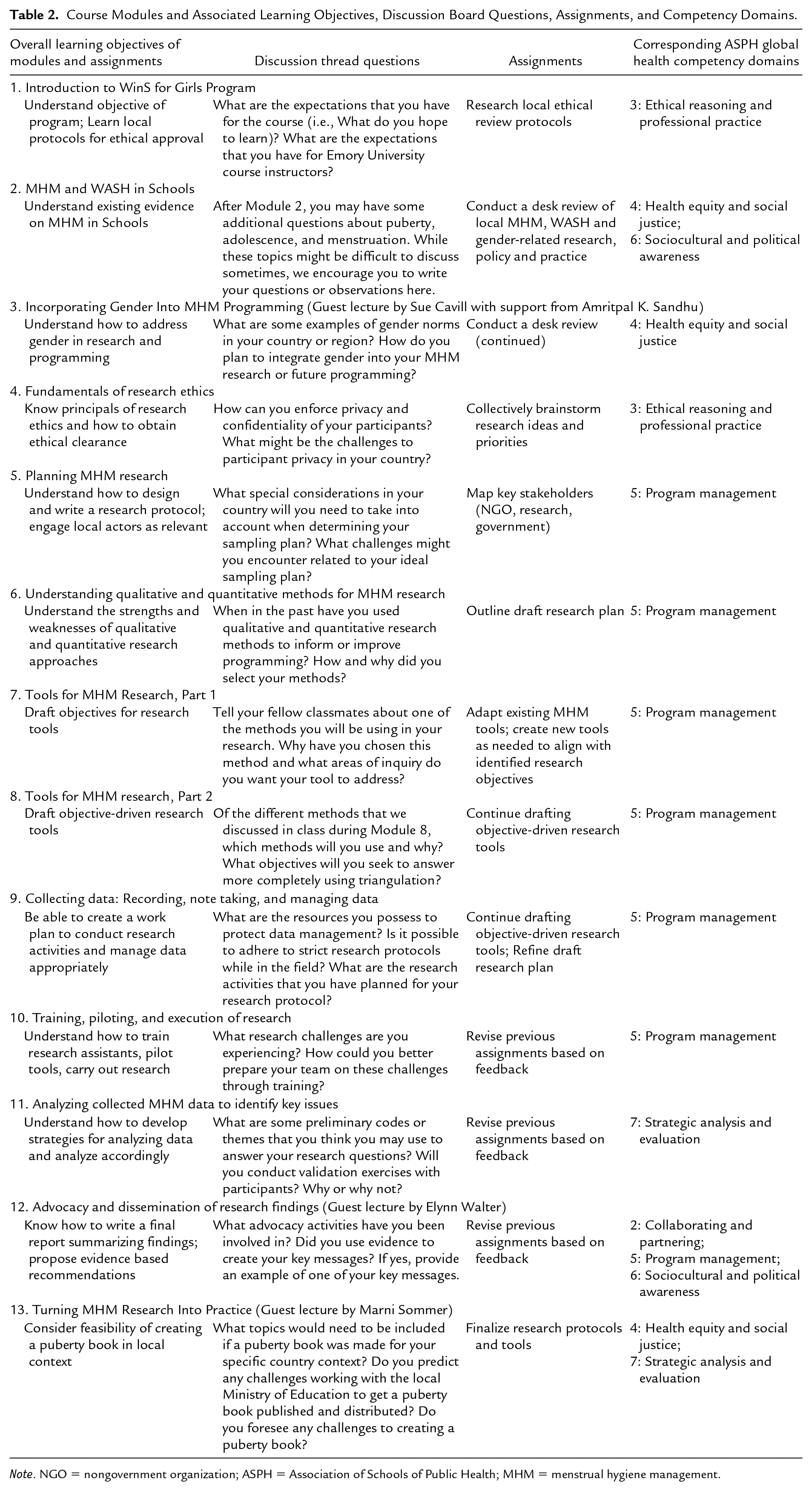
Note. NGO = nongovernment organization; ASPH = Association of Schools of Public Health; MHM = menstrual hygiene management.
Course Delivery
Coauthors BAC and AE served as the lead instructors and delivered most course modules. A noted benefit of online instruction, we easily and cost-efficiently recruited global experts to develop and deliver three sessions from afar (Finch et al., 2012): Sue Cavill with support from Amritpal K. Sandhu (Incorporating Gender Into MHM Programming), Marni Sommer (Turning MHM Research into Practice), and Elynn Walter (Advocacy and Dissemination of Research Findings).
