
Abstract
Community-based participatory research (CBPR) is widely recognized as an effective approach to understand and address health inequities. Opportunities for public health practitioners and researchers to engage jointly with community partners in intensive colearning processes can build capacity for CBPR. Using active learning approaches that engage diverse partners can enhance partnership development, competence, and equity. Examination of such pedagogical approaches can strengthen understanding of their contributions to the effectiveness of CBPR capacity-building programs. This article describes a weeklong intensive course carried out by the Detroit Urban Research Center as the foundation for a yearlong training program to build the capacity of community-academic partnership teams to engage in CBPR in their own communities. The in-person CBPR course was developed and implemented by expert academic and community instructors and used an experiential action learning model that integrated CBPR principles and processes. We describe the course content and application of our collaborative, experiential action learning model to course design; present results from participant evaluation of course effectiveness, CBPR competence, and equitable partnership development; and examine the contributions of the pedagogical approach to outcomes central to successful CBPR. The participatory, formative course evaluation used multiple methods that included closed- and open-ended questionnaires to assess instructional effectiveness, participant competence on 12 core components of CBPR, and course impact on partner relationships. Evaluation findings suggest that an experiential action learning approach with attention to colearning, collaboration among diverse instructors and participants, and an environment that fosters and models equitable and trusting relationships can be effective in building CBPR capacity.
Community-based participatory research (CBPR), with its emphasis on equitable and collaborative partnerships among diverse constituencies, is widely recognized as an effective approach to address health inequities and has been identified as a core competency for public health professionals to address the major health problems facing society (Freudenberg, Klitzman, Diamond, & El-Mohandes, 2015; Gebbie, Rosenstock, & Hernandez, 2003; Neiworth, Allan, D’Ambrosio, & Coplen-Abrahamson, 2014). Although CBPR training materials and a number of courses have been developed in the United States in recent years (Canfield et al., 2016; Masuda, Creighton, Nixon, & Frankish, 2011; van Olphen et al., 2015; Israel, Coombe, & McGranaghan, 2018), few provide opportunities for public health professionals and researchers to engage jointly with community partners in a colearning process facilitated by experienced community-academic instructor teams (Andrews et al., 2013). Active learning approaches in which participants are engaged in experiences to gain and apply knowledge to real situations, and in which diverse participants learn with and from each other, can contribute to attaining objectives such as partnership development, equity, and collaboration (Cunningham, 1998; Johnson & Johnson, 2017; Kolb, 2015; Reinschmidt, Maez, Iuliano, & Nigon, 2019). We know of few examinations of how such a learning model and pedagogical approach may contribute to the effectiveness of a course in enhancing capacity to engage in CBPR (Reinschmidt et al., 2019; Rubin et al., 2012).
This article describes a weeklong intensive course carried out by the Detroit Urban Research Center (Detroit URC) as the foundation for the CBPR Partnership Academy, a yearlong national training program aimed at building the capacity of community-academic partnership teams to engage in CBPR in their own communities (see Coombe et al., 2020, for a description of the program). Participants were pairs of one community and one academic partner new to CBPR who applied and were selected for the yearlong program through a nationally competitive process. The foundational in-person course on CBPR was developed and implemented by expert academic and community instructors and used an experiential action learning model that integrated CBPR principles. The purpose of this article is to describe the course content and our learning model as it informed the course design; present results from participant evaluation of course effectiveness, learning, and partnership development; and examine the ways in which the learning model and pedagogical strategies contributed to outcomes that are central to successful CBPR. We discuss implications for the development of training curricula to enhance the capacity of academics, public health and health promotion professionals, and communities to develop equitable partnerships for CBPR.
Background
Community-Based Participatory Research
CBPR is a partnership approach to research that equitably involves community members, organizational representatives, public health and other practitioners, and researchers in all aspects of the research. All partners contribute expertise and share decision making and ownership to increase knowledge and understanding of a phenomenon and integrate that knowledge with interventions, policy advocacy, and social change to improve quality of life for communities and reduce health inequities (Israel et al., 2019; Israel, Schulz, Parker, & Becker, 1998). Its applicability to interventions, policy change, evaluation, and sustainability make CBPR especially relevant in health promotion and public health fields (Israel, Eng, Schulz, & Parker, 2013b; Wallerstein, Duran, Oetzel, & Minkler, 2018). Below we describe a course designed specifically to create opportunities for community, academic, and public health practitioner partners to engage in an intensive colearning process designed to strengthen capacity to use CBPR in their work. The course was informed by pedagogical principles that are synergistic with CBPR, with the goal of strengthening capacity and colearning among diverse public health practice, academic, and community partners (Freudenberg et al., 2015; Rubin et al., 2012).
The Detroit Community–Academic Urban Research Center (Detroit URC)
The Detroit URC is a long-standing partnership that fosters health equity through CBPR. Established in 1995, the Detroit URC aims to facilitate and support the establishment of CBPR partnerships to enhance understanding of how social and physical environments affect health and to translate that knowledge into interventions, programs, and policies that build on community resources and strengths to promote health equity. The center is directed by a board composed of representatives from partner organizations: nine community-based organizations, the city health department, an integrated health care system, and a university (see Acknowledgments; Israel et al., 2019). The Detroit URC has fostered and supported more than 75 CBPR partnerships across multiple disciplines, conducting more than 100 research projects on critical health issues. Center members conduct workshops nationally and internationally and have mentored and trained hundreds of researchers, practitioners, and community members in CBPR. Building on this experience, in 2014, the Detroit URC established the CBPR Partnership Academy, an integrated, yearlong applied learning program to enhance the capacity of new community-academic partnerships. The foundation of this national program is a weeklong course in CBPR, which is the focus of this article.
