
Abstract
Black, Indigenous, and other people of color (BIPOC) are underrepresented in the public health workforce. Strengthening the public health pipeline through graduate institutions of public health is a necessary anti-racist approach to address health disparities. Programs that provide effective mentoring are one strategy for evidence-based anti-oppressive instructional practice, proven to help racial and ethnic students historically targeted by oppression in propelling career trajectories, professional development, and overall institutional experience in graduate school. The Mentoring of Students and Igniting Community (MOSAIC) program was founded in 2019 as a comprehensive and anti-racist faculty-to-student mentorship initiative for BIPOC and first-generation students. Through a scoping review of mentorship programs at schools of public health and an iterative feedback process that included faculty, students, and staff, the MOSAIC model was created. Built on the tenets of successful mentorship approaches, MOSAIC focuses on increasing equity and educational justice with a focus on professional development and academic success through faculty-to-student mentorship. The growth of MOSAIC has demonstrated it fills a critical gap for students of color and first-generation students in a school of public health. MOSAIC intends to act as a programmatic model for replication at other schools of public health to provide necessary support and mentorship for BIPOC students.
Introduction
Black, Indigenous, and other people of color (BIPOC) are underrepresented in schools of public health and the public health workforce (Brown et al., 2021; Liburd et al., 2021; Mitchell & Lassiter, 2006). Numerous public health studies have documented the impact of threats to belonging—the feeling of being unseen, unwelcome, or unrepresented—not only on academic achievement but also on health itself (Gopalan & Brady, 2020; Paradies et al., 2015). A diverse public health workforce, trained at inclusive institutions of public health, is critical in ensuring anti-racism approaches are amplified and health disparities are effectively addressed (Aqil et al., 2021; Derreth et al., 2021; Goodman et al., 2020; Liburd et al., 2021; Merino, 2019).
The creation of a people-centered, inclusive educational climate—one in which not only content but also instructional activities are grounded in evidence-based anti-oppressive practice, is essential to the realization of inclusive institutions (Aqil et al., 2021; Hagopian et al., 2018; Hussain & Jones, 2021; Perez et al., 2021). Anti-oppression is the strategy of mitigating the social harms of those historically oppressed in society and rebalancing power within communities, institutions, and systems. Related, anti-racism is the process of identifying and opposing racism at structural and systemic levels to actively change the policies, behaviors, and beliefs that perpetuate racism (Kendi, 2019). Programs that provide effective mentoring are one strategy for evidence-based anti-oppressive and anti-racist instructional practice, proven to help racial and ethnic students historically targeted by oppression in propelling career trajectories, professional development, and overall institutional experience in graduate school (Brown et al., 2021; Davidson & Foster-Johnson, 2001; Reddick & Young, 2012; Thomas et al., 2007).
Mentorship, particularly for students historically targeted by oppression, is only made a priority for undergraduate students (Thomas et al., 2007). Yet mentorship is identified as a critical component in the successful personal and professional growth of students from underserved groups, including BIPOC and first-generation students, pursuing graduate education (Brown et al., 2021; Brunsma et al., 2017; Davidson & Foster-Johnson, 2001; Johnson & Gandhi, 2015; Thomas et al., 2007). Students disadvantaged by race, income, education, gender, and other stigmatized social markers express greater difficulty in reaching out to potential mentors and developing a relationship with them (Brown et al., 2021; Brown-Nagin, 2016). With mentorship that includes strong institutional support and guidance throughout education, BIPOC students are better equipped to enter the public health field, leading to higher representation from these communities (Brown et al., 2021).
Mentorship can occur at multiple levels from peer-to-peer to alumni-to-student and faculty-to-student (Clark et al., 2012; Dollinger et al., 2019; Reddick & Young, 2012). Peer-to-peer mentorship programs are commonplace for BIPOC students (Clark et al., 2012). However, comprehensive faculty-to-student mentorship programs at the graduate level for BIPOC and first-generation students are uncommon (Brown et al., 2021; Thomas et al., 2007). The lack of mentorship programs at schools and programs of public health can be attributed to the historic lack of diversity in both student and faculty populations and historic and structural racism that laid the foundation for modern institutions.
