
Abstract
Policy shapes the health of communities by enabling and limiting public health practice. Major organizations that focus on public health systems, education, and training stress the importance of policy to population health. They also recognize that practitioners should learn, practice, and be able to deploy policy skills. However, despite the recognized role of policy in public health, some public health practitioners remain uncomfortable with policy. And although teaching policy in public health programs appears on the rise, public health policy pedagogy literature is limited and tends to define policy narrowly. Service learning, which is used to teach other skills critical for public health, exhibits great promise as a tool to teach public health policy. This article describes an interdisciplinary, graduate-level public health policy course that relies on a service-learning approach. The course aims to teach public health policy principles, theories, and concepts and to make students more comfortable with public health policy through applied learning.
Few public health practitioners are comfortable with policy concepts, especially in the public sphere (Hernandez, Rosenstock, & Gebbie, 2003). They report limited engagement with (Kerr et al., 2017) and sometimes an aversion to public policy (McFarlane & Gordon, 1992). Perceived barriers to public health policy engagement include scarce resources and also a lack of familiarity with policy, limited confidence in advocacy skills, and frustration with policy processes (Mahas, Van Wasshenova, Everhart, Thompson, & Boardley, 2016; Moreland-Russell, Zwald, & Golden, 2016). Public health practitioners’ limited knowledge and comfort with policy may stem from ad hoc policy coverage in public health programs (Hearne, 2008), where public health policy courses tend to highlight the policy process, ethical and legal issues, and advocacy (Heiman, Smith, McKool, Mitchell, & Roth Bayer, 2016). It may also be aligned with national patterns of low levels of knowledge about political institutions and low levels of civic interest and participation, despite rising educational attainment (Checkoway, 2001; Galston, 2007).
Discomfort with policy is concerning because of policy’s critical role in public health. Policy can change population-level health determinants and improve health outcomes. For example, policy has helped protect air and water, reduce motor vehicle injuries and fatalities, prevent and contain infectious disease outbreaks, and combat chronic diseases primarily by focusing on tobacco, food, and physical activity (Moulton, Goodman, & Parmet, 2007).
Definitions of policy in public health policy vary but are usually expansive. Policy includes “laws, regulations, and judicial decrees as well as agency guidelines and budget priorities” (Brownson, Chriqui, & Stamatakis, 2009, p. 1576). Policy also includes “procedure, administrative action, incentive, and voluntary practice of governments and other institutions” (Centers for Disease Control and Prevention, Office of the Associate Director of Policy, n.d., p. 1). And, in today’s Health in All Policies era, public health policy extends beyond the traditional health sector to transportation, housing, education, agriculture, and other sectors because they all affect health at some level (Rudolph, Caplan, Ben-Moshe, & Dillon, 2013).
Guidelines for public health systems, professionals, and organizations acknowledge the significance of policy in public health practice. For example, in 1988, the U.S. Institute of Medicine deemed “policy development” one of three Core Public Health Functions (Institute of Medicine, Committee for the Study of the Future of Public Health, 1988, p. 44). Policy-related work also appears in each of the 10 Essential Public Health Services, perhaps most directly as developing policies, enforcing laws, evaluating interventions, and managing systems (Centers for Disease Control and Prevention, 2018). Health department accreditation standards also reinforce the significance of policy. Two of the 12 domains of the Public Health Accreditation Board (PHAB; 2013) focus on policy directly: “Domain 5: Develop public health policies and plans” (p. 124) and “Domain 6: Enforce public health laws” (p. 167). Additional policy elements are incorporated into other PHAB domains and standards, including Standards 1.4 (integrating data analysis and policy recommendations) and 3.1 (health promotion policies around prevention; PHAB, 2013).
Education and Training in Public Health Policy
Contemporary standards for educating public health and health education practitioners in the United States emphasize learning and applying policy principles. For example, four of the Master of Public Health (MPH) Foundational Competencies espoused by the Council on Education for Public Health (2016) directly reference public health policy; they call for MPH graduates to be able to discuss the policy-making process, identify stakeholders and build coalitions, advocate for health-promoting policies and programs, and evaluate impacts of policies. Similarly, the National Commission for Health Education Credentialing, Inc. (2015) established a competency to ensure credentialed health education specialists (i.e., Certified Health Education Specialist and Master Certified Health Education Specialist) can “[i]nfluence policy and/or systems change to promote health and health education” (p. 11). This competency involves assessing the effects of policies and systems on health, projecting impacts of policy changes, using evidence-based policy analysis, and advocating for health-promoting policies (National Commission for Health Education Credentialing, Inc., 2015).
