
Abstract
Documented health disparities among racial and ethnic minorities exist in the United States, and health injustices frequently have deep historical ties, especially in the South. Therefore, it is critically important for students to understand root causes of both historical and contemporary public health issues and their effects on population health. In spring 2018, 15 undergraduate and graduate students from the University of Alabama at Birmingham participated in a six-credit-hour travel course by touring throughout the Deep South to learn more about the ways in which history and place interact with programs, policies, and practices to influence population health. Students saw firsthand how the social determinants of health frequently affected access to health care and discovered the value of a multidisciplinary approach to public health and health programs in addressing health equity. The purpose of this article is to describe student experiences with the travel course through an exploration of students’ reflective journal entries, blog posts, and student presentations. Additionally, the authors report results of a self-assessment designed to measure student interest and level of comfort in working with, or on behalf of, medically underserved populations. The article concludes with implications for public health and best practices for offering place-based courses across academic majors.
Those who cannot remember the past are condemned to repeat it.
Documented health disparities among racial and ethnic minorities exist in the United States (Bouye, McCleary, & Williams, 2016; Braveman et al., 2011). Despite tremendous strides over the past several decades in providing preventive services and high-quality clinical care as well as significant investments in U.S. health care spending, “race/ethnicity disparities persist in life expectancy, vaccination rates, infant mortality, and exposure to pollutants” (U.S. Department of Health and Human Services, 2016, pp. 6-7). Health injustices frequently have deep historical ties, especially in the South (Levy & Sidel, 2013); therefore, it is critically important for students to understand root causes of both historical and contemporary public health issues and their effects on population health.
In spring 2018, the University of Alabama at Birmingham (UAB) piloted a 2-week, six-credit-hour travel course for undergraduate and graduate students to explore population health in the Deep South, an area we defined by the following four states in the southeast region: Alabama, Mississippi, Louisiana, and Georgia. The overarching goals of the course were to illustrate the interdisciplinary nature of public health practice and demonstrate the ways in which the social determinants of health must be addressed to achieve health equity among the poor and underserved.
The purpose of this article is to describe student experiences with the travel course through an exploration of their reflective journal entries, blog posts, and student presentations. In addition to providing qualitatively rich data through student work, the authors report results of a self-assessment designed to measure student interest and level of comfort in working with, or on behalf of, medically underserved populations (MUPs): populations with a lack of access to primary care services (Health Resources and Services Administration, 2016). The article concludes with implications for public health and best practices for offering place-based courses across academic majors. As a strategy for reflective practice, this project was conducted, in part, to guide course improvement. The question that guided this study was the following: What are student experiences in a travel course in the Deep South in relation to population health, health equity, and the social determinants of health? Subquestions gauged student interest and level of comfort in working with, or on behalf of, medically underserved populations.
Background
This cross-listed undergraduate and graduate travel course, titled “Exploring Population Health: On the Road in the Deep South,” was designed to include a 2-week, out-of-classroom experience conducted during the May mini-term. Seed money for the course was provided by the UAB Quality Enhancement Plan Teaching and Learning Award and coordinated through the UAB Office of Education Abroad. The course was led by one public health faculty member and one teaching assistant with additional support (e.g., logistics) provided by the Office of Public Health Practice in the UAB School of Public Health. Through this course, students representing multiple public health majors and varying degree levels (i.e., bachelor’s, master’s, doctoral), toured historically significant sites; visited communities and community-based organizations; attended presentations about contemporary and historical public health issues; and visited local, state, tribal, and federal public health agencies to learn about organizational structures, programs, service delivery models, and approaches to addressing issues of public health. In 12 days, one faculty member, one teaching assistant, and 15 students traveled more than 1,200 miles, visiting four states, nine cities, and 20 sites significant to public health.
Predeparture
The week prior to departure, students met with faculty and staff to review course expectations and student responsibilities and discuss relevant public health topics through journal articles, assigned readings, and presentations on the following:
Human immunodeficiency virus (HIV) and sexually transmitted infections (STIs)
Tuberculosis (TB) and the history of the Mississippi TB Sanatorium
Radiological exposures and the history of the Salmon Test Site
Social determinants of health, poverty, and exacerbated disaster outcomes due to Hurricane Katrina
Culture and healthy eating
Infectious disease outbreaks and the history of quarantine in the United States
BP Deepwater Horizon oil spill effects
Marine litter and microplastics
Tuskegee syphilis experiment and bioethics
Zoonotic diseases and “One Health” concept
Green space and redevelopment
The Carter Center’s Guinea worm eradication project
Homelessness and access to health care
In addition to facilitating class discussions, students worked in teams to develop definitions for the following terms: population health, health equity, and social determinants of health. After all teams presented their term definitions, the entire class worked as a group to reach consensus on final definitions that students used throughout the travel course to inform their observations, journal reflections, and blog post assignments as well as to guide their posttrip presentations (see Table 1). Topics and definitions were heavily influenced by student readings from the book Healthier: Fifty Thoughts on the Foundations of Population Health, a text that describes strategies for approaching population health from a social justice perspective (Galea, 2018).