Given the gap in faculty-to-graduate student mentorship in schools of public health, Mentoring of Students and Igniting Community (MOSAIC), was conceptualized as an anti-racist senior to junior (faculty-to-student) mentorship program for BIPOC and first-generation students. MOSAIC is founded on the notion that anti-racist pedagogy is an organizing effort for institutional and social change that goes well beyond teaching in the classroom (Kishimoto, 2018). MOSAIC utilizes an anti-racist framework by recognizing the system of racism (including in institutions of higher public health education), by encouraging the confrontation of faculty and student implicit bias and racist ideas, by recognizing that hate has spillover effects across and between communities, including different racial groups, and explicitly supporting anti-racist policy and practice through student and faculty ideas, programs, and policies elevated to the school-wide and university level.
MOSAIC leverages the Mentoring Competency Framework (MCF), a framework originally designed for successful research mentoring, that includes effective communication, aligning expectations, assessing understanding, fostering independence, addressing diversity, and promoting professional development (Fleming et al., 2013). For example, effective communication includes active listening, providing constructive feedback, developing a trusting relationship, accommodating communication styles, pursuing strategies to improve communication, and coordinating with other mentors (Fleming et al., 2013). This descriptive case study of MOSAIC provides an overview of the program and the lessons learned from 2 years of program implementation in order to provide a model, set of best practices, and programmatic outline for implementation at additional schools of public health.
Methods
Formative Research and Scoping Review of Mentorship Programs
As a first step, a scoping review of mentorship programs aimed at BIPOC and first-generation students in the top 20 schools of public health (based on the U.S. News and World Report 2021 rankings) and related medical schools and general health fields (at institutions of or affiliated with the top 20 schools of public health) was conducted. The scoping review was conducted using targeted web-based searches on mentorship programs offered at various public health institutions through institutional websites, organizational webpages, and broader Google-based searches. Schools of public health were identified using the U.S. News & World Report rankings, and some related schools of medicine and general health programs (not exhaustive) were included. Key search terms included “mentorship programs, mentoring, mentors, BIPOC, first-generation, graduate students, senior to junior, faculty mentorship, alumni mentorship, and professional development.” The information derived from public institutional websites included the name of the program, the affiliated institution, location, mission, and type of mentorship offered, which were then compiled into a database.
Program and Curriculum Development
The MOSAIC curriculum was based on the Mentoring Competency Framework (Fleming et al., 2013) and created based on the needs and interests of BIPOC and first-generation MPH students. The programmatic tenets were ultimately developed by faculty and eligible students who self-identify as BIPOC and/or first-generation. The pilot group of students attended a working meeting with the two lead faculty members to discuss how they envisioned the structure and content of the MOSAIC curriculum. Students split into small groups and responded to prompts regarding gaps in their academic, mentorship, and professional development experiences and ways to fill those gaps. Students identified that formal and informal mentoring from faculty and alumni was a gap in their educational experiences at a university that was not originally designed for students of color—indeed, explicitly excluded them. Students expressed a desire for a group mentorship and community-building approach with faculty.
Integral to the mission of MOSAIC is considering student input throughout the entirety of the program planning process. In an initial MOSAIC meeting at the start of each semester, students are asked to provide topics they would like to discuss at meetings as well as the type of events they would like to attend during the academic school year that would be beneficial to their educational and professional long-term goals. This is done in a workshop setting where students and core faculty are placed into small groups, given prompts, and discuss different programing (informal and formal) that would be most beneficial to them. The curriculum for the year is then tailored to this input to address student needs.
Attendance records from each meeting were reviewed to assess the expansion of MOSAIC over the course of 2 years. Subscription to the program listserv also provided a record of the total number of student participants each year. At the end of the year, graduating students are entered into the alumni database to remain in touch and engage them in future volunteer and panel opportunities.
The lessons learned from the first 2 years of program implementation were used to create the MOSAIC logic model for faculty-to-student mentorship for students of color and first-generation students at schools of public health. Program documents such as grant applications, meeting notes, and input from faculty and eligible students affiliated with MOSAIC ultimately informed the programmatic and evaluation model. Per study procedures approved by the university Institutional Review Board (AAT5993), informed consent was not required.