Teaching policy in public health programs is on the rise (Hearne, 2008), perhaps in response to these standards. However, literature examining the current state of teaching and training of health policy across health-related disciplines (including public health, medicine, nursing, and health care administration) reveals notable patterns. First, as Heiman et al. (2016) state in their systematic review, “Literature published in the past 30 years on health policy training remains limited” across health-related disciplines but especially in public health (p. 7). Second, in the context of teaching and training, educators and professionals in health-related disciplines tend to define health policy narrowly, focusing primarily on health care delivery systems rather the more expansive policy definitions embraced by public health (Heiman et al., 2016). Third, teaching and training in health policy faces several barriers, including inadequate resources, perceptions that it is of limited relevance, incongruity with faculty interests and expertise, time constraints, and insufficient research on best practices (Heiman et al., 2016).
Many public health practitioners, educators, and trainers indicate that learning health policy requires fusing classroom learning and practical application. Public health practitioners report the value of stand-alone public health policy courses, efforts to integrate policy concepts across the public health curriculum, and “practical policy experiences that involve students directly in the policy process” (Moreland-Russell et al., 2016, p. 653). Meanwhile, health policy educators and trainers recognize the importance of combining lecture-based learning with case studies, group projects, and discussions and emphasize skill-building and application, interactions with policy participants, real-world practice, and experiential and service learning (Hearne, 2008; Heiman et al., 2016).
Public Health Policy Through Experiential and Service Learning
Public health programs rely on learning by doing to teach various topics and skills (Gregorio, DeChello, & Segal, 2008). Experiential learning involves gaining classroom knowledge and skills and applying what is learned inside the classroom in a real-world setting with immediate consequences outside the classroom (Bentley & Swan, 2018; Cashman & Seifer, 2008). It connects theoretical information and practical skills to encourage discovery of knowledge through application, new ways of thinking, self-reflection, and civic engagement (Bentley & Swan, 2018; Cashman & Seifer, 2008). Service learning, a type of experiential learning (Bentley & Swan, 2018; Cashman & Seifer, 2008), is also frequently used in public health education. Service learning integrates community service with academic course-work “through a cycle of action and reflection” in which “the service enhances the learning and the learning enhances the service” as students, faculty, and community partners respond to community-identified needs (Cashman & Seifer, 2008, p. 274). Public health service learning emphasizes “learning how to intervene on the multiple factors that affect health and quality of life” (Cashman & Seifer, 2008, p. 274) and aligns with social justice values (Sabo et al., 2015). Public health service learning is also a useful teaching mechanism. Sabo et al. (2015) found that after a weeklong service-learning course focused on specific populations, graduate public health students in several U.S.-based programs reported enhanced communication skills, abilities to identify personal strengths, awareness of the health professionals’ roles, responsibility for their own learning, and leadership.
Service learning can help teach health policy (Heiman et al., 2016; O’Brien-Larivée, 2011). However, the literature contains few discussions of service learning in health policy courses, particularly in public health (Heiman et al., 2016). Examples of how to teach public health policy through service learning are needed because (1) policy plays a major role in public health practice, (2) public health practitioners report limited comfort with policy, (3) the literature contains limited information on teaching and training in public health policy, and (4) service learning shows promise to reinforce health policy concepts and develop professional identities. This article offers a way to structure a graduate-level, service-learning public health policy course.