Community-Based Participatory Research Partnership Academy
The Detroit URC conducted the CBPR Partnership Academy, a capacity-building research education program for pairs of academic researchers and community partners new to CBPR, carried out from 2014 to 2019 and funded by the National Institute of General Medical Sciences, Award #1R25GM111837 (see Coombe et al., 2020). Participants were selected through a nationally competitive process by a committee of community and academic experts in CBPR. The CBPR Partnership Academy was composed of an intensive in-person short course in CBPR followed by a yearlong program of mentoring, online learning activities, development of CBPR partnerships/projects in participants’ communities, an ongoing community–academic scholars network, and subsequent program-wide dissemination. Three cohorts of 12 teams each completed this process. In the final year, all three cohorts were involved in webinars, networking, and an Academy-wide symposium to enhance and sustain participants’ CBPR skills beyond the yearlong program. The final year also focused on evaluating the short- and long-term success of the program and on disseminating the knowledge gained, curriculum, and materials. A detailed description of the overall program, individual components, and evaluation of the first 2 years has been provided elsewhere (Coombe et al., 2020). This article focuses on the curriculum, pedagogy, and evaluation of the weeklong intensive course, to provide a more in-depth understanding of how the course elements and pedagogy contributed to participant learning.
Conceptual and Pedagogical Framework
Community-Based Participatory Research Approach
The CBPR Partnership Academy, including the weeklong intensive course, was developed, implemented, and evaluated using a CBPR approach that involved highly regarded academic and community partners with years of CBPR experience. In accordance with the CBPR principles adopted by the Detroit URC Board, all activities were carried out using approaches that built on the diverse strengths of all partners and fostered synergy, equity, colearning, empowerment, and long-term sustainability (Israel et al., 1998; Israel et al., 2017). In keeping with these CBPR principles, all training, evaluation, and dissemination activities were carried out jointly by academic and community partners.
Experiential Action Learning Model Within a CBPR Approach
The Partnership Academy was guided by a long-standing experiential action learning model (Browner & Preziosi, 1995; Cunningham, 1998; Johnson & Johnson, 2017; Kolb, 2015). The five core principles and assumptions of this model for capacity-building and health promotion programs are that learning is (1) more meaningful when participants are actively involved in real experiences that require solutions, (2) more effective when participants are engaged in experiences to gain and then apply knowledge, (3) enhanced when participants develop strategies to address a problem and reflect on their decisions, (4) improved when participants learn with and from one another, and (5) more likely to change knowledge, behavior, and attitudes when participants are actively involved in the process (Cunningham, 1998; Johnson & Johnson, 2017; Kolb, 2015).
In addition to these five principles, experiential learning has more recently included several other concepts that are central to our learning model for CBPR. One concept is that experiential learning is centered in collective experiences with others in a context within which individuals bring their own experiences and may develop shared or different understandings (Pau & Mutalik, 2017). Furthermore, an educational approach termed “community-engaged pedagogy” (Reinschmidt et al., 2019; Rubin et al., 2012) includes the principle that effective experiential action learning both relies on and builds relationships among a diverse community of learners and instructors. These concepts align with the core CBPR principles of colearning and attention to equity among diverse partners (Israel et al., 1998; Israel et al., 2013b). Colearning facilitates the reciprocal transfer of knowledge, skills, capacity, and power. Attention to equity involves empowering and power-sharing processes that recognize and attend to social inequalities. Thus, our model of experiential action learning in the context of CBPR modifies the long-standing model by adding two principles, that learning is enhanced when (6) relationships and a community of learners are built through collective colearning experiences and (7) diverse faculty and community partners engage collaboratively and equitably.
Accordingly, the Partnership Academy course applies these seven principles of our pedagogical framework to create new understandings and skills for applying a CBPR approach to research. The course uses a number of active learning strategies, combining didactic methods with interactive activities, group discussions, problem-solving tasks, reflection, and feedback. Learning activities are layered to encompass individual, dyadic, small-group, clusters of teams, and entire-group learning opportunities in order to provide a variety of supportive environments for sharing and risk taking (Masuda et al., 2011) and to generate new understandings through interaction. The model recognizes learning as a continuous cycle of knowledge acquisition, experience, observation, and reflection; development of concepts and generalizations; and integration and application of these concepts and generalizations to real-life situations (Kolb, 2015).
Methods
CBPR Intensive Weeklong Course Design and Implementation
Overview of the Course Curriculum
To establish a strong foundation, the yearlong program begins with an intensive CBPR course at the University of Michigan in Ann Arbor, taught by expert academic-community teams from the Detroit URC. The course curriculum enhances knowledge and skills in partnership development, research designs and methods using a CBPR approach, equity and cultural humility, ethics in research, and partnership evaluation. Community instructors facilitate a site visit to Detroit highlighting CBPR partnerships and the long-standing leadership of community organizations.
Pedagogical Approach and Instructional Methods
In keeping with our experiential action learning model, the intensive course uses multiple learning methods and tools to achieve the program goals. These include interactive didactic methods, team hands-on activities and relationship-building opportunities, small-group exercises, slide presentations, discussions, role plays, word cloud tools, hypothetical case studies, practical application of research-related tasks based on actual case examples, analysis of readings, personal reflection, and a site visit. Participants are expected to complete the readings (see below) and engage actively in discussions. Applying the principles of experiential action learning throughout, all course sessions encourage participants to ask questions, share their own experiences, reflect on the application of learning in their own communities, explore issues and challenges related to equity and research ethics, and consider the implications for their professional development. Each session is cofacilitated by an academic and community instructor team. Participants have opportunities to work together both within their community-academic pairs and with other teams to develop their partnerships and discuss next steps. Activities foster peer knowledge sharing and relationship building to develop an ongoing network of community and academic practitioners of CBPR.
Instructors
The course was developed, implemented, and evaluated using a CBPR approach, involving highly regarded academic and community partners with years of experience. Eighteen community and academic instructors were involved, representing multiple racial, ethnic, and gender identities and specializing in diverse research disciplines. Fifty-six percent (56%) of the instructors are persons of color (23% African American, 33% Latino/a), and 72% are women. All instructors specialize in CBPR, with 39% currently serving or having recently served in a leadership role at a community-based organization or health and human services agency. They are leaders in their fields and are addressing contemporary public health issues, including cardiovascular disease, diabetes, asthma, and socioeconomic and environmental contributors to health inequities, such as air pollution, water quality, and climate change.