Terms and Definitions. a

Definitions were based on student consensus of terms.
The Experience
In this travel course, students visited historically significant sites throughout the Southeast with stops in Alabama, Mississippi, Louisiana, and Georgia. On a typical day, participants boarded a chartered bus at 8:00 a.m. and travelled to two locations per day. At each site, students met with officials from local, state, tribal, and federal public health agencies or subject matter experts to discuss past and present public health issues and frequently toured facilities and/or areas negatively affected by natural or man-made disasters. Students were encouraged to take pictures at each site to be included in final student presentations and a project vision board. While traveling on the bus between sites, students were led through guided discussions/debriefing sessions of what they saw and heard at each site, frequently using reflection questions and definitions of population health, health equity, and social determinants of health to prompt discussion. In the evenings, students completed daily student reflection journal entries or worked in small groups to construct content for daily blog posts. Journal submissions and blog posts were based on structured questions and frequently focused on the public health and/or historical significance of the site visit as well as student learning, observations, and experiences of each community.
Literature Review and Conceptual Framework
To frame this article, our team adopted a general, conceptual perspective of experiential education guided by adult learning theory and informed by both Public Health 3.0 and Council on Education for Public Health accreditation standards for public health. The team also drew from Pipitone’s (2018) conceptualization of place-based learning to inform our understanding of learning spaces that both shape and are shaped by sociocultural, sociospatial, and historical perspectives.
Adult Learning Theory
The research literature shows that adult learning occurs best through experiential approaches; however, most graduate-level courses in the United States still rely on a traditional lecture style format with limited hands-on activities (Fink, 2003; Merriam, Caffarella, & Baumgartner, 2007). Moreover, researchers have demonstrated the limitations of the teaching-as-telling (lecture) style of instruction (Prosser & Trigwell, 1999; Ramsden, 1992), yet it continues to be the predominant method in which instruction occurs at the postsecondary level in the United States.
Unlike child-centered learning (pedagogy), adult-centered learning (andragogy) recognizes that adult learners have different developmental needs and life experiences (Knowles, 1968; Merriam et al., 2007). Knowles (1980) described the following characteristics of adult learners: they (a) are independent and self-directed learners, (b) use life experiences as a resource for learning, (c) demonstrate readiness for learning based on needs that reflect social roles, (d) are problem solvers who want to apply what they have learned to their personal and professional lives, and (e) are intrinsically motivated to learn. Therefore, courses designed for adult learners must focus on student-centered approaches to learning that are both relevant and meaningful for the student (Wlodkowski, 2008).
Experiential Education
The principles of adult learning theory lay an appropriate foundation for experiential education to occur (Moon, 2004). Experiential education is an educational philosophy that describes out-of-classroom learning opportunities that many colleges and universities in the United States offer to enhance students’ classroom curriculum (Gardner & Bartkus, 2014). Kolb (1984) defined experience-based learning as a process whereby knowledge is created through the transformation of experience (Higgins, 2009; Yardley, Teunissen, & Dornan, 2012).
Experiential learning activities are broadly used across academic disciplines (de Oliveira et al., 2015; Warkentin, 2017), and include a wide range of options, including clinical internships, service learning, cooperative education, and place-based education (e.g., study abroad, study away; Austin & Rust, 2015). Irrespective of format, experiential education programs share a common set of principles and characteristics: (a) reflection, critical analysis, and synthesis of the learning experience; (b) student accountability for learning; (c) active engagement; (d) deeper understanding of self and self in relationship to others; and (e) opportunities for growth through natural consequences, mistakes, and successes.