The course was taught live via Adobe Connect in English from 7 a.m. to 8 a.m. EST in order to best accommodate participants across a range of time zones, though some sessions extended up to 30 minutes longer than the hour depending on the content needed to be covered or questions from participants. When signing into sessions, participants indicated the country from which they were participating and the number of people logging into the same computer as part of their username (i.e., Anna_USA_3). In many circumstances, computer and Internet access was limited and many participants gathered around a single computer to engage. This basic information in the username allowed participants to share about themselves and let instructors and others know the context from which comments were made.
Many participants from two countries, Niger and Burkina Faso, spoke French only or spoke limited English. To accommodate these participants, all slides were made available to participants several days to a week in advance to enabled teams to have the slides translated into French. This allowed participants to review the slides independently and follow-along with a translated deck during the live session. Team members who spoke English well were able to clarify questions for other team members. The Burkina Faso team had a translator available to translate all the sessions, either live or from the session recordings.
Questions were posed to participants several times throughout each module and the “chat” feature enabled active live participation during the modules. Instructors waited for and reacted to participant responses provided in the chat box, intentionally calling on contributors by name to recognize and encourage inputs. Emory University–based teaching assistants (coauthors GS and CG) and program leads from UNICEF headquarters (coauthors MS and SC) participated in all sessions, actively answering questions posed by participants and responding to or posting comments online via the chat window as the instructor delivered the course content. Their online activity motivated participants to be active and pose questions and responses to others. Most important, the chat feature allowed course participants to get to know one another; participants often directly posed questions to specific participants based on what they had come to learn about their context and experience.
Participants received e-mail reminders about the course the day before each scheduled module, with an embedded course link to the online platform. Due to work schedules, time differences, and unreliable Internet connections, it was not uncommon for participants to miss the live modules. All modules were recorded to enable later access as needed.
The course used Blackboard, a virtual learning and course management system, to manage the course schedule, readings, module PowerPoints and recordings, quizzes, a discussion board platform, and resources to reference and adapt (e.g., consent form templates, tools, and data entry forms used in other studies, etc.).
Assignments, Discussion Board, and Quizzes
After each module, participants received a group assignment and two individual tasks: a discussion board response and a “review and feedback” quiz.
All assignments aimed to sequentially guide country teams, step-by-step, through their own MHM research as part of the broader WinS for Girls Program. Example assignments included a literature review (which could later inform tool design or be incorporated into ethical review protocols and final reports), identification of research objectives, and drafting of research plans and tools (see Table 2 for all assignments). Though covered in depth later in the course, the first assignment required teams to investigate local research ethics review processes in their country given the lengthy amount of time typically needed for review and approval. Assignments were not graded. Rather, teams received feedback on all assignments from instructors and teaching assistants to strengthen their research. As each team worked in a different context, our comments focused largely on research methodology, though we also shared our knowledge of MHM-related issues in similar context to suggest readings, a line of inquiry, or probes that the team could consider if of interest. Teams were encouraged to submit revisions of research plans and tools for further feedback as often as they were motivated to do so. Each team had a “focal person” who was responsible for submission of all team assignments, facilitating communication.
Participants accessed a discussion board, where a new discussion thread was posted after each module session (see Table 2 for the discussion prompts), and the “review and feedback” quizzes via Blackboard. These individual assignments served to maintain participant engagement between module sessions and the discussion board facilitated sharing within and across country teams. Participants were encouraged to post on the discussion board after each module and could also initiate their own discussion threads, whether asking about a method, sharing an anecdote from their research, or asking other teams if participants in their study had reported similar experiences or beliefs. The quizzes reviewed key concepts from the modules using multiple choice, matching, and fill-in-the-blank questions, and elicited feedback from participants on the most useful thing they learned from the module session, concepts they were still uncertain about, and any suggestions or general feedback they had for the course. Course instructors and teaching assistants selected common questions or informative comments posted on the discussion board and from the quiz feedback questions to present at the beginning of the next course module, giving credit to contributors and addressing areas that needed greater explanation.
Office Hours
Office hours were held every other week (when course modules were not webcast). Office hours increased knowledge sharing between individuals and country teams and allowed course instructors additional opportunities to engage with participants. Initially, office hours were used to provide opportunities for participants to ask the instructors questions about the research that teams were initiating in their country. Participants could either e-mail questions in advance or ask them during the session. Later, office hours were led by country teams. They provided updates on their research progress. Teams signed up to provide brief 10- to 15-minute presentations describing their research challenges and achievements and their plans for next steps. Teams then received feedback and questions from instructors and other participants.