Course Objectives and Expected Competencies
Organized along the phases of CBPR (Israel, Eng, Schulz, & Parker, 2013a), the course aims to enhance participant knowledge and skills in all aspects of CBPR, and it includes strategies to ensure timely career advancement while using this approach. Table 1 lists the course’s learning objectives toward achieving core competencies of CBPR.
Intensive Weeklong Course in Community-Based Participatory Research (CBPR): Learning Objectives Derived From CBPR Competencies.

Source. Israel, Coombe, & McGranaghan (2018).
Curriculum and Instructional Activities
In this section we provide a brief description of the content covered each day, with examples of the experiential learning activities used. All activities apply our experiential action learning model and pedagogical approaches as described above, and most course sessions integrate multiple pedagogical strategies. The curriculum as a whole reflects the overarching principle that learning is more meaningful, effective, and enduring when participants work together in a collaborative environment to apply learning to their own experiences (Kolb, 2015).
Day 1: CBPR rationale, principles, and partnership development; introductions and team building; responsible conduct of research
Morning
An overview of CBPR is provided, including its definition, rationale, principles, and phases, and strategies for partnership formation, maintenance, and sustainability. In small groups, participants identify and select partners for a hypothetical case study using a set of key questions, such as who should be invited to partner on this grant application and why, and how the partnership would be structured. This session also addresses the benefits of, challenges in, and barriers to applying a CBPR approach to research; facilitating factors for overcoming these challenges; and lessons learned from the experience of the Detroit URC. Equity, ethical conduct of research, and cultural humility are highlighted as integral to CBPR and addressed throughout the course.
Afternoon
The teams are introduced to one another, and relationships within and across teams are strengthened through an interactive team-building activity. In pairs, each team develops a 3-minute presentation that includes one strength each team member brings to the partnership, a brief description of their partnership focus, and a symbol or drawing that represents their community. In the large group, teams present their partnership and share their drawings in an engaging and positive atmosphere. In the second part of the afternoon, formal instruction is provided in responsible conduct of research for a community-academic audience that fulfills the institutional requirements for Human Subjects Protections. The 90-minute session includes four interactive learning strategies in which participants reflect on the role of ethics in research, apply the Belmont principles (National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research, 1978) to actual cases of violations, practice responding to ethically questionable researcher requests, and generate ethical issues relevant to their particular communities.
Day 2: Survey methods in CBPR; mixed methods in CBPR
Morning
Describe and analyze the application of a CBPR approach in conducting survey research, using a case study from Community Action Against Asthma (CAAA), a Detroit URC-affiliated partnership focused on air quality and childhood asthma (Parker et al., 2013). Session topics include an examination of survey design and implementation using CBPR; a description of the roles that partners play in the process; and an analysis of the lessons learned and implications and recommendations for using CBPR in projects involving surveys. In small groups, participants role-play a discussion about using an existing validated questionnaire that community partners have concerns about, then work together to draft alternative questions that are acceptable to both academic and community partners.
Afternoon
Examines the relevance and application of mixed methods research in CBPR, particularly to study and address complex public health problems (Creswell & Plano Clark, 2017). An actual case example is used throughout to illustrate the process and content of a mixed method study using CBPR. Topics include the rationale for using mixed methods in CBPR, timing and sequencing of mixed methods in the study design, methods for combining the strengths of both quantitative and qualitative methods, and integration strategies for analyzing and presenting results using mixed methods. Teams apply learning to their own partnerships in a three-part iterative small group activity to develop the research question, identify data to answer the question, and develop a data collection design that integrates qualitative and quantitative methods.
Day 3: Focus groups in CBPR; innovative research design in CBPR
Morning
The use of focus group interviews in the context of CBPR is described and analyzed. The session addresses why and when to use focus group methodologies; steps in planning and conducting focus groups and the functions of the steering committee; how to involve all partners in feedback, interpretation, and dissemination of results; and lessons learned and recommendations for using focus group interviews within the context of CBPR (Kieffer et al., 2013). Participants apply material through a role play in which a hypothetical partnership plans a focus group process to design a community-based intervention. After participants share their models and processes, the instructors describe how a Detroit URC–affiliated partnership, Racial & Ethnic Approaches to Community Health, used focus groups to plan and evaluate multilevel interventions to prevent and address diabetes.
Afternoon
This session discusses challenges and limitations in using randomized control trials (RCTs) for community interventions conducted within the context of a CBPR approach, and it presents and analyzes innovative research designs that complement or serve as viable alternatives to RCTs (e.g., randomized staggered/lagged intervention). Examples of CBPR intervention studies by Detroit URC–affiliated partnerships that apply innovative and viable research designs and rigorous methods are discussed. Active discussion throughout is facilitated by questions posed by participants and instructors.
Day 4: Interpreting, applying, and disseminating results to inform community change; research design and statistical methods in CBPR; site visit to Detroit
Morning
The session describes and analyzes the roles of community partners in interpretation, analysis, and action planning based on findings from the Healthy Environments Partnership (Schulz et al., 2011) and Community Action to Promote Healthy Environments, two Detroit URC–affiliated partnerships that address the combined influence of physical and social environments on health. Dissemination guidelines are described, with specific examples of how community members have been actively engaged in interpreting, analyzing, and setting action priorities based on data from multiple sources, determining policy strategies and disseminating results to policymakers, and translating research findings in order to develop interventions to reduce air pollution and promote health. Participants work in small groups to review and interpret research findings and to prioritize actions toward achieving community goals by applying a CBPR approach similar to the one described.
Afternoon
Statistical methods and issues are described—including integrating multilevel data—as applied to innovative research designs that complement RCT designs. Participants apply sampling concepts in small groups, then later apply study design concepts to their previous activity in an iterative process. In the afternoon and evening, participants make a site visit to Detroit, facilitated by community instructors, highlighting select Detroit URC partner organizations engaged in CBPR. Being in the community grounds the classroom CBPR learning in communities’ strengths, resources, and challenges and demonstrates the role of long-term community leadership in working with academic researchers to develop and implement strategies to address health and equity. Having dinner in Detroit further strengthens relationships and builds networks among participants and instructors/mentors.