As a place-based form of experiential education, this travel course most closely resembled study away, an educational strategy that integrates study abroad programs with domestic programs. Sobania and Braskamp (2009) persuasively argued that the benefits of study abroad programs, such as self-identity formation, cultural sensitivity, cross-cultural communication, and the ability to adapt to changing circumstances, are not limited to international settings: Today, even in many rural locations, the United States has become so richly diverse that one does not need to travel more than a few blocks from campus to have a cross-cultural experience, to hear other languages spoken, meet people from different cultural traditions, and discover religious practices from one’s own. (p. 23)
Tracing the history of public health in the United States through significant events and locations in the Deep South provided further support for offering a travel course in a specific geographic region of the country.
Importance of Place
McClellan and Hyle (2012) suggested that the goal of higher education should be to facilitate learning experiences. Citing Fink (2003), the authors stated, “If we can find ways to identify and create learning experiences that students and others can agree are truly significant, we will have made important progress in our effort to improve the quality of higher education” (Fink, as cited in McClellan & Hyle, 2012, p. 240). The concept of place, however, plays a vital role in determining the significance of the learning experience. Informed by the work of Pipitone (2018), our team envisioned this travel course as encounters with learning spaces that are situated within sociocultural and sociospatial contexts and reflect historical perspectives that are frequently complex and controversial. Pipitone (2018) noted that these composite viewpoints allow for “exploration of the ways in which experiences in/of place are both socially produced and socially producing through engagement with surrounding environments” (p. 59).
Public Health 3.0
Public Health 3.0, a call to action issued in 2016 by the U.S. Department of Health and Human Services, describes a set of practices that modernizes public health goals and missions for the 21st century to address social determinants of health and promote health equity in the United States. Public Health 3.0 identifies key steps that must be taken to ensure the health and well-being of all U.S. citizens. Of salience to the current discussion, Public Health 3.0 advances the need to build a strong public health workforce and establish cross-sector partnerships to address the most urgent community health needs. Specifically, the authors of Public 3.0 stated, “Achieving the goal of Healthy People requires addressing social determinants of health, which includes both social and physical environments where people are born, live, work, and age” (U.S. Department of Health and Human Services, 2016, p. 7). This place-based travel course was designed to introduce students to historical and contemporary public health issues, their effects on population health, and how public health systems are working to address health issues in the very places where they are occurring.
Council on Education for Public Health
Additionally, this course was guided by course learning objectives and public health competencies outlined by Council on Education for Public Health (2018), “An independent agency recognized by the U.S. Department of Education to accredit schools of public health, and public health programs outside schools of public health” (para. 3). Learning objectives for the course included the following:
Identify root causes of both historical and contemporary public health issues across the southeastern United States and their effects on public health
Describe how health systems, public health agencies, and community-based organizations are addressing the social determinants of health across diverse cultures and communities
Compare and contrast the structure, programs, service delivery models, and approaches to addressing issues of public health of local, state, tribal, and federal health departments
Express critical thinking regarding the effects of politics on the policies and operations of public health systems
Demonstrate effective written communication skills
Compare and contrast the public health issues across the disciplines represented in the class and analyze the different approaches used to mitigate public health effects in the community
Foundational public health competencies linked to the above objectives advanced the value of performing effectively on interprofessional teams; recognizing the means by which structural bias, social inequities, and racism undermine health and create challenges to achieving health equity; and examining the systems and structures that either support or fail to support the function of public health.
Method
For this investigation, our team used a concurrent nested design, in which quantitative and qualitative data were collected simultaneously and integrated toward the end of the study (Creswell, Plano Clark, Gutmann, & Hanson, 2008). According to Creswell et al. (2008), the concurrent nested design features one predominant method that guides the project and one secondary method embedded within the predominant method that “addresses a question different from that addressed by the dominant method” (p. 184). Although we used a mixed methods approach, our priority study method was qualitative. A quantitative measure was embedded within the larger context of the study to examine student interest and comfort in working with, or on behalf of, MUPs. Combined, these two complementary methods provided a more robust analysis of students’ travel course experiences and reflected the multiple and frequently overlapping perspectives described by Pipitone (2018). A visual depiction of the concurrent nested design can be seen in Figure 1.

Visual depiction of concurrent nested design.
Data Collection and Analysis
Qualitative data consisted of students’ reflective journal entries, blog posts, and student presentations. Due to the exploratory nature of qualitative inquiry, the primary author used inductive coding to identify themes related to student experiences with the travel course. Data were organized using a text-to-table application in Microsoft Word and coded using the procedures outlined by Ivankova (2015). Line-by-line coding allowed the team to extrapolate recurring words and ideas from participants (McKinney & Morris, 2010). Emergent codes and themes were verified by both authors, and disagreements were discussed until consensus was reached. Additionally, we used multiple methods of verification to ensure trustworthiness of the data, including triangulation of data sources, peer debriefing, and maintaining an audit trail. Finally, we used reflexivity to clarify our own values, beliefs, and assumptions (Denzin & Lincoln, 2011). For quantitative data, students completed pre- and postcourse self-assessments regarding their interest and comfort in working with or on behalf of MUPs (1 = not interested to 5 = very interested). Results were averaged across students, and differences were calculated by hand. Due to the small sample size, preliminary findings are considered pilot data for a larger study.