Results
Table 1 shows mentorship programs that were identified across the top 20 schools of public health, and some related schools of medicine and general health programs. Several of the leading public health schools have mentorship programs; however, the majority of programs do not offer faculty-to-student mentoring, and many are focused on alumni-to-student mentorship. Only four schools of public health (Brown School of Public Health, Harvard Chan School of Public Health, George Washington University, and Washington University in St. Louis Institute for Public Health) have faculty-to-student mentorship programs, but these are not geared toward current public health graduate students. To our knowledge, no other programs at the top 20 schools of public health provide comprehensive mentorship that includes faculty, staff, alumni, and students for students of color and first-generation graduate students. Other related health sciences programs, including schools of medicine and general health programs, seem to have more offerings (N = 6) in terms of programming for faculty-to-student mentorship. None of the identified programs at the leading schools of public health have clear curricular and mentorship models for students of color and first-generation graduate public health students that could be replicated at other institutions.
Mentorship Programs at the Top 20 Schools of Public Health and some Schools of Medicine and General Health Programs a .
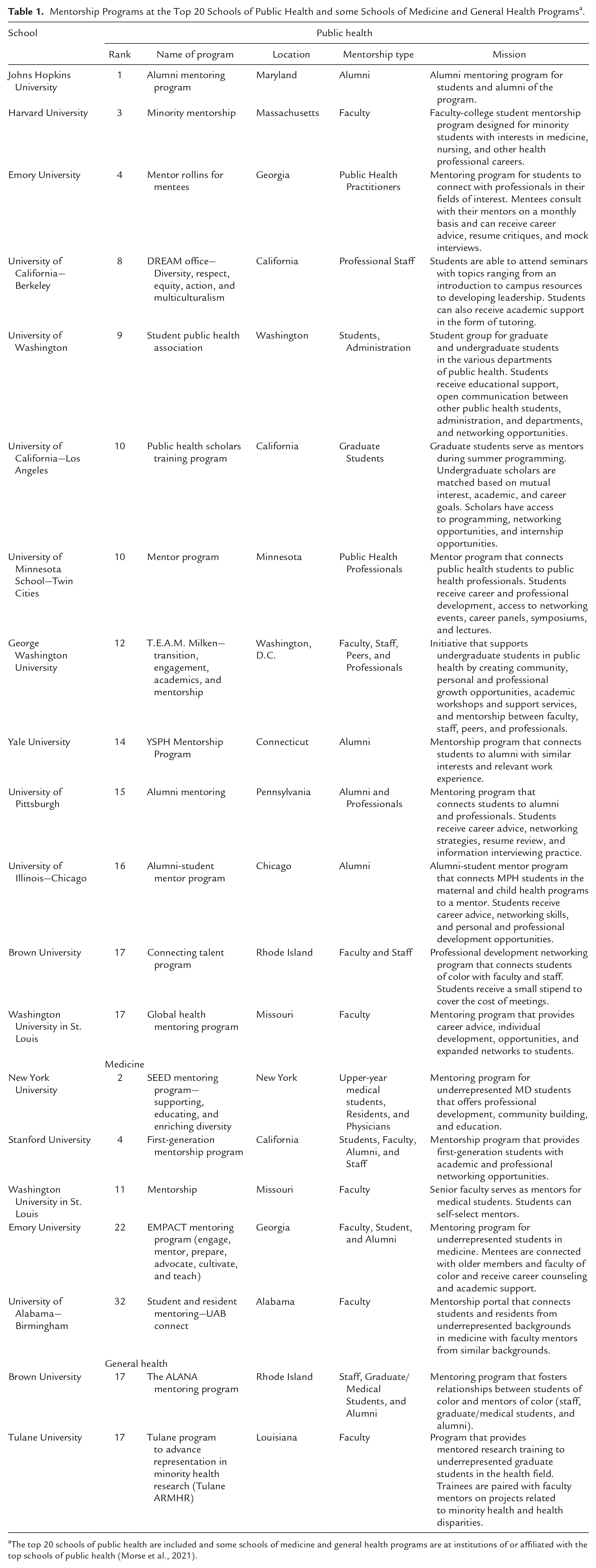
The top 20 schools of public health are included and some schools of medicine and general health programs are at institutions of or affiliated with the top schools of public health (Morse et al., 2021).