Day 5: In-depth interviews and partnership evaluation in CBPR; short-course evaluation; next steps, reflections, and celebration
Morning
The session examines the purpose of and conceptual framework for the evaluation of CBPR partnerships. The use of in-depth interviews within a mixed methods design for evaluating the process and impact of partnerships using a formative approach is examined. Topics discussed include the data collection and analysis process, the role of all partners in conducting the evaluation, the feedback and incorporation of evaluation results to improve partnership functioning, and lessons learned. Using a hypothetical partnership as a case example, participants develop an evaluation plan and sample interview questions in small groups, which they then share across groups. At the end of the morning session, participants complete an open-ended questionnaire to evaluate the course.
Afternoon
This session presents content and format for the integrated yearlong activities, including small planning grants, monthly online learning forums, and mentoring. The week culminates with a celebration and opportunities for photos and video reflections.
Educational Materials
Participants receive a course syllabus and a copy of the book Methods for Community-Based Participatory Research for Health (Israel et al., 2013b). All slide presentations, a course pack of selected readings, examples of forms and materials developed by Detroit-based CBPR partnerships (e.g., dissemination guidelines, evaluation questionnaires), career development tools, and a resource guide to CBPR are provided in both hard copy and electronic form. A Partnership Development Checklist is provided to assist Partnership Academy teams in documenting and evaluating their activities and to facilitate mentor discussions. All instructional resources are also provided through an online learning management system and repository (Canvas).
Course Evaluation Methods
Purpose, Approach, and Design
The purpose of the course evaluation was to assess implementation process and outcomes—including course effectiveness in enhancing CBPR competence and equitable partnership development—and to examine ways the pedagogical approach may have contributed to those outcomes. The course evaluation was one component of the overall evaluation of the CBPR Partnership Academy, as described elsewhere (Coombe et al., 2020). The participatory and formative evaluation involved program instructors, staff, and the Detroit URC Board to prioritize research questions, decide on measurement tools and methods, and interpret and apply findings to make improvements (Coombe, 2012; Cousins, 2012). Process evaluation examined the implementation of activities to understand how and why aspects of the program were more or less effective. Outcome evaluation assessed the aims of the course, for example, enhanced CBPR capacity, and the contribution of activities to program success.
The multiple methods design used measurement tools developed by the program team, including two course evaluation questionnaires, program documentation, and group discussion. All participants completed a pencil-and-paper open-ended questionnaire on the last day of the course. A second questionnaire with closed- and open-ended questions was administered a week following the course, using Qualtrics Survey Software, Version 2018 (Qualtrics, Provo, UT).
Closed-ended measures of instructional effectiveness included seven items to assess the quality and usefulness of the content, organization, instruction, and materials. CBPR competence (knowledge, skills, and understanding; Israel et al., 2013a) was self-assessed on 12 key components of CBPR. Closed-ended survey items were rated on a 5-point Likert scale, from 1 = strongly disagree to 5 = strongly agree. Open-ended questions asked about what was the most and least valuable/beneficial, recommendations for improving the course, the beneficial aspects of the Detroit trip, and the impact of the course on the relationship between partners.
Data Analysis
Descriptive statistics were generated using Qualtrics and Stata Statistical Software, Version 15.0 (StataCorp LLC, 2017). We calculated the mean and standard deviation (SD) for each survey item. To determine the differences between cohorts, we used a Wilcoxon rank-sum test (de Winter & Dodou, 2010) to compare the average response for each question between Cohorts 1 and 2 and between Cohorts 2 and 3. A Bonferroni correction was applied within each question to account for multiple comparisons being performed simultaneously (Dunn, 1961). Seventy of the 74 participants completed the Qualtrics questionnaire administered a week after the course. All participants completed the open-ended questionnaire administered on the last day. Qualitative data from both questionnaires were analyzed by a grounded theory method of open thematic coding using verbatim language and grouping content conceptually using constant comparison (Charmaz, 2014).
Results
We present participant characteristics and course evaluation results for instructional effectiveness, CBPR competence, the most beneficial aspects of the course, qualitative findings aligned with experiential learning principles and strategies, and the least beneficial aspects/recommendations. Quantitative results are presented by and across cohorts, indicating significant differences bet-ween cohorts. As a formative evaluation, the results were shared with the presenters, and the course was modified accordingly.
Participant Characteristics
Three cohorts, each composed of 12 community–academic pairs, completed the course. The 72 participants (36 two-person community-academic teams) reflected multiple dimensions of diversity, including 18 states and two tribal nations and rural, urban, suburban, and island communities, with 68% from racial and ethnic groups underrepresented in research (e.g., African American, Latino/a, Native American, Native Hawaiian, Arab American, Southeast Asian). Seventy-two percent of the participants were women; of the academic participants, 83% were women. The academic participants represented multiple disciplines, including public health, environmental sciences, urban planning, psychology, sociology, epidemiology, biostatistics, medicine, and nursing. The community participants included nonprofit, advocacy, and health care organizations. The teams represented diverse communities of identity and interests, including multiple racial/ethnic identities, immigrants, low-income workers, homeless persons, and youth. All three cohorts were comparable in CBPR experience and demographic characteristics.
Course Instructional Effectiveness
Participant assessment of instructional effectiveness related to organization, instructors, resources, and activities is presented in the first section of Table 2. Mean ratings for all items are presented separately for each cohort. In addition, we compared cohorts to determine whether there were statistically significant differences between Cohorts 1 and 2 and between Cohorts 2 and 3, indicated by p values.
Course Instructional Effectiveness and Self-Assessed CBPR Competence: Comparison of Evaluation Findings Across Cohorts.