Participants
Fifteen students participated in the travel course. The course was available to students at all degree levels and academic majors at the university. The composition of student participants included the following: undergraduate students (6), master’s-level students (8), and doctoral-level students (1). Students represented the following public health majors and/or concentrations: General Public Health (4), Health Education/Health Behavior (3), Maternal and Child Health (3), Environmental Health (2), and Epidemiology (1). Additionally, two students were dually enrolled in a master’s degree program that combines Health Care Organization and Policy and Business Administration. The broad distribution of students across academic majors supported the goals of the course and reinforces broad concepts for building capacity that leads to collective impact. Of the 15 student participants, only one self-identified as male; racial/ethnic descriptors were not collected. Due to the small number of participants, the team assigned pseudonyms to participants to ensure confidentiality. This project was reviewed by the University of Alabama at Birmingham Institutional Review Board (#300001578) and classified as quality improvement for course design.
Findings
Three overall themes emerged from our review of journal entries, blog posts, and student presentations; these themes reflected aspects of the three core principles that guided the course: (a) barriers to health equity, (b) contextualizing the social determinants of health, and (c) strategies for improving population health. For each theme, we provide subthemes and representative quotes to highlight findings.
Qualitative Results
Barriers to Health Equity
Characterizing their experiences of traveling in the Deep South, students frequently identified issues of (dis)trust within various communities and discussed how lack of trust can serve as a barrier to improving population health. Additionally, students described many of the challenges associated with funding public health initiatives throughout this region.
Issues of trust
Several participants reported learning about issues of (dis)trust between community members and the federal government based on a visit to the Salmon Testing Site, or Tatum Salt Dome, near Baxterville, Mississippi, the location of two underground detonations of nuclear weapons in 1964 and 1966. Despite efforts by the Mississippi State Department of Health’s (MSDH) Division of Radiological Health to educate and inform the population and screen for potential hazards, Deborah noted mistrust and skepticism among community members: “The population does not trust the government and has not for generations.” Students suggested that a lack of information and community buy-in before testing occurred had fostered a legacy of generational suspicion and fear: issues that were recurrent throughout the travel course.
Students also visited Tuskegee, Alabama, the site of the infamous Tuskegee Syphilis Study in which African American men in rural Alabama received a placebo treatment for syphilis under the pretext of receiving free health care from the U.S. Public Health Service between 1932 and 1972. Lori, who called the syphilis study a “gross violation of human rights,” said, “We were able to go to Tuskegee and talk to people who had been there and see relics from this experience.” She stated, Until I was there, until I talked to the children and the grandchildren of these men who had been in the study, until I visited the Greater Shiloah Baptist Church where these men were recruited for this study, it didn’t really hit home.
Despite previous class discussions about the Tuskegee Syphilis Study in undergraduate and graduate courses as well as a recognition of the historical importance of this clinical study in establishing ethical standards and human rights protections, Lori suggested that visiting the site affected her in ways that could not be replicated by a classroom encounter. Moreover, she intimated that the visit gave her and her peers a greater understanding of the deep-seated fears about patient experimentation, medical research, and the depersonalization of health care in the Deep South, fears that reverberate among many African American communities to this day. Wendy observed that historical injustices and social stigmas associated with disease prevention continue to make it difficult for states to effectively serve disenfranchised subpopulations in the Deep South.
Several students drew parallels between past and present policies for the containment of infectious diseases through a site visit to a former TB sanatorium (past) in Magee, Mississippi, as well as a visit to the University of Mississippi Medical Center’s (UMMC) Special Care Unit (present) in Jackson, Mississippi. Deborah noted that the quarantine policies of the past have informed biosafety regulations and ethical standards of today to “help protect the public from diseases, but (also) protect the rights of those with the disease.” Despite advancements in TB prevention and treatment as well as policies to protect an individual’s rights, Valerie recounted that a disproportionate number of TB cases in Mississippi affect African Americans. She suggested that this disease burden demonstrates that health outcomes can still be divided along racial lines.
