
Abstract
In the past decade, the number of undergraduate public health programs has increased exponentially. This growth provides a unique opportunity to explore concepts and issues relevant to understanding the determinants of health at a population level using new pedagogical approaches. One of these issues is stigma toward mental disorders. Stigma is a concept that refers to a feature or characteristic that reduces, devalues, and disempowers a person. Given the prevalence of mental and substance use disorders among college students, undergraduate education is an important setting for attempting to address stigmatizing attitudes both for society at large and for faculty, staff, and students, including those experiencing mental health problems. This article describes an effort to develop an undergraduate course in public mental health that explicitly addresses the ways stigma shapes student understanding of this topic and discusses lessons learned from this experience.
In the past decade, the number of undergraduate public health programs offered at U.S. universities has increased exponentially. This growth provides a unique opportunity to explore concepts and issues relevant to understanding the determinants of health at a population level using new pedagogical approaches. Within the tradition of liberal arts training, which emphasizes critical thinking skills and analysis rather than applied praxis (e.g., data collection and analysis; Robinson et al., 2018), undergraduate programs are ideal settings for addressing complex challenges in public health that have few readily available solutions. One of these challenges is stigma toward mental disorders and related behaviors. This article describes an effort to develop an undergraduate course in public mental health that explicitly addresses the ways stigmatizing attitudes shape student understanding of this topic.
Stigma is a concept that refers to a feature or characteristic that reduces, devalues, and disempowers a person (Pescosolido, 2013); in manifestation, it is related to discrimination, marginalization, and oppression (Phelan et al., 2008). Stigma is correlated with misunderstanding, avoidance, and disengagement from people experiencing mental illness, and leads to a lack of information (and even acceptance of erroneous information and myths) about lives and characteristics of people who have experienced mental illness, the causes of mental health conditions, and the effectiveness of treatments (Link et al., 1997; Phelan et al., 2008). Stigma directly inhibits help-seeking behaviors for mental health conditions, including among college students (Martin, 2010). While mental disorders are not the only objects of stigmatizing attitudes relevant to public health (i.e., sexually transmitted infections—particularly HIV—are prime examples; Pachankis et al., 2018), mental disorders offer the means to explore and model pedagogical approaches that address stigma. Fifty percent of mental disorders onset in adolescence (Kessler et al., 2005), and an estimated one third of college students have experienced a clinically significant mental disorder in the past year (Auerbach et al., 2018). This makes undergraduate education an important setting for attempting to address stigma both in society at large and for students experiencing mental health problems and the university faculty, staff, and fellow students with whom they interact (Roy, 2018).
Current Offerings of Undergraduate Training in Public Mental Health
Mental disorders are among the most common health conditions in the population and are associated with substantial social and economic costs. Depression is the leading cause of disability worldwide (Friedrich, 2017), and when these results were released, the Director General of the World Health Organization commented that “these new figures are a wake-up call for all countries to re-think their approaches to mental health and to treat it with the urgency it deserves” (World Health Organization, 2017). In spite of this need, only about half of undergraduate public health programs in the United States offer any coursework on mental health. In July 2019, we reviewed the course listings of Council on Education for Public Health–accredited schools or programs and cross-checked these against the National Center for Education Statistics database to identify undergraduate majors in “Public Health.” Of the 112 institutions included, 72 offered at least one (and often only one) course on psychiatric and/or substance use disorders (hereafter public mental health) as indicated in the course title or description (Supplemental Table 1). Forty-two institutions, including 34 of those with public mental health coursework, offered classes that addressed stress management/personal wellness and/or peer education regarding mental health. These “wellness” classes were directed at students’ own health behaviors rather than conveying the importance of public mental health as a social issue. (We recognize that course content changes over time, may not be fully captured by course descriptions, and that “wellness” classes may address stigma [particularly self-stigma] as part of their pedagogy; Pescosolido, Perry, & Krendl, 2019). While public health students may take coursework pertaining to mental health outside their major (e.g., psychology, neuroscience, or sociology), those disciplines approach mental health from a different perspective than public health. Moreover, the recent emergence of undergraduate training in public health provides an opportunity for exploring new approaches to teaching about mental health since there is no historical memory or disciplinary tradition about syllabus content, core readings, and so on, as there is with foundational undergraduate courses in psychology and sociology.