The Course—Public Health Policy: Integrating Theory and Practice
This course is designed to introduce students to disciplines and theories pertinent to the policy-making process and tools relevant to understanding, making, and advocating for health-promoting policies. It is structured as an interdisciplinary, service-learning course available to graduate-level students of public health (i.e., MPH and PhD level), law (i.e., second and third years), and other health-related disciplines. The goal of the course is to enable students to engage directly with the public health policy process. It aims to achieve this goal by simultaneously examining public health policy from a theoretical vantage and applying policy concepts and skills through a community-oriented, semester-long project. By the end of the semester, students should be able to do the following:
Describe the policy process
Discuss how policy decisions shape health determinants and outcomes
Explain and analyze theories underlying policy processes and outcomes
Identify examples of how scientific, legal, political, ethical, and economic factors influence public health policy decisions
Develop a real-world policy analysis of a public health issue important to the community.
This course is offered at a large, public, research university. Student enrollment is capped at eight students to facilitate collaborative service learning. The class meets weekly during the semester for 2 hours and 45 minutes. Meetings are divided into two complementary segments: (1) examining public health policy theory through readings and facilitated class discussions and (2) applying public health policy knowledge through a service-learning project.
Conceptual and Theoretical Content
To understand how policy shapes public health, students explore a series of topics, theories, and disciplines during the first segment of most class meetings. The course defines “policy” as decisions of governmental and private organizations regarding rules, practices, and processes as well as their implementation (Golden & Moreland-Russell, 2016). Topics and related learning objectives are summarized in Table 1. Assigned readings include segments from two books (Bhattacharya, 2013; Eyler, Chriqui, Moreland-Russell, & Brownson, 2016) as well as peer-reviewed journal articles and policy reports. They serve as the basis for class discussions.
The Theoretical Component: Course Topics and Corresponding Learning Objectives.
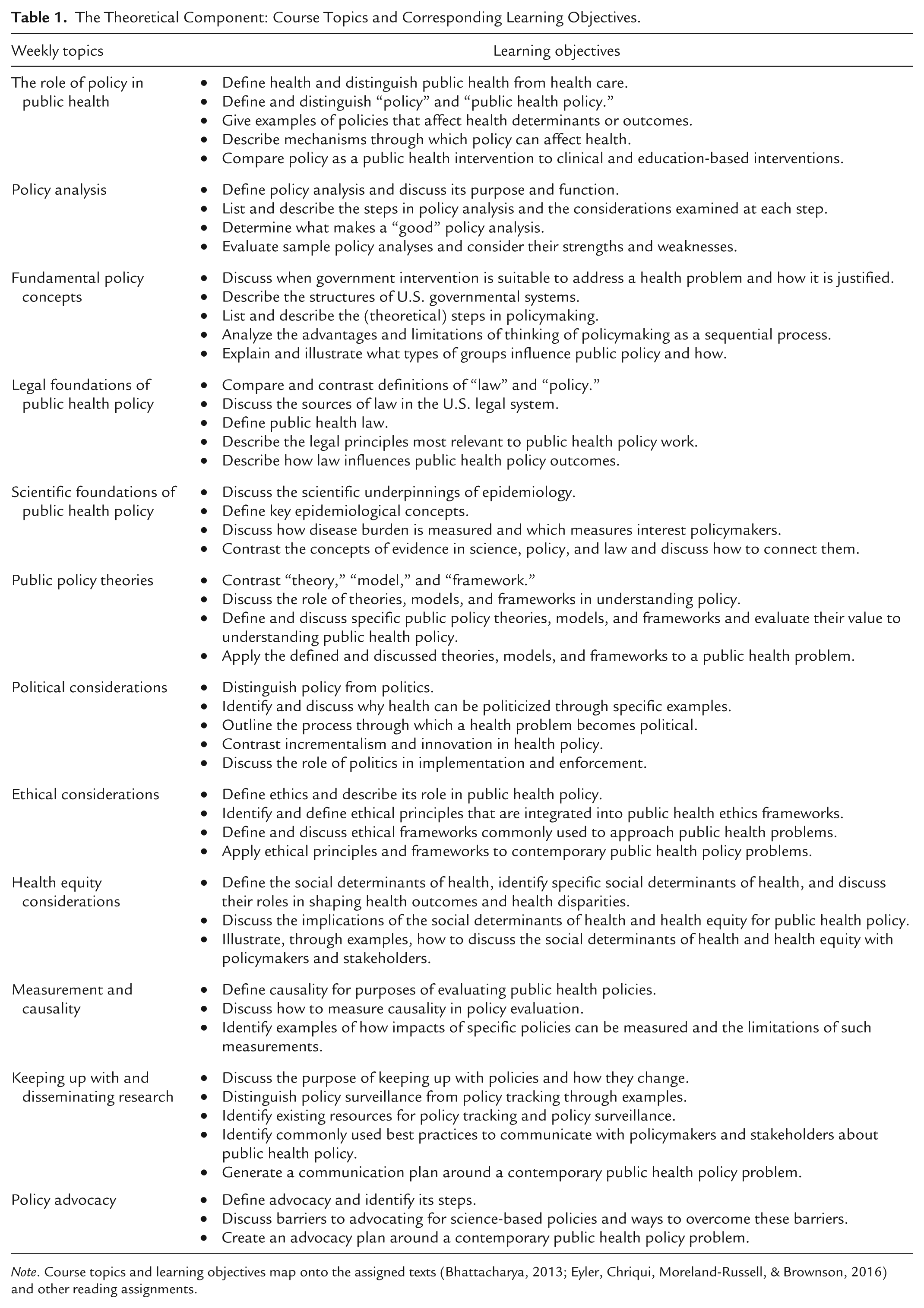
Note. Course topics and learning objectives map onto the assigned texts (Bhattacharya, 2013; Eyler, Chriqui, Moreland-Russell, & Brownson, 2016) and other reading assignments.
Students and the instructor define concepts, examine their contribution to understanding public health policy, and apply them to contemporary public health problems through discussions and exercises. Service-learning projects illustrate how theories and concepts apply. For instance, after students read about various public policy theories, the instructor facilitates a discussion to define each theory, analyze how it informs public health policy, and apply it to the service-learning project topic (e.g., youth obesity or levels of public health funding). Similarly, after students read about ethical frameworks, the instructor facilitates discussion to outline each and to apply it to the policy alternatives examined in the project.