Funding
Students commented on the ways in which politics, policies, and social values can limit access to and funding for health care services. Notably, three of the four states visited in this course—Mississippi, Alabama, and Georgia—rejected Medicaid expansion as part of the Affordable Care Act. While Wendy noted that Mississippi “barely squeaks by with the funds it receives,” others observed measureable financial shortfalls.
Andrea reported the challenges of the MSDH in distributing funds among multiple and competing priorities, noting that administrators could only use unencumbered funds that are a small fraction of the state’s overall public health budget “to put toward new initiatives and new programs that they thought would be the most beneficial for the people in their state.” She further noted that in fiscal year 2017, the state legislature cut 10% from these programmatic funds, which resulted in difficult decisions based on key state priorities and competing values. In one reflection statement, Jeremy noticed that the Public Health Laboratory, which conducts environmental and clinical testing services, was both understaffed and underresourced. Similarly, Rachel observed that the ongoing fight against TB in Mississippi was hampered by “budget cuts and lack of personnel.” Andrea summarized, “Having funding cuts, having to tighten up their belts, having people have to take on multiple roles when really new people should be hired . . . to expand those roles,” these are just a few of the realities of working in public health in the Southeast. Students identified similar challenges of state and federal funding across all four states in the Deep South.
Contextualizing the Social Determinants of Health
Across sites, students discussed the value of seeing firsthand the ways in which the social determinants of health influenced policy and practice and affected individual lives. The most obvious connections between social, environmental, and economic factors could be seen in a visit to the Lower Ninth Ward in New Orleans, Louisiana. Students described in detail the devastating and long-term effects of Hurricane Katrina, a destructive Category 5 hurricane that struck the Gulf Coast of the United States in 2005. Andrea observed, Before Hurricane Katrina (the Lower Ninth Ward) had a really high percentage of Black home ownership, and once the hurricane came through and just devastated people’s homes, the recovery efforts in that district are so different from what happened in the rest of the city. We were able to see how communities like the Lakeview district, all the houses were rebuilt—everything looked beautiful. People were able to retain the value and get back the things that they lost. Now, that community also happens to be predominately White and wealthy whereas the Lower Ninth Ward is still largely devastated.
Andrea noted that residents of the Lower Ninth Ward lost a tremendous amount of generational wealth due to the undervaluing of their destroyed homes. Moreover, students reported arresting health statistics between these two communities: “The average life expectancy in Lakeview is around 80 years old, whereas in the Lower Ninth Ward, it’s around 55 years old.” Students learned that the differences in life expectancy are due, in part, to racial homogeneity and a predisposition for heart disease as well as urban blight, violence, mobility, and access to health care (Somosot, 2012).
Normalized unhealthy behaviors
Visiting Bourbon Street in the French Quarter of New Orleans, Louisiana, Sarah expressed feelings of ambivalence and discomfort with the apparent contradictions in the city. On one hand, New Orleans generates a sizeable portion of its taxable revenue from tourism and recreation. However, many of the activities that draw people to the city also promote “behaviors that put at risk the health of those who work, live, and play” in these areas. She noted that many of the behaviors associated with the city’s nightlife (e.g., smoking, excessive drinking, solicitation) have become “normalized” for the sake of consumerism. Moreover, these activities occur in a state that has one of the highest rates of STIs and teen pregnancies, yet sex education in the public schools is neither mandatory nor widely encouraged.
Similarly, students explored the topics of obesity and nutrition at various locations, including a tribal health center at a federally recognized tribe in the Southeast. As a sovereign entity, students learned that the health facility is funded and operated separately from the state department of health. Holly described a health needs assessment the tribe developed, and noted that the top three health risks of tribe members were “diabetes, obesity, and hypertension.” To address these three priority issues, the tribe had formed subcommittees and developed activities, including “Work Out Wednesdays with the elders and a farmer’s market.” In addition to health and nutrition, Holly noted that alcohol and other substance use issues were also priorities for the tribe.
Interconnectedness of health
Throughout the travel course, students were continually reminded of the interconnectedness and interdependencies of health. Jeremy described this as the “One Health approach,” which recognizes that the health and well-being of humans is connected to the health of animals and the environment (Centers for Disease Control and Prevention [CDC], 2018). Tying global health to local health outcomes, Valerie described visits to the CDC and the Carter Center in Atlanta, Georgia, and the ways in which health practitioners combat Ebola and guinea worm in Africa by “overcoming cultural beliefs, religion, and distrust,” many of the same barriers that persist in the Deep South.