Individual and Country Team Achievements
At the end of the course, participants were eligible for certificates of participation. Basic individual course participation certificates were given to participants who completed 12 module quizzes (indicating viewing of all course modules); a participation with excellence certificate was given to participants who completed 12 module quizzes and posted at least 12 times on the discussion board. Team certificates were given to country teams who completed all course assignments. All twelve active country teams received team certificates and completed formative research and reports as hoped. Five of those country teams presented research findings at international conferences, and eight reported using formative research findings for advocacy purposes. Notably, both Mongolia and Zambia reported the integration of menstruation issues into national education policies. As the work of policymaking and program creation takes time, it is possible that teams will have achieved more by date of publication. Forty-four participants received individual certificates, including 25 who received certificates with excellence (see Table 1).
Reflections and Lessons Learned
Participant Reflections
Participants reported that the course not only aided with the overall research and provided them with new skill sets, but it also brought stakeholders from various sectors and cultures together, increased buy-in from government stakeholders on the topic, and engendered interest in additional learning opportunities. Still, unreliable Internet and managing the time for the course amid other work commitments remained a challenge (see Supplemental Table S1, available in the online version of this article, for participant reflections).
Instructor Reflections
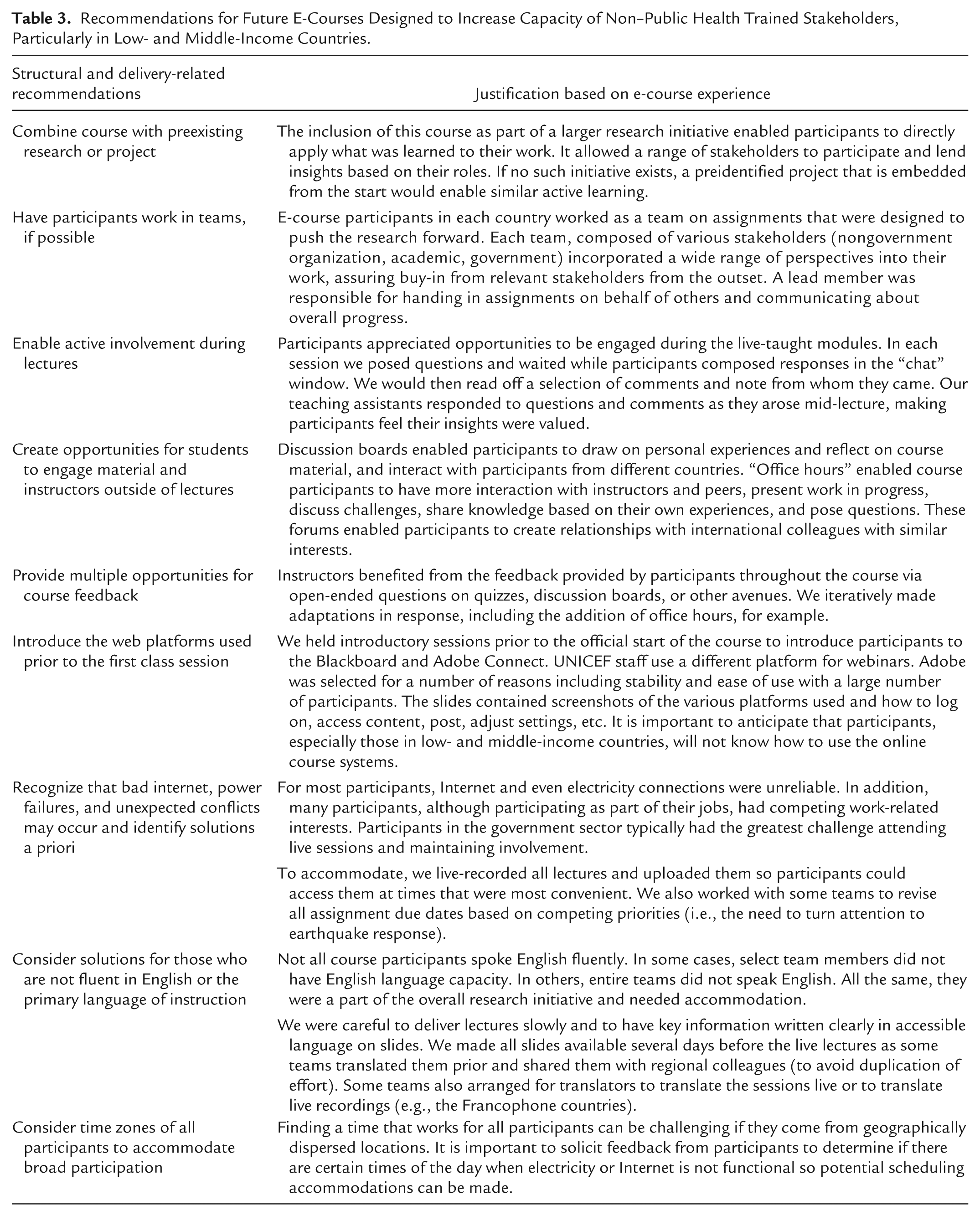
In Table 3, we present recommendations for others designing e-courses. We emphasize key lessons learned, particularly when working with a range of stakeholders in LMICs, though consider most recommendations to be applicable in non-LMIC contexts as well. Overall, active learning and opportunities for application, engagement, and teamwork are valuable tools for e-courses, just as they are in traditional classroom settings. Logistical issues are important to anticipate a priori, including consideration of time zones, language needs, and familiarity with technology.