Diverse academic and professional backgrounds enable students to alternate as “experts” and “novices.” For example, public health students take the lead to describe concepts of morbidity and mortality while law students lead analysis of legal constraints on governmental authority. Diverse student perspectives simultaneously ensure students are exposed to new concepts and are also challenged to explain, apply, and teach familiar ones.
Application Through Service Learning
Students simultaneously apply public health policy concepts through a semester-long, service-learning group project that concerns a public health problem with policy components. This project involves a thorough policy analysis modeled on an established process described by Chriqui and Young (2016). The project is completed in conjunction with a community partner organization.
Selecting a Community Partner Organization and a Policy Problem
The instructor selects a potential community partner to work with students before the start of the semester. The partner is identified after considering: preexisting relationships between the instructor and the partner, the partner’s active participation in the public health system, and the partner’s knowledge about public health issues affecting the community. The instructor approaches the potential partner to assess levels of interest, reciprocal value of collaboration, and commitment to working with students all semester.
If the instructor and partner decide to collaborate, they generate a list of possible project topics. The needs of the community partner drive topic selection. However, the instructor also considers the availability of research, how other communities use policy to handle this problem, governmental authority, policy history, and feasibility of completing the policy analysis in a semester. The topic is selected both to generate useful deliverables for the partner or community and to provide a valuable pedagogical opportunity. The community partner appoints a staff member as the primary point of contact for the class.
Conducting the Policy Analysis
Students first read about and discuss the policy analysis process, as outlined in Chriqui and Young (2016), and sample policy analyses. Then, they complete a series of assignments designed to research, analyze, and produce the components of an objective policy analysis. Students (1) craft a problem statement, (2) conduct background research and analysis regarding the problem, (3) analyze the policy landscape and stakeholder perspectives, (4) generate policy alternatives to address the problem, (5) establish and define evaluation criteria, (6) analyze the policy alternatives based on the selected criteria, and (7) ultimately generate policy recommendations (Chriqui & Young, 2016). Students apply public health policy knowledge and skills to the real-world community problem in each exercise. All assignments must be informed by outside research, including scientific peer-reviewed literature, gray literature, public health data, legal documents (e.g., relevant statutes, regulations, cases), and publicly available information.