Valerie recalled stories of new cases of guinea worm in villages that had otherwise been free of the disease. She said that researchers discovered a new vector, “We’re seeing guinea worm in dogs . . . you would get rid of guinea worm in the human population, but now with the dogs getting it, it’s re-infecting the humans again.” Students observed that this phenomenon reinforced the One Health concept, citing “6 out of every 10 infectious diseases in humans are spread from animals” (CDC, 2018, para. 2). Valerie quoted one of the speakers at the Carter Center, stating, “We’re smarter together,” suggesting that eradicating diseases and solving complex public health problems requires interdisciplinary and cross-sector partnerships and collaboration.
Strategies for Improving Population Health
Students frequently commented on the value and importance of establishing partnerships to improve population health. Several students identified successful public–private partnerships as a strategy to reach the most vulnerable individuals. Others discussed how leaders had implemented program redesign and innovation to meet the needs of their existing clientele.
Collaborative partnerships
Rachel described the efforts of one community-based organization that collaborates with the MSDH, My Brother’s Keeper (MBK), in Jackson, Mississippi. MBK is a nonprofit organization dedicated to reducing health disparities in the community by engaging with the population, identifying community needs, and providing services to meet those needs. Rachel stated, “They (staff members) go out into the community to gain trust and create relationships so those who need help are more likely to seek help.” By developing trusting relationships and engaging with the population about HIV, for example, Lori suggested that staff members at MBK “reduce some of the stigma around HIV enabling folks to take part in preventive behaviors.”
In Louisiana, several students noted that the New Orleans Health Department had reorganized itself after Hurricane Katrina. Program administrators replaced their outdated model of direct health care service provision with one that emphasized community-based approaches to health care through a network of community partners and providers. According to Valerie, once the New Orleans Health Department acknowledged the duplication of services, “they shut down their health care clinics and let other organizations that were already offering the same services operate” with greater support and authority. This transition allowed the New Orleans Health Department to maintain a federally qualified health care center for its homeless population, which Valerie reported as a dire need for approximately 12,000 homeless men and women in the city, the composition of which reflected both the diversity and disparities of the city: African American (60%), White (30%), Latino (5%), and Vietnamese (3%; Statistical Atlas, 2018).
Citing a unique intra-agency collaboration, Sarah described a collaborative partnerships that comprised UMMC, the Special Care Unit that was created in response to the Ebola crisis in 2014, and UMMC/MEDCOM, a command center designed to “coordinate care across multiple hospitals in the state of Mississippi” in emergency situations. State officials described the purpose of these two units in preparing for and mitigating emergent natural and man-made disasters, including public health outbreaks. According to Sarah, this investment in prevention reflects one of the core values of public health. Erica further stated, “It was amazing to see how so many systems came together to coordinate an effective emergency response.”
Innovation
Students described the innovative nature of health care delivery through a one-stop model of care they witnessed in New Orleans, Louisiana. Our Daughters of Charity Health is a Catholic organization that has 10 clinics in New Orleans. These clinics offer free or low-cost, comprehensive, patient-centered health care to an underserved community with an eye toward eliminating barriers to health care for all of its patients. Students noted that one of the greatest obstacles to health care is reliable transportation. Our Daughters of Charity provides transportation for patients and schedules multiple appointments on the same day to maximize patient visits. Additionally, Our Daughters of Charity houses multiple service lines in the same location, which allows individuals to receive dental, vision, pediatric, gynecological, and other services in one place. Janet stated, Even the layout of the clinic reflects this same thoughtfulness for the population that they’re serving. They have the Women’s Clinic just across the hall from the pediatric clinic . . . also the Women, Infants, and Children (WIC) office, which provides nutrition services and the pharmacy are also housed in the same building.
Janet advocated for other clinics in the United States to consider this model of coordinated services by colocating clinics. She regarded the intentional design and functionality of clinics as a first step toward understanding patient needs and eliminating barriers to health care access for vulnerable populations.
Like Our Daughters of Charity in Louisiana, Felicia noted that the Escambia County Health Department in Alabama also recognized transportation as a barrier to patients in rural areas and had therefore initiated the “Wheels to Wellness” program to provide patients with dependable transportation to doctor’s appointments. She reported that program administrators were starting to use telehealth technology to provide remote doctor–patient consultations. “Telehealth is great for high risk OB (obstetrics) patients,” she said, because it allows physicians to monitor vital signs of the mother and fetus without contributing to the stress burden of unnecessary travel.