Mentoring of Students and Igniting Community
Figure 1 shows the five domains of the Mentoring of Students and Igniting Community (MOSAIC) model. Guided by the scoping review results and the Mentoring Competency Framework (Fleming et al., 2013), these domains include professional development, faculty mentorship, navigating institutions, incident management, and guest speakers or connections to faculty and alumni. MOSAIC strives to mobilize and engage students, faculty, staff, and alumni amongst historically oppressed and privileged voices at multiple levels. Specifically, the MOSAIC model centers on facilitating senior-to-junior mentorship and guidance, informal engagement of students with faculty, and the creation of community.
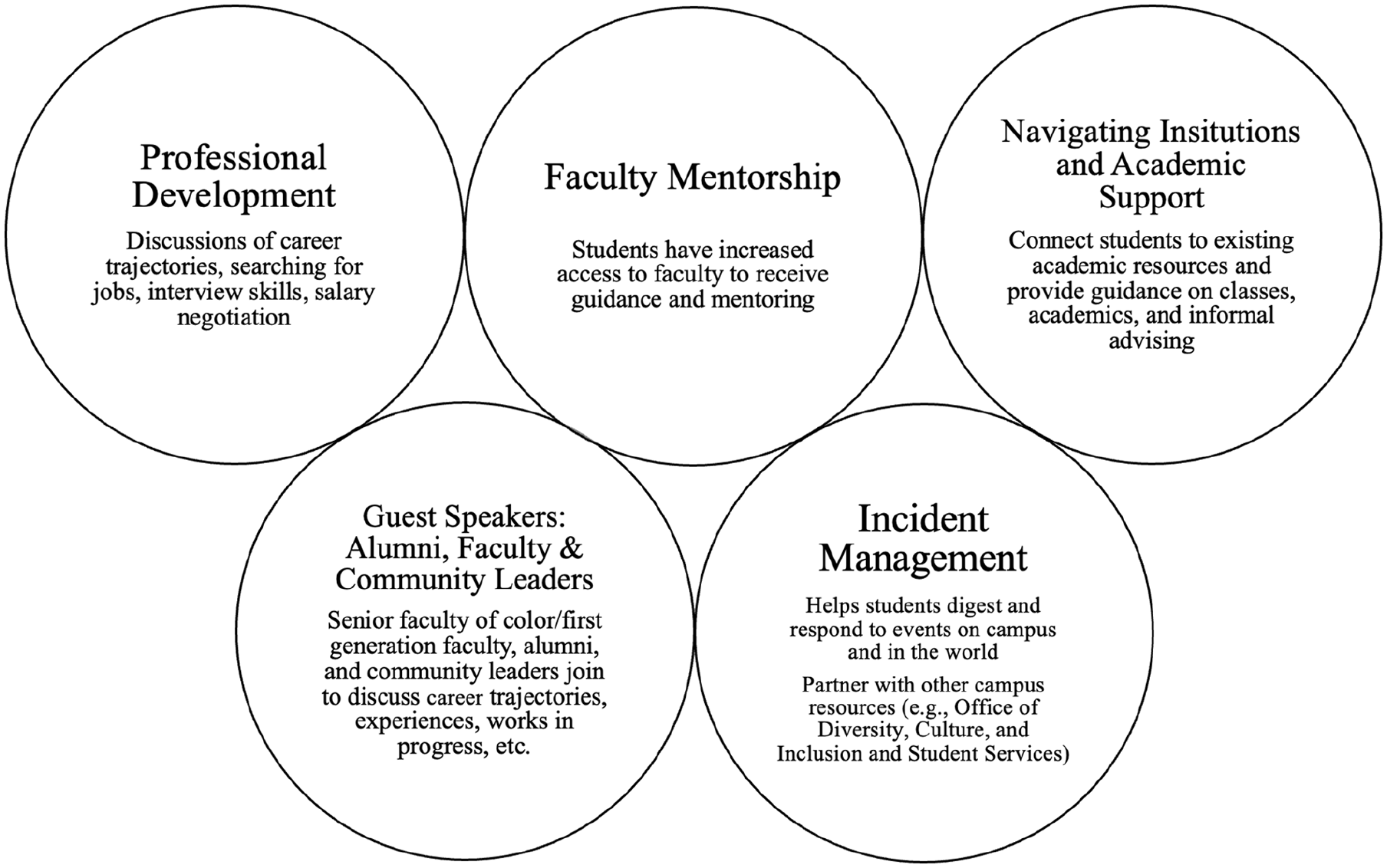
Five domains of MOSAIC.