Recommendations for Future E-Courses Designed to Increase Capacity of Non–Public Health Trained Stakeholders, Particularly in Low- and Middle-Income Countries.
Conclusion
Creating and embedding an e-course within a larger research initiative enabled all teams and participants to gain or improve research skills that benefited country-level research and that of the project as a whole. The course, however, had limitations. As reported by Frehywot et al. (2013), Internet connectivity was a challenge. Some participants could only access Internet from certain locations (i.e., not at home) influencing their availability to participate in real-time if they needed to go home or work in an alternate location, and in some places Internet was weaker at certain times of day affecting the quality of what participants received. Some participants did not have access to individual computers requiring them to tune-in as a group, limiting their ability to “chat” or engage in discussions. And, because the course was delivered to countries around the globe, the course could be early in the day, during the workday, or late in the evening, further influencing participation depending on personal schedules and ability to participate at those times. Despite challenges and limitations, however, the course also had several benefits, some also noted by others reporting on the design and delivery of e-courses: It enabled individuals to access information and learning opportunities that would be otherwise inaccessible (Stamatikos & Ratnapradifa, 2011); it provided a platform for participants from geographically disparate areas to share their perspectives and experiences on a common topic, engendering a community of practice and learning (Finch et al., 2012; Kanekar, 2017); it brought together diverse stakeholders in the same community working on the same problem who may not otherwise have had regular occasions to interact; and it created a support structure such that teams struggling with specific challenges could solicit feedback from both instructors and members of other global teams to determine a way forward or simply get assurance that their struggles were not uncommon.
E-courses have the potential to assist in tackling complex, public health issues that require engagement from a variety of stakeholders at local and global levels and their further development and deployment among public health and nonpublic health professionals should be explored further.
Supplemental Material
PHP811983_Supplemental_Material – Supplemental material for Building Qualitative Research Capacity Among Interdisciplinary Teams to Investigate Girls’ Challenges With Menstruation: Process and Lessons Learned From a 14-Country E-Course
Supplemental material, PHP811983_Supplemental_Material for Building Qualitative Research Capacity Among Interdisciplinary Teams to Investigate Girls’ Challenges With Menstruation: Process and Lessons Learned From a 14-Country E-Course by Bethany A. Caruso, Anna Ellis, Gloria Sclar, Candace Girod, Gauthami Penakalapati, Murat Sahin and Sue Cavill in Pedagogy in Health Promotion
Footnotes
Acknowledgements
The authors wish to acknowledge Gabrielle Berman, Lizette Burgers, Maria Carmelita Francois, Matthew Freeman, Nora Fyles, Molly Linabarger, Jeanne Long, Meera Mohan, Yodit Sheido, Marni Sommer, Elynn Walter, Brooke Yamakoshi, and all the participants for their contributions to this article or the course itself.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The e-course was part of the program “WASH [water, sanitation and hygiene] in Schools for Girls: Advocacy and Capacity Building for Menstrual Hygiene Management through WASH in Schools Programmes (WinS for Girls)” undertaken with the financial support of the Government of Canada provided through Global Affairs Canada. BAC was funded in part by the NIH/NIGMS Institutional Research and Academic Career Development Award (IRACDA), 5K12-GM000680-18.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.