Quantitative Results
Students who participated in this travel course were required to complete pre- and postcourse self-assessments to determine their interest and level of comfort in working with, or on behalf of, medically underserved populations. As shown in Table 2, students reported a slight increase in their level of interest in working with MUPs (0.3) and greater comfort in working on behalf of MUPs (0.6). Due to the small sample size, these data demonstrate trends rather than statistical significance therefore caution should be used when interpreting results.
Interest and Level of Comfort in Working with Medically Underserved Populations.
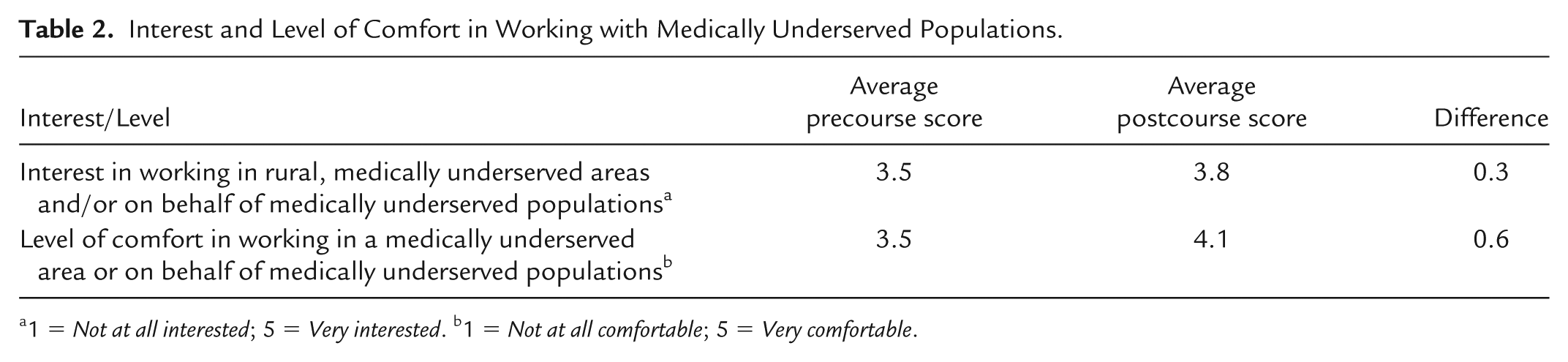
1 = Not at all interested; 5 = Very interested. b1 = Not at all comfortable; 5 = Very comfortable.
Discussion
In spring 2018, 15 students from the UAB traveled to sites throughout the Deep South to learn more about the ways in which history and place interact with programs, policies, and practices to influence population health. Students saw firsthand how the social determinants of health frequently affected access to health care and discovered the value of a multidisciplinary approach to public health and health programs in addressing health equity. Data analysis yielded barriers to health equity, contextualizing the social determinants of health, and strategies for improving population health as the three primary themes; the ways in which these concepts were presented through student reflections and writings offer greater insights into student experiences with the travel course.
Throughout this travel course, students identified challenges to health access and health equity including inadequate funding for programs and services as well as widespread distrust among local communities. While some communities, like Baxterville and Tuskegee, continue to be affected by historical injustices, others, like Jackson, are stridently working to build trusting relationships through community outreach. Students described the interconnectedness of health outcomes through the concept of One Health, noting that a healthy environment, healthy animals, and healthy people are inextricably tied to one another, and observed how behaviors and culture are frequently context-specific and require unique strategies and solutions to address community needs. Finally, students recognized the challenges of systemic racism, widespread poverty, and educational disparities and saw how these social determinants of health affect public health and contribute to poor health outcomes. Students observed the value of systems thinking in addressing complex and deeply embedded social norms and practices and observed how multiple systems interact with public health to improve health outcomes.
Quantitative data suggested that the travel course may have influenced student interest and comfort in working with, or on behalf of, MUPs, but the small sample size and lack of gender diversity limits our ability to interpret results beyond practical utility and program improvement. Additionally, the students who were most likely to register for this course may have been predisposed to working with rural or underserved populations before the travel course. Nevertheless, these results are encouraging in light of projected workforce shortages in underserved, remote, and poor areas in the United States (Huicho et al., 2010).
We believe this travel course allowed students to put a face on public health, both literally and figuratively, and to recognize the challenges that many communities in the Deep South face, including conditions and health outcomes in some areas that rival those of Third World countries. Consistent with findings by Pipitone (2018), we observed the value of “place” in constructing valuable and meaningful learning spaces for students to engage with local populations and draw on their stories, histories, customs, and values to better understand the complex nature of health and health care in rural and underserved areas.