Table 2 outlines the policy analysis assignments and activities. Assignments, as well as pre- and postassignment activities and feedback, occur in a week-by-week pattern of (1) preparation; (2) completion; (3) discussion, reflection, and feedback; and (4) revision. The problem statement assignment illustrates this pattern. First, students encounter the project problem by reading community partner documents and interacting with a partner representative. Then, they draft and turn in a problem statement. Students receive written feedback from the instructor on how to improve the draft. They also critique each other’s problem statements as the instructor circulates in the classroom to provide additional feedback and to answer questions. Finally, the instructor facilitates a group exercise to integrate draft problem statements into a working problem statement that the group uses and revises for the remainder of the project. The purpose of feedback is to improve assignment quality and to encourage critical thinking and reflection about what makes a “good” policy analysis.
The Policy Practice and Service-Learning Component: Policy Analysis Assignments.
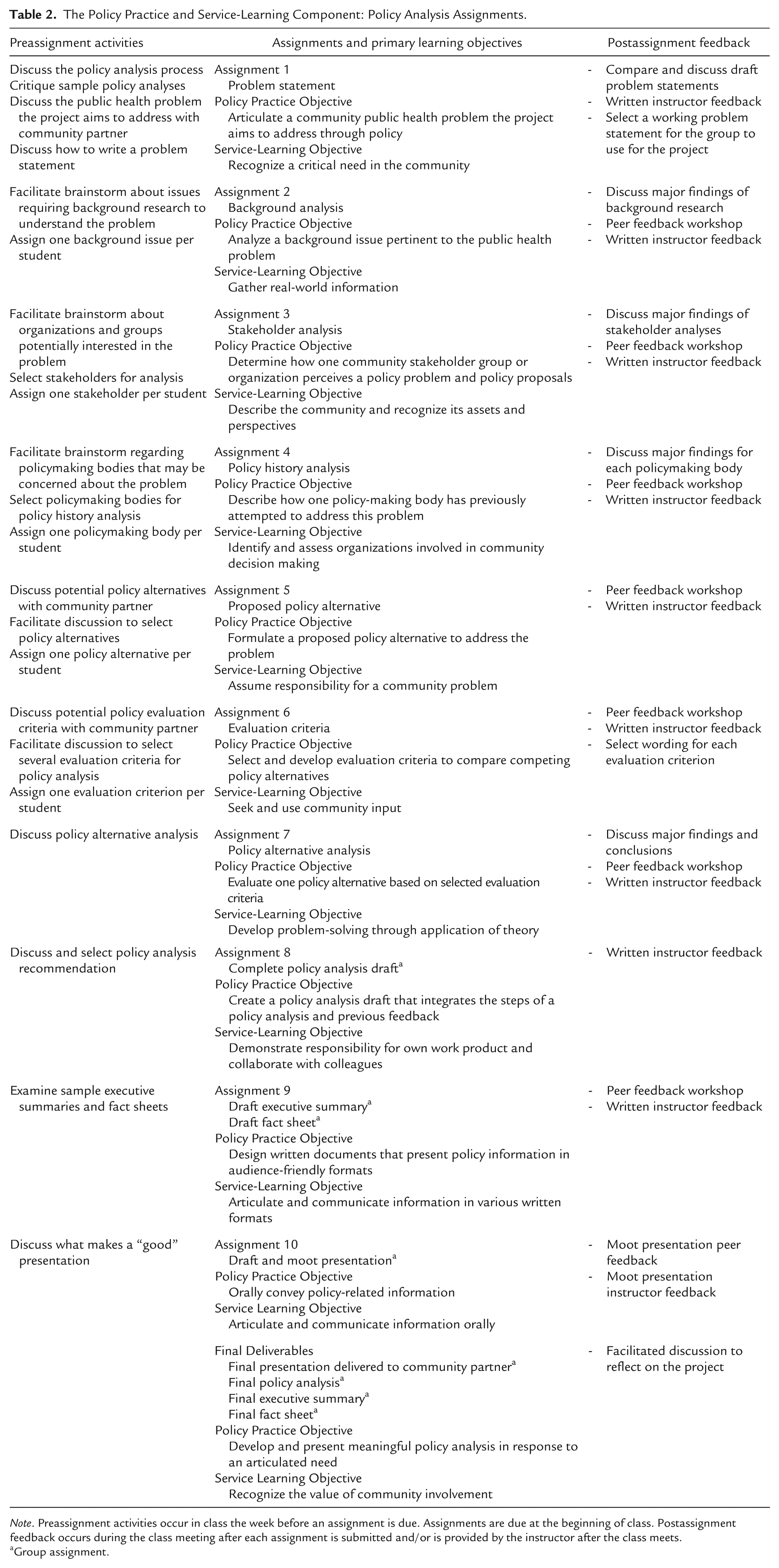
Note. Preassignment activities occur in class the week before an assignment is due. Assignments are due at the beginning of class. Postassignment feedback occurs during the class meeting after each assignment is submitted and/or is provided by the instructor after the class meets.