MOSAIC was designed to help students of color and first-generation students navigate the world of academia and public health more successfully while creating community between faculty, staff, alumni, and students. The five domains of MOSAIC were refined and further adapted in consultation with the students during the founding year of MOSAIC (2019) so as to be responsive to student input and the specific gaps in the mentorship they identified. MOSAIC tackles issues of racial justice and equity through each domain. Specifically, MOSAIC centers on an anti-racist approach to graduate student mentorship by recognizing a system of racism, confronting implicit bias, understanding how hate has spillover effects across and between communities, engaging in an intersectional approach, involving diverse student and community feedback in the process at all times, and supporting anti-racist policy and practice through actionable programmatic and policy efforts. By simply creating a mentorship space for first-generation and students of color, MOSAIC creates community between faculty, staff, alumni, and students, addresses curricular gaps related to racial equity, and establishes connections to existing institutional resources.
Table 2 shows the growth MOSAIC has undergone over the first 2 years of its existence—a testament to the gap it is filling for BIPOC and first-generation students. The origins of MOSAIC were in one department. Yet, even in its founding year (2019), students from all other school of public health departments were welcome to join. It is foundational to MOSAIC that no student is turned away from mentorship. Thus, the MOSAIC membership in the first year included two departments in the school of public health and a total of 26 students. In the second year, the membership increased fourfold (N = 96 students), demonstrating that there is a need among BIPOC and first-generation students for programs like MOSAIC. As of 2021, the racial and ethnic distribution of MOSAIC students included 13% Hispanic, 39% Asian, 33% Black, 8% Middle Eastern, and 8% of two or more races.
MOSAIC Composition Over Time.

As MOSAIC has expanded and as MOSAIC students have graduated and become alumni, the alumni involvement has also increased from the 2019 academic year to the 2021 academic year. Alumni involvement is critical as it increases the amount of mentorship students receive and connects them beyond their two short years in graduate school. Further, because of the ongoing growth of MOSAIC, staff who identify as BIPOC or first-generation have also become increasingly involved in events. Two faculty members of color comprise the core faculty of MOSAIC, four to six faculty of color are involved annually to support mentorship efforts, and any faculty who want to be involved in the program are welcome to join and provide additional student support.
MOSAIC Logic Model
Figure 2 displays the logic model for the MOSAIC curricular and mentorship approach. The logic model demonstrates the culmination of lessons learned for the MOSAIC approach over the first 2 years. MOSAIC aims to have senior to junior mentorship lead to improved student engagement with the community, improved academic performance, higher retention of students, a greater sense of professional development, and improved navigation of academic and professional outlets. At the core, MOSAIC requires faculty mentors to oversee the group and plan activities, BIPOC graduate students, and bi-monthly meetings to cover the different activities (Figure 2, Activities and Outputs columns). These activities will at times require alumni engagement and institutional support, including financial resources (outside speakers, meeting needs, and student support for printing, summer internships, and conference attendance). Although the main tenets of the curriculum are set (see Figure 1), the specific programmatic efforts each semester are meant to have flexibility in order to be responsive to evolving student needs and institutional changes. The BIPOC and first-generation faculty and students that are engaged in MOSAIC make up the major inputs to the program, along with resources including financial and institutional support.