As an experiential form of learning, the travel course provided students an immersion experience that allowed them to delve deeply into the realities of serving at-risk populations with limited human and financial resources. For some, the course affirmed their desire of working with disenfranchised populations; for others, it challenged them to consider the day-to-day experiences of public health practitioners in rural or remote locations and reflect on their willingness and interest in working under such conditions. Irrespective of outcome, the course met its intended outcomes for experiential education: engagement and active learning (Knowles, 1980).
Implications for Public Health Practice
The authors of Public Health 3.0 (U.S. Department of Health and Human Services, 2016) recommended that emerging and current public health practitioners become “strategists” within the communities they serve to promote health efforts across disciplines. For the students who participated in this travel course, becoming a strategist meant developing a broad network of contacts and coalitions to leverage the critical knowledge of communities to influence health policy and advance positive behavior change among individuals. Students observed that affecting change requires participation from more than just public health practitioners. As demonstrated through this place-based course, community-based health interventions may involve tribal elders and other respected community leaders, educators, policy makers, volunteers, and more.
Through this travel course, students developed a greater awareness of how diversity and culture, including history, values, and beliefs, affect public health in various areas of the Southeast. Students recognized the value of cross-disciplinary approaches for understanding and thereby addressing complex public health issues. Finally, students observed the passion and commitment of individuals working in public health settings and discussed how these attributes, combined with data and evidence-based practices, can begin to mitigate the social determinants of health. This place-based course provided valuable context for public health students to connect concepts from the classroom with public health practice in the field and to prepare themselves for their future roles in the public health workforce.
Best Practices for Academia
While this travel course was designed to address public health issues in the Deep South, we propose that the course design could be replicated in other settings and with other academic majors. We would encourage instructors and course designers to prepare students and provide opportunities for discourse before, during, and after the travel portion of the course, as immersion experiences tend to place students in new and frequently uncomfortable situations. Organizers are encouraged to work closely with their university travel abroad offices to discuss resources for logistics and support. Consistent with best practices in study abroad/away, strategies for processing the experience may include predeparture discussions about differing cultural norms and awareness of one’s own biases and preconceptions as well as daily debriefing sessions throughout the experience and postcourse reentry (Donnelly-Smith, 2009).
Additionally, since reflection is a critical component of the learning experience (Walzer-Kuntz & Iroz, 2017), we recommend that instructors spend sufficient time with students before the travel portion of the course discussing the difference between “reflecting” and “reporting” of events. In fact, instructors may want to review the first one or two student reflections during the trip and provide feedback to reinforce concepts and make recommendations for improvement. Finally, instructors should identify opportunities for students to share their experiences in meaningful ways with campus and community constituents. Outlets may include student presentations, blog posts, and/or campus media. Dissemination of student experiences may generate student interest for future travel course offerings and solidify institutional buy-in and financial support for long-term program sustainability.
Conclusion and Next Steps
Contemplating the quote by Santayana in relation to this travel course, Wendy stated, “If we want to create successful public programs, we need to understand the history of the communities we’re working with . . . the fears, the distrust and the overall health experiences of these individuals.” We assert that this reflection perfectly captures the value and importance of place-based education in preparing students for the realities and challenges of addressing complicated public health issues in the Deep South. Furthermore, as schools and programs of public health continue to recognize the value of out-of-classroom learning, it compels all of us to become more intentional about designing future curricular innovations.
UAB is planning to build on the foundation laid through this domestic, place-based course by offering both domestic and international courses to explore issues of population health. Ultimately, students will have the opportunity to engage with the practice community through visits to multiple venues in the United States and across the world. These course offerings will allow students to develop a greater understanding of health issues across differing communities and to truly consider why place matters. Opportunities, like the one described in this article, give students a platform to explore and develop a better understanding of root causes of both historical and contemporary public health issues and their effects on population health today.
Footnotes
Acknowledgements
The authors would like to thank the University of Alabama at Birmingham (UAB) Quality Enhancement Plan Teaching and Learning Development Grant Program, the UAB Center for Teaching and Learning, and the staff of the UAB School of Public Health Office of Public Health Practice for supporting the development of this course. The authors would also like to thank Meena Nabavi, MPH, who served as a teaching assistant for this course. Meena and Sabrina K. Hagen worked tirelessly and expertly to arrange the logistics for this 2-week travel course through the Deep South.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.