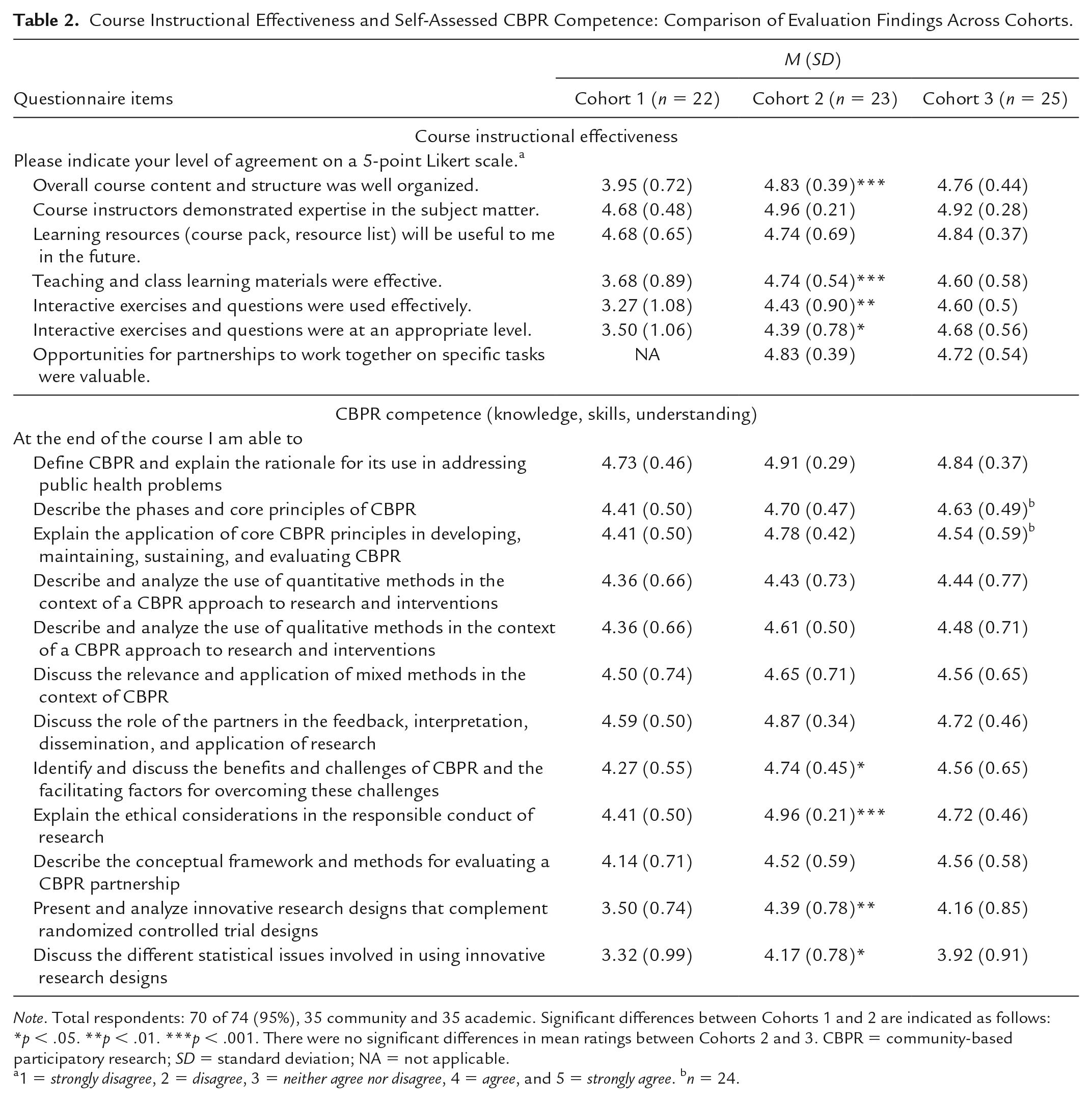
Note. Total respondents: 70 of 74 (95%), 35 community and 35 academic. Significant differences between Cohorts 1 and 2 are indicated as follows: *p < .05. **p < .01. ***p < .001. There were no significant differences in mean ratings between Cohorts 2 and 3. CBPR = community-based participatory research; SD = standard deviation; NA = not applicable.
1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, and 5 = strongly agree. bn = 24.
Mean responses were at or above 4.68 (agree/strongly agree) in all three cohorts for two indicators of course effectiveness: instructors’ expertise (ranging from M = 4.68, SD 0.48 to M = 4.96, SD 0.21) and the future usefulness of learning resources (ranging from M = 4.68, SD 0.65 to M = 4.84, SD 0.37). For all four other indicators of instructional effectiveness, mean responses were below 4 in Cohort 1 (M ranged from 3.27 to 3.95) but improved significantly to above 4 in Cohort 2 (M = 4.39, SD 0.78 to M = 4.83, SD 0.39), as shown in Table 2. Scores remained high in the third cohort for all 12 instructional effectiveness measures. The greatest improvements from the first to the second cohort were in overall organization of course content and structure (from M = 3.95, SD 0.72 to M = 4.83, SD 0.39) and effective use of teaching and learning materials (from M = 3.68, SD 0.89 to M = 4.74, SD 0.54), significant at p < .001. Items about whether interactive questions and exercises were used effectively and at an appropriate level each were rated somewhat lower than other aspects of instruction among the first cohort (M = 3.27 and 3.50, respectively) but improved significantly in the second cohort (M = 4.43, SD 0.90** and M = 4.39, SD 0.78*, respectively). In the second year, we added a question to assess the value of opportunities for partnerships to work together, a core aspect of experiential action learning pedagogy, and it was rated highly in both Cohorts 2 (M = 4.83, SD 0.39) and 3 (M = 4.72, SD 0.54).