Acknowledging the Elephant in the Room: Stigma Attitudes of College Students
The majority of college students today seek health information on the internet or other lay media outlets (Jacobs et al., 2017; Oh & Kim, 2014). Media portrayals of mental health conditions are predominantly negative, as noted by Whitley and Wang (2017): Portrayals of people with mental illness tend to revolve around negative factors such as danger, criminality, and violence and frequently contain stigmatizing language. They rarely contain more positive or hopeful stories of recovery. [ . . . ] This negative media coverage can contribute to a toxic social environment that facilitates the rejection, stigmatization, and marginalization of people with a mental illness. (p. 279)
Consistent with this persistent negative portrayal of mental illness in popular media, public opinion surveys show that the level of stigma toward mental disorders including depression, bipolar disorder, and schizophrenia has remained essentially unchanged and substantially negative over the past two decades, and for some conditions, such as substance use disorders, attitudes have worsened over time (Parcesepe & Cabassa, 2013; Pescosolido, 2013). This is despite widespread public education efforts about the neurological basis of mental disorders and related behaviors by health care and advocacy groups (Pescosolido et al., 2010).
It is helpful to understand the pervasive stigma toward mental disorders within a broader context. In contrast to public perceptions and media portrayals of mental illness, today’s media coverage of cancer, a condition that was historically the object of stigma and discrimination, is more often characterized by positive stories of “survivorship” (Larson et al., 2009). Notwithstanding the well-founded critiques of media portrayals of breast cancer survivorship (Bell, 2014), in the past 40 years there has been a fundamental shift in the language used to talk about people who have a history of cancer (Holland, 2002). Part of this shift occurred because of improvements in treatments, and was reflected in the emergence of psycho-oncology as a legitimate clinical field in the 1970s (Holland, 2002). Indeed, today vignette studies of college students indicate little evidence of stigma toward people with a history of cancer, and even suggest such individuals may be rated more favorably than persons who have not experienced cancer (Tuinman et al., 2018).
The potential corollary to education regarding public mental health is this: Stigmatizing attitudes are malleable, but many current approaches are inadequate to address these beliefs. Mental health literacy campaigns, which sought to reduce stigma by educating the public about the neurobiological basis of mental disorders, have indeed enhanced the awareness of and vocabulary with which society discusses mental disorders (Corrigan et al., 2012). However, this enhanced literacy has had little to no impact on these attitudes (Pescosolido, 2013; Pescosolido et al., 2010; Pescosolido, Manago, & Monahan, 2019). Perceptions of people with mental or substance use disorders as dangerous and/or violent have remained essentially unchanged over from the mid-1990s to the mid-2000s, with a majority of Americans agreeing that individuals with schizophrenia or alcohol dependence are likely to be violent toward others (Pescosolido et al., 2010); more recent data give no indication that stigma attitudes have substantially changed since that time (Parcesepe & Cabassa, 2013; Pescosolido, Manago, & Monahan, 2019). Moreover, stigma toward mental disorders is not restricted to the attitudes of the “general public”: It is also common among health care professionals, including those with expertise in mental health (Henderson et al., 2014; Schulze, 2007). In short, previous studies have suggested that coursework about mental health, in and of itself, is unlikely to have an impact on stigma beliefs of students if the approach to pedagogy is solely informational without directly addressing stigma attitudes and beliefs. Instead, a growing body of empirical evidence supports the central importance of direct contact and/or interaction with persons living with, or otherwise describing their experience of, mental and substance use disorders for effective stigma reduction efforts (Corrigan et al., 2012; Corrigan et al., 2013; Penn & Couture, 2002; Wong et al., 2016). This article sought to translate those lessons-learned from advocacy efforts into the classroom.