Group assignment.
The project culminates in group deliverables: a final policy analysis, an executive summary, a fact sheet, and an oral presentation to the partner organization. Importantly, the final policy analysis contains policy recommendations to address the identified problem that are generated by analyzing policy alternatives along evaluation criteria selected through brainstorming, research, and discussion with the community partner. For example, for a project focused on obesity rates among minority youth, students generated and examined policy alternatives: maintaining the status quo, enacting a sugar-sweetened beverage tax, amending physical education requirements, enhancing implementation of an existing school wellness policy, incentivizing healthy weight through college savings accounts, expanding vending machine labeling requirements, and increasing funding for a child nutrition and food security program. Students analyzed the legal authority, scientific evidence base, equity implications, administrative feasibility, and political feasibility of each alternative. They ultimately recommended enhancing implementation of a school wellness policy because this policy alternative received the highest marks across the five evaluation criteria.
Student–Community Partner Interactions
Students interact with community partner representatives at multiple stages in the policy analysis process. A partner representative attends class to discuss the public health problem and its salience to the community. A representative also attends class to participate in the discussion that generates and selects policy alternatives and evaluation criteria. In these classes, students drive the dialogue and the representatives provide real-world input to guide how students approach the problem and potential solutions. Such discussions allow students to practice formulating questions, gathering information, interviewing, and synthesizing and integrating feedback.
The end-of-semester presentation to the partner organization’s staff serves as the final interaction. The point of contact assists with coordinating this event. During the presentation, students spend 35 minutes presenting their policy analysis and their ultimate recommendations. The remaining 25 minutes consist of exchanges between students and partner organization staff in which students answer staff questions and receive feedback on their analysis. The partner organization posts project deliverables on its community resources website, and the presentation informs community partner discussions.
Assessment of Student Work and Student Reactions
The instructor evaluates all assignments. Individual assignments cumulatively comprise 30% of a student’s course grade. The instructor considers timeliness, the extent of research, the depth of analysis, the quality of writing (e.g., grammar, syntax, cohesiveness, readability, and citations), and the students’ ability to demonstrate how the assignment fits into the larger policy analysis process when evaluating assignments. Another 40% of the grade, which is assigned to the group, is based on the final project deliverables: the policy analysis, presentation, executive summary, and fact sheet. The instructor considers the same criteria used in evaluating individual assignments as well as fidelity to the policy analysis process, organization, integration of feedback received over the semester, and cohesiveness and polish of deliverables. Class attendance and the quantity and quality of in-class participation comprise the remainder of the grade.