Self-Assessed CBPR Competence (Knowledge, Skills, and Understanding)
Participants assessed their competence on 12 core components of using a CBPR approach, which also aligned with the course learning objectives. The competence items assessed participants’ knowledge, skills, and understanding in response to the statement “At the end of the course I am able to . . .” Results are shown in the second section of Table 2. For all three cohorts, mean scores were greater than 4 (agree) on 10 of the 12 competence indicators (M = 4.14, SD 0.71 to M = 4.96, SD 0.21). For the other two indicators, mean assessments were below 4 for the first cohort only and significantly higher for the second cohort: ability to understand innovative research designs such as randomized staggered intervention designs (Cohort 1 M = 3.50, SD 0.74 and Cohort 2 M = 4.39, SD 0.78**) and statistical issues in innovative research designs (Cohort 1 M = 3.29, SD 0.99 and Cohort 2 M = 4.17, SD 0.78*). Mean assessments were also significantly higher for Cohort 2 than for Cohort 1 on two other competencies, (1) identify benefits, challenges, and facilitating factors (Cohort 1 M = 4.27, SD 0.55 and Cohort 2 M = 4.74, SD 0.45, p < .05) and (2) explain ethical considerations in responsible conduct of research (Cohort 1 M = 4.41, SD 0.50 and Cohort 2 M = 4.96, SD 0.21, p < .001). There were no differences in mean scores between Cohorts 2 and 3 on any competencies.
Most Beneficial Aspects of the Course
Table 3 presents qualitative findings across all three cohorts from open-ended questions asking what was most valuable/beneficial about the course, in what ways the Detroit trip was beneficial, and how the course affected the relationship between partners. Nine themes that emerged from the data are presented in the table as summary statements, and selected responses that exemplify the themes are presented below each theme.
Qualitative Evaluation Results: Most Beneficial Aspects of the Course by Themes and Illustrative Responses (Cohorts 1–3).
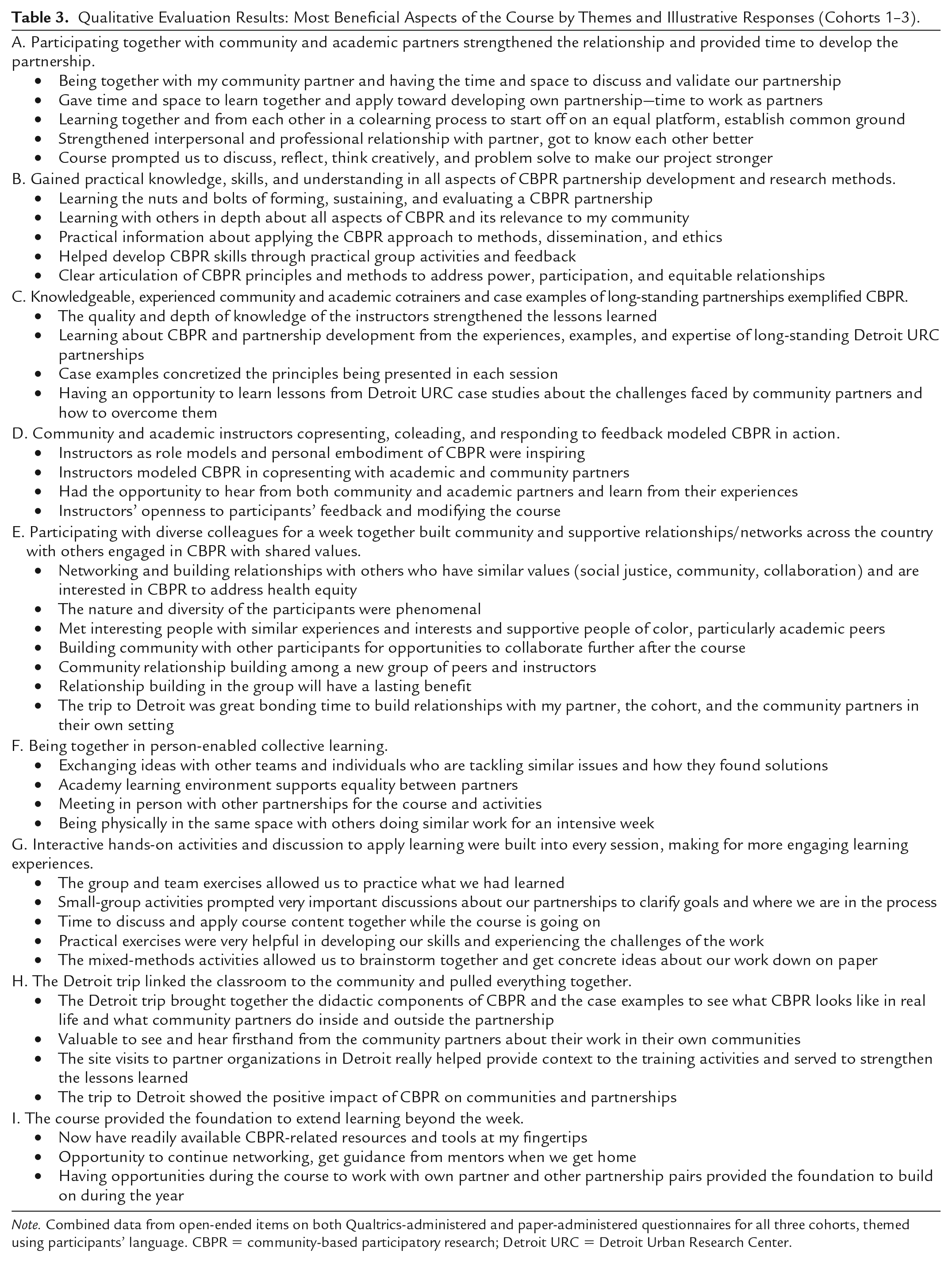
Note. Combined data from open-ended items on both Qualtrics-administered and paper-administered questionnaires for all three cohorts, themed using participants’ language. CBPR = community-based participatory research; Detroit URC = Detroit Urban Research Center.
As presented in Table 3, the evaluation results show that the participants frequently mentioned relational aspects of learning that were integrated into the course structure and pedagogy as the most beneficial aspects of the course. Four themes that centered relationships as a beneficial dimension of learning in the course are participating as partners, learning from community and academic co-instructors, building networks among others with shared values, and being together in person.