Approach to Instructional Design of an Undergraduate Public Mental Health Course
In spring 2019, the University of Michigan graduated its first cohort of undergraduate public health majors. Here, we briefly describe the design of a three-credit undergraduate course PUBHLTH 414: Population Approaches to Mental Health (Instructor: Mezuk; enrollment: 24), which was initially offered in fall 2018 as part of the new public health curriculum. An abbreviated syllabus is provided in the Supplementary Materials. To facilitate the instructional design, we hosted a daylong workshop with University of Michigan faculty from sociology, social work, nursing, and public health during the first week of the fall 2018 semester, and expert consultant Dr. Bruce Link began the workshop by giving a public lecture titled “Stigma and Discrimination Associated With Mental Disorders: What Can We Do About It?” We reviewed and critiqued proposed lesson plans, class activities, and assessments, focusing on the motivating principle of increasing knowledge about mental disorders while simultaneously addressing stigma attitudes.
Based on this developmental work, we identified four foundational topics to address in the course (see syllabus provided in the Supplemental Materials):
Conceptual frameworks for understanding population mental health, including the life course framework and the stress-diathesis model
Measurement of mental disorders, data collection, and related issues for quantifying population mental health
In-depth discussions of several major mental health conditions: schizophrenia, depression/anxiety disorders, substance use and dependence, autism, neurocognitive disorders, and suicide
Mental health services, policy, and law
These topics were discussed (both via the online discussion board and in-class activities) in an iterative, recursive fashion throughout the term (e.g., when discussing the epidemiology of substance use disorders, students also learned about data collection issues relevant to this condition; the class discussion of mental health services and the legal system revisited the unique issues related to obtaining treatment for drug abuse and dependence). All these topics involved exposure to both scientific perspectives (i.e., journal articles written for academic audiences) and stakeholder perspectives (i.e., first-person narrative accounts) directed at public audiences. These stakeholder perspectives included media produced by advocacy groups (i.e., the National Alliance on Mental Illness website); TedTalks (i.e., A Tale of Mental Illness from the Inside by Elyn Saks); podcasts interviews (i.e., The Hilarious World of Depression hosted by John Moe; Death, Sex and Money hosted by Anna Sale); readings from autobiographical graphic novels (i.e., Hyperbole and a Half by Allie Brosh); artistic expressions (i.e., “I’m Not Gonna Miss You” by Glen Campbell; “We Grow Accustomed to the Dark” by Emily Dickenson); and even a videogame (i.e., DepressionQuest by Zoe Quinn). Most scientific readings came from the required textbook Public Mental Health (Eaton & Fallin, 2019). This book was chosen because it provides sufficient depth into the four topics above, but also excellent breadth and opportunities for supplemental text for students interested in reading further.
This decision to pair empirical research with stakeholder narratives was inspired by empirical studies showing that direct exposure to or interaction with persons with mental illness reduces stigma (Corrigan et al., 2012; Penn & Couture, 2002; Penn & Martin, 1998; Wong et al., 2016), with the caveat that much of the research supporting this conjecture relies on either past reports of interactions, relatively short-term intervention programs, or experimental manipulation within the confines of a research study (Corrigan et al., 2012; McGinty et al., 2015; Penn & Couture, 2002). These intervention or experimental studies, while critical to isolating the causal processes underlying efforts to reduce stigma, may not be directly translatable to classroom settings (i.e., the longitudinal nature of the teacher–student relationship and the evaluative [grading] element of courses may limit either the implementation or effectiveness of these efforts). To our knowledge, this approach of pairing scientific articles with first-person accounts is not widely used in instructional design for courses that address mental disorders; however, this approach is recommended by policy advocacy groups to enhance the reach and effectiveness of messaging efforts (McGinty et al., 2018). Beyond the archival stakeholder perspectives described previously, students had direct in-person contact with two stakeholders in the public mental health system: (a) the instructor facilitated a question and answer session with the Executive Director of the Washtenaw County Community Mental Health board during a class session, and (b) the class attended a 2-hour hearing at the Washtenaw County Mental Health Court and met with the presiding judge afterwards. Finally, over the course of the semester, students completed a writing project in which they had to synthesize the evidence about a topic relevant to public mental health, of their choosing, incorporating both academic research and stakeholder perspectives into their project.