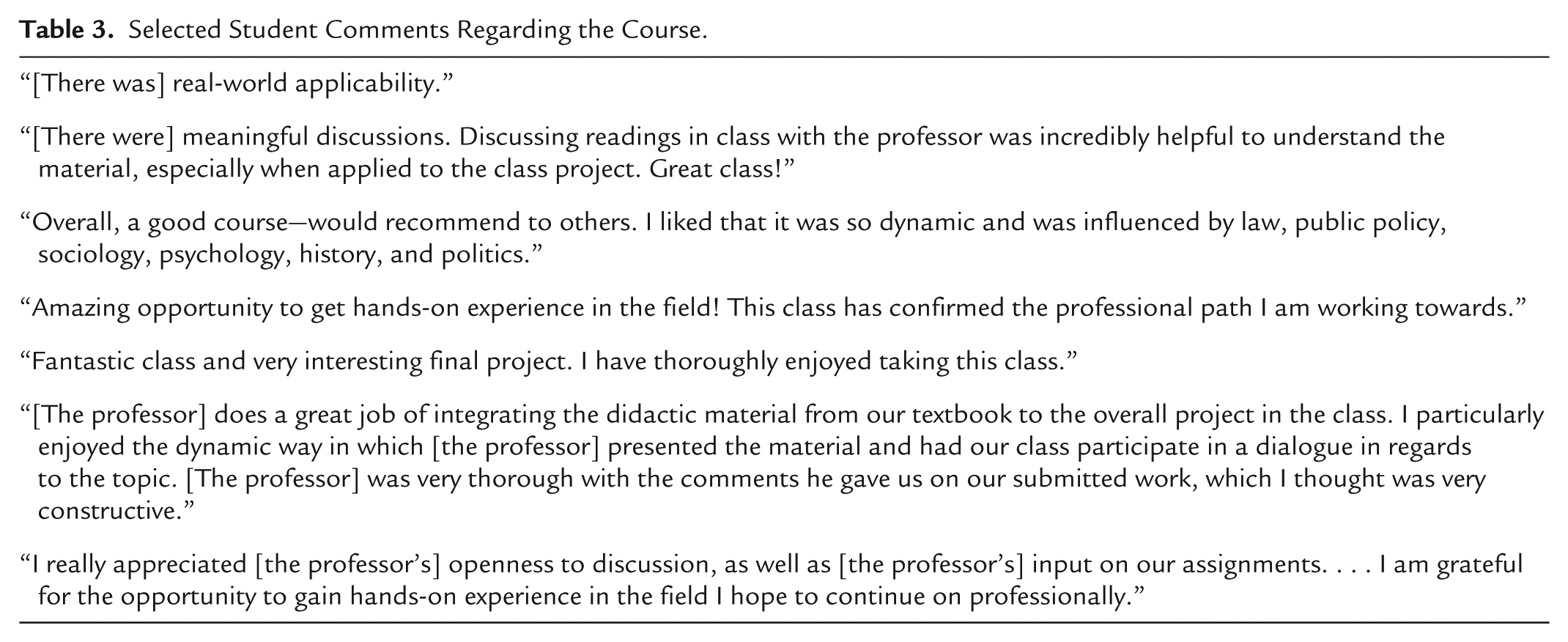
Students have articulated overall positive reactions to the course. Table 3 contains selected excerpts from anonymous, end-of-semester course evaluations. These comments indicate that students appreciated applying public health policy concepts in a real-world setting and in an interdisciplinary manner. Some students emphasized the influence of the course in shaping their professional goals and identities.
Selected Student Comments Regarding the Course.
Conclusion
The power of policy is central to public health. However, many public health practitioners and students appear uncomfortable with policy concepts and the policy process. Research, theory, and case studies help illuminate policy. Alone they cannot prepare students for public health policy work. Hands-on learning is essential. A service-learning course that uses a real-world project creates an opportunity to apply policy principles through engagement with a community partner. Such a course requires preplanning and flexibility. The instructor must foster a relationship with a community partner, select a project that is useful to the partner and optimal for learning, and join students in a world of uncertainty where “right answers” may be difficult to discover.
However, a service-learning course with a real-world project helps demystify public health policy for students. It allows them to tackle the challenges of how to frame problems, grapple with scientific research, and formulate and analyze solutions in a complex and dynamic world. It enables learning through experience and service, demonstrates that data are not always accessible, and necessitates difficult choices. A public health policy course with a real-world project illustrates how and when to apply policy theories and also how and when they break down, how competing considerations fit together, and how to communicate with users in mind. Finally, it fosters connections among students, faculty, universities, and community partners while enhancing the capacity of the public health system.
Footnotes
Acknowledgements
The author thanks the University of Nevada, Las Vegas, for supporting this course; the students for their interest in public health policy and dedication to their service-learning projects; and the community partner for enabling this method of teaching.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.