Another set of themes cited the in-depth, practical knowledge of CBPR that was gained from the real-world expertise, case examples, and visit to Detroit to see what CBPR looks like in practice. Finally, a central finding was that participants highly valued the interactive, hands-on activities and discussion to apply learning that were built into every session of the course.
Evaluation Findings by Experiential Action Learning Model and Pedagogical Strategies
To synthesize results in relationship to pedagogy, Table 4 presents the connection between the experiential action learning model, pedagogical strategies used in the course, and corresponding qualitative evaluation findings. From left to right, the first column lists each of the seven principles of our model (presented above), including five principles of experiential action learning (Cunningham, 1998; Johnson & Johnson, 2017; Kolb, 2015) and two principles of community-engaged pedagogy that align with CBPR (Israel et al., 2019; Pau & Mutalik, 2017; Rubin et al., 2012). In the middle column, several course activities are listed that exemplify how each principle of our model was applied through pedagogical strategies. In the right-hand column, we list qualitative findings from course evaluations that correspond to the specific principle of the model and pedagogical strategies used. The findings presented are the qualitative themes identified in Table 3, lettered accordingly.
Experiential Action Learning Principles, Pedagogical Strategies, and Qualitative Evaluation Findings.

Note. Findings are from open-ended questions on course evaluation questionnaires administered electronically and in person. See Table 3. CBPR = community-based participatory research.
For example, in the first row of Table 4, Principle 1, “Active involvement in real experiences requiring solutions,” is applied through the pedagogical strategy “Own-team sessions to develop partnership, plan evaluation.” One example of this is an activity in the Day 5 session on using in-depth interviews within a mixed methods design for evaluating CBPR partnerships. Participants work in small groups to identify the purpose, conceptual framework, and audience for evaluating their own partnership, and then they develop sample evaluation questions for conducting in-depth interviews. Results are shared among the large group, who ask questions and provide feedback. From the findings presented in Table 3, corresponding outcomes of this activity can be found within the themes as follows: A. strengthening relationships and developing their own partnership, B. gaining skills in evaluating partnerships, and G. interactive activities to apply learning, shared within and across groups. In addition, the activity enhanced knowledge and skills in how to use a CBPR approach to develop and conduct in-depth interviews, and understanding of a conceptual framework for evaluating CBPR partnerships, corresponding to B. Thus, Table 4 depicts how the principles of our experiential action learning model, applied through pedagogical strategies, contributed to specific outcomes as described by the participants themselves (e.g., “Participating together with community and academic partners strengthened the relationship and provided time to develop the partnership.”).
Participant Assessment of the Least Beneficial Aspects and Recommendations for Change
Responses to questions asking “what was the least beneficial” and “recommendations for change” fell into four major categories, summarized here as recommendations (not presented in table form). There was some variation by cohort, as instructors modified the course in each subsequent year in formative response to evaluation feedback. First, participants recommended that more time be provided for hands-on activities to apply learning, including more time to interact with other participants and to work within teams on their own partnerships. Second, participants recommended that more opportunities be provided to hear from Detroit community members and to interact with community-based organizations outside the classroom. A third recommendation involved tailoring the research methods content to match the different learning needs of community and academic participants. Last, participants suggested that sessions be broken up by including more breaks and physical movement activities.
In addition, many responses to the “least beneficial/recommendations for change” question were that everything was beneficial. The responses included the following: “Nothing—everything was valuable”; “Great job, incredible amount of information, and adapting to participant needs”; “I found the course extremely helpful and engaging”; “Everything exceeded my expectations!!”; “Nothing—this was by far the best use of time/experience I’ve had in the 8 years of working at my current agency”; and “Everything was well thought out.”
Discussion
This article sought to describe the course content and our collaborative, experiential action learning model as it informed the course design; present results from participant evaluation of course effectiveness, learning, and partnership development; and examine the ways in which the learning model and pedagogical strategies contributed to course outcomes that are central to successful CBPR.
The quantitative and qualitative results presented here found that, overall, the participants considered the course instruction to be effective and they came away with high levels of CBPR competence. In response to open-ended questions, the participants described multiple ways in which the course process and content contributed to their learning and to the development of relationships within and across teams. Table 4 suggests that adhering to an experiential learning model and using multiple instructional strategies can contribute to outcomes that cut across active learning principles and activities. It further shows that different aspects of the pedagogy reinforce the importance of attending to all learning principles to enhance capacity in CBPR.
Using both quantitative and qualitative methods and a formative evaluation approach enabled us to strengthen the course both during the week and for subsequent cohorts. For example, we learned from the quantitative results that some aspects of instructional effectiveness and competence were rated lower than was anticipated in Cohort 1. To better understand why, the instructors examined participant responses to open-ended questions about what was the most and least beneficial and recommendations for improvement (qualitative results). Accordingly, we added a relationship-building activity on the first day, integrated more active learning activities throughout, and modified course materials in response. As described in the results section, aspects of instructional effectiveness and competence that had the lowest ratings in the first year received higher ratings in the second cohort and remained high in the third cohort.
There are a number of lessons learned from the pedagogical approach used in this intensive course, illustrated here by participant comments.
Engaging community and academic partners in pairs as both participants and instructors distinguished the CBPR Partnership Academy course from many other trainings. The hands-on, collaborative weeklong experience facilitated intensive colearning within and between diverse partner teams and provided formal and informal opportunities to develop relationships with one another and with instructors.
One of the most valuable things I learned is about relationships. For CBPR to be successful, you’ve got to take the time to build the relationships, and from that, everything else will come.
The course not only addressed the important process and relationship-building components of applying a CBPR approach but also strongly emphasized rigorous methodology, such as the use of mixed methods and alternative research designs within the context of CBPR.
In the type of research I’ve done in the past, the community piece has usually come in at the level of recruitment or disseminating research findings. But through this course, I really learned how to engage the community from the beginning and how to craft research questions together and design the study together, from start to finish.
Affirming what we sought to examine in this article, the underlying conceptual framework and pedagogical strategies of experiential action learning guided by CBPR principles were identified by the participants as critical to the effectiveness of the course. Over the span of one week, community and academic partners developed a shared base of knowledge on how to carry out research using a CBPR approach to address issues of importance to their own communities.