Evaluation of Student Stigma Attitudes Toward Mental Disorders Over the Semester
Figure 1 illustrates two “word clouds” that were generated by the class on the first and last day of the semester as part of a lesson plan. They were each created by having students provide anonymous written responses to the simple prompt, “Write down the first 10 words you think of when you hear the term mental disorders,” which were then collected and collated using wordclouds.com. The size of each word is proportional to its frequency. For both images, the word stigma is prominent. The most notable differences between the two images are that there is more diversity of terms in the second image (i.e., the words human and disparities are present in the second cloud but not the first), consistent with an interpretation that students developed a greater vocabulary with which to answer this prompt.
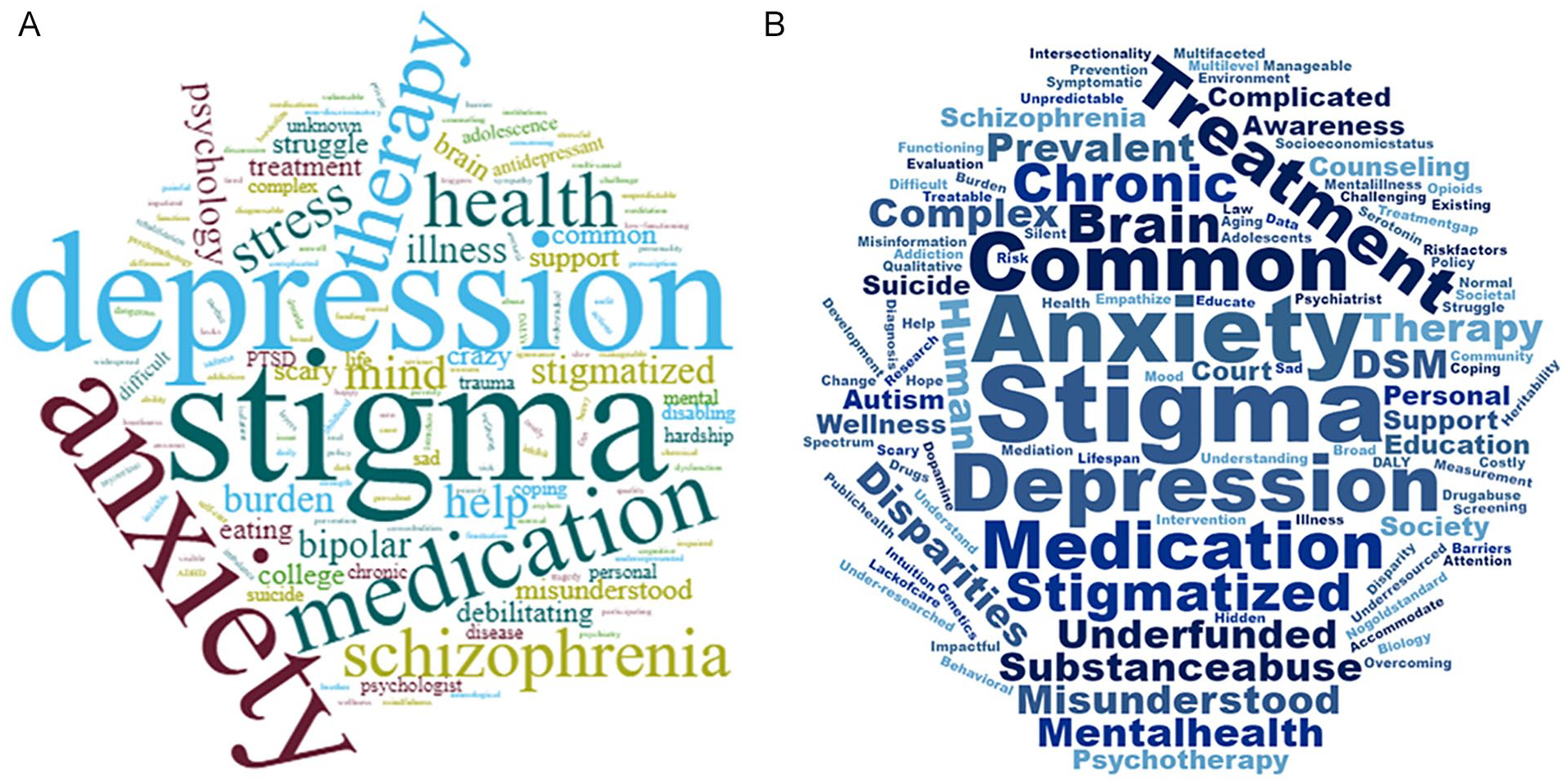
Class word clouds created at the beginning and end of the semester.
Table 1 provides an overview of anonymous course evaluations, including excerpts from the 19 responses to the prompt, “Do you feel your own attitudes/beliefs toward mental & substance use disorders changed as a result of this course? In what way?” Several students cited the importance of the stakeholder perspectives in their response: “. . . the stakeholders have provided a level of empathy that wasn’t there before. There is such a difference between reading about symptoms in a textbook and hearing firsthand how someone’s life has been affected by mental health issues.” We feel it is reasonable to assume that the four students (17% of evaluators; 23 of 24 students completed the course evaluation) who did not respond to the prompt did not feel their attitudes had changed; combining them with the two responses who noted that their attitude had not changed, overall 75% of students (18/24) reported that their attitudes had changed as a result of the course.
Excerpts From Course Evaluations to the Question “Do You Feel Your Own Attitudes/Beliefs Toward Mental & Substance Use Disorders Changed as a Result of This course? In What Way?”

Note. Total class enrollment = 24 students. Number of course evaluations completed = 23 students. Number of students who responded to the open-response question = 19 students.
Beyond the Classroom: The Potential of Undergraduate Education About Stigmatized Health Conditions
Our experience should be understood in context. The course we developed is an upper-level elective at a selective undergraduate institution (acceptance rate is ~25%). We did not have a comparison classroom against which to conduct a formal test of the impact of our instructional design decisions on student stigmatizing attitudes. However, our findings suggest that such an effort is worth pursuing. Our approach to pedagogy was informed by expert consultation with both content experts on stigma and instructional design experts through the Center for Research on Learning and Teaching. We have made the syllabus for this course available so that others can build on our work at their own institutions.
Stigma forestalls creative and critical thinking about the ways in which health care practitioners, educators, researchers, and community stakeholders can address mental health needs in the population. The Association of American Colleges and Universities (2014) says that “an understanding of public health is a critical component of good citizenship and a prerequisite for taking responsibility for building healthy societies.” Our experience illustrates the potential for undergraduate public health to further this goal through evidence-based pedagogical approaches that explicitly recognize the widespread stigma toward mental disorders and related behaviors and seek to challenge them through (a) experiential learning; (b) elevating stakeholder perspectives through written, audio, and visual narratives; and (c) curriculum that goes beyond describing the symptoms, prevalence, and risk factors of mental disorders to one that helps students envision the lives affected by these conditions.
Implications for the Next Generation of Public Health Training
Undergraduate training in public health does not yet have a historical legacy that characterizes many other disciplines of liberal arts education. This provides a window of experimentation, flexibility, and adaptation not only in the content of coursework but in the pedagogical approaches used to engage students with that content. This flexibility is an important strength of undergraduate education in our field, and while it should be preserved, it can be guided by professional organizations and accrediting bodies such as the American Public Health Association and Council on Education for Public Health through emphasizing the importance of mental health as a central component of public health and the roles of stigma and related constructs (i.e., discrimination) play in shaping population health. There is also a need to develop training materials (e.g., textbooks, syllabi, lesson plans) that instructors can draw on when developing their own courses. Our experience illustrates the potential for creative, thoughtful pedagogy that both informs students on the science of public mental health and engages them with personal lived experiences of mental illness to address stigma toward mental disorders. The lessons from our experience can inform future approaches to teaching about stigmatized conditions and populations in public health education.
Supplemental Material
HPP922871_suppl_mat – Supplemental material for What Elephant? Pedagogical Approaches to Addressing Stigma Toward Mental Disorders in Undergraduate Public Health Education
Supplemental material, HPP922871_suppl_mat for What Elephant? Pedagogical Approaches to Addressing Stigma Toward Mental Disorders in Undergraduate Public Health Education by Briana Mezuk, Belinda Needham, Kevin Joiner, Daphne Watkins, Sarah Stoddard, Sarah Burgard and Bruce Link in Pedagogy in Health Promotion
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Gilbert Whitaker Fund for the Improvement of Teaching from the University of Michigan Center for Research on Learning and Teaching.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.