It brought us together in shared understandings of CBPR and allowed us to have necessary conversations about our work together. I feel aligned now, and equipped with the same body of knowledge and resources that can inform our work.
Working collaboratively, the participants applied these concepts and processes to their own work, developing skills and plans to advance their partnership. They noted that the intensive experience allowed them to get to know one another, problem solve in a supportive environment, and build the trusting, equitable relationships that are central to CBPR.
I think it’s awesome to be able to have two very different perspectives at the table together learning simultaneously—and then being able to, almost immediately, take things in theory and apply them to your conceived project and then bring them to your community.
Creating an equitable and safe learning environment of mutual respect and with a highly diverse group of participants was noted as further contributing to building CBPR capacity. This was particularly cited by academics of color, who established networks among one another beyond their institutions.
Many times when I go to conferences or trainings, I have been the only person of color or one of a few people of color, or the only person who speaks Spanish or is an immigrant. This group, honestly, has been a very diverse group, and I think my experience has only been enriched by not having that burden of being the only person or being excluded or whatever.
Having diverse and highly experienced instructors who embodied the principles and processes of CBPR was also mentioned by many participants as central to the learning. Working together, community and academic instructors demonstrated and modeled the critical importance of mutual respect, addressing inequities, ensuring that community knowledge is central to the research effort, and creating a caring community.
The role models and personal embodiment of CBPR was inspiring. I was deeply impressed by the enthusiasm, compassion, and spirit of excellence with which members of the Detroit URC conducted the week . . . seeing your hospitality and how much you invested in us.
For many participants, this experience reinforced the need for and benefit of using multiple instructional methods, recognizing that participants learn differently. Our findings further demonstrate the strength and value of an experiential learning model grounded in CBPR principles in enhancing the capacity of a diverse group of community-academic partners to establish the foundation for carrying out CBPR in their communities. In the words of one participant, Going through each step of integrating or infusing CBPR approaches to community-based research has helped me reflect on how my organization could have done things better and on how we can use this strong approach to truly make our work more community driven.
Challenges and Limitations
Although this article examined how the experiential action learning model/strategies contributed to course outcomes, the course evaluation was not designed to specifically address that question or to evaluate active learning processes. Thus, our primary reliance on quantitative and qualitative data about the beneficial aspects of the course more broadly was a limitation. The evaluation questionnaire did, however, include two questions more specific to pedagogy: What impact did the course have on the relationship between partners and development of the partnership, and what were the beneficial aspects of the site visit to the community? Findings from those questions were included in the themes in Tables 3 and 4 to help inform the extent to which and the ways in which the action learning model was applied and valued.
We sought to provide multiple experiential learning activities to enhance knowledge, skills, and understanding in all aspects of CBPR, while fostering the development of partnerships and networks. Despite our efforts to integrate methodological content, actual case examples, and active learning, participants were eager for more opportunities to engage directly with the material and apply it to their own partnerships. This was particularly so in the first year. As described in the discussion section, using formative evaluation allowed us to modify the course midweek during the first year and improve the course for subsequent cohorts by enhancing experiential and relationship-building activities.
Addressing the learning needs of both academic and community participants was challenging at times, recognizing the very different backgrounds and experiences each brought to the course. Although the course was not a primer on conducting research, but rather how to apply a CBPR approach, some of the methods sessions were too basic for academics and too advanced for some community partners. Although the program team considered participant recommendations to divide up some sessions accordingly, in order to maintain the collaborative, colearning pedagogical emphasis that underlay the course, we instead modified sessions to integrate more colearning between academic and community members.
Finally, being in a classroom all day for a week can be exhausting. In the second year, we ended each day with individual and pair reflection time. In response to the evaluation feedback, we recommend including more physical movement activities and continuing efforts to diversify active learning experiences.
Conclusion
The weeklong intensive course of the CBPR Partnership Academy engaged academic and community partners jointly in a colearning process to enhance their capacity to use a CBPR approach in their communities. Using an experiential action learning model and pedagogical strategies that integrated CBPR principles, the course actively engaged participants in learning with and from one another. Our findings suggest that an experiential action learning approach with attention to colearning, collaboration among diverse instructors and participants, and an environment that fosters and models equitable and trusting relationships can be effective in building CBPR capacity toward achieving health equity.
Footnotes
Acknowledgements
The authors would like to acknowledge the vital contributions to the work described in this article by all of the partner organizations involved in the Detroit Community–Academic Urban Research Center: Community Health and Social Services Center, Inc., Communities In Schools, Detroit Health Department, Detroit Hispanic Development Corporation, Detroiters Working for Environmental Justice, Eastside Community Network, Friends of Parkside, Henry Ford Health System, Institute for Popu-lation Health, Latino Family Services, Neighborhood Service Organization, and the University of Michigan Schools of Public Health, Social Work, and Nursing. The authors also acknowledge the contributions of all CBPR Partnership Academy instructors and mentors (![]() ). We also thank Graciela Mentz, Michael Muhammed, Lello Guluma, and Jennifer Tang Cole for statistical analysis, and Eliza Wilson-Powers, Katherine Corbit, Brianna Jacobs, Lindsay Terhaar, Samantha Henstell, Lisa Pappas, and Julia Weinert for their invaluable assistance.
). We also thank Graciela Mentz, Michael Muhammed, Lello Guluma, and Jennifer Tang Cole for statistical analysis, and Eliza Wilson-Powers, Katherine Corbit, Brianna Jacobs, Lindsay Terhaar, Samantha Henstell, Lisa Pappas, and Julia Weinert for their invaluable assistance.
Authors’ Note
All authors are affiliated with the Detroit Urban Research Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Michigan Summer Session in Epidemiology hosted the initial course from which this course was adapted and provided funding support. This program is funded by the National Institute of General Medical Sciences of the National Institutes of Health under Award #1R25GM111837. Related materials do not necessarily represent the views of the National Institutes of Health.