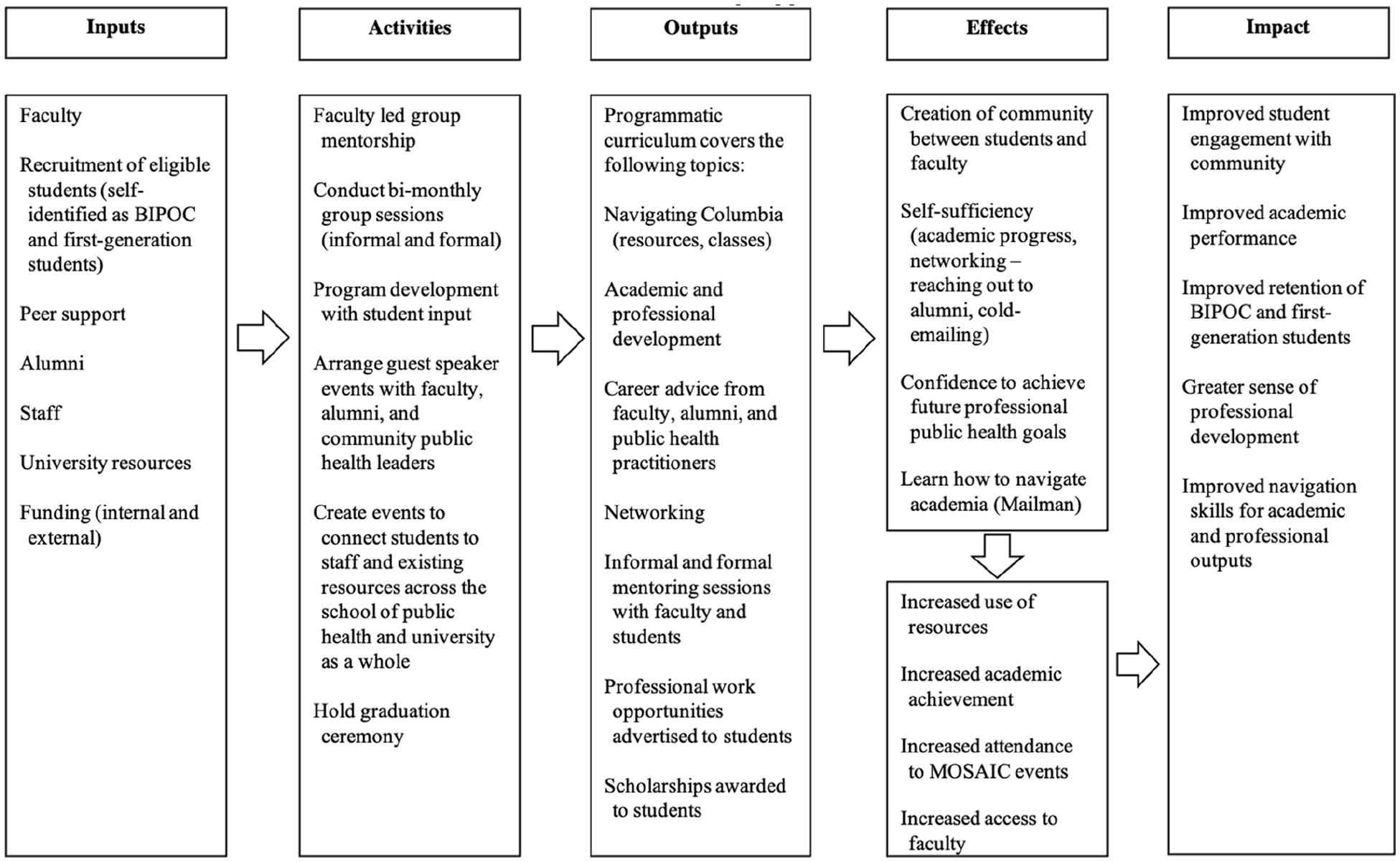
Logic model for MOSAIC programmatic and mentorship approach.
The lessons learned from the first 2 years of program implementation were used to create the MOSAIC logic model, as well as input received from students and faculty. The activities and outputs are made up of the formal and informal components of the MOSAIC curriculum. MOSAIC was intended to exclusively operate through formal mentorship pathways; however, student input indicated that informal time with faculty was integral to their sense of community. Thus, MOSAIC meets twice monthly, and MOSAIC students are polled at the beginning of each semester to establish a meeting time (lunchtime, end of the day, etc.). One meeting is designed to be a formal programmatic event across the five domains and one meeting is designed to be an informal check-in, reflections on current events, and an open forum to discuss any ongoing or emergent issues. Formal programmatic events are moderated by the two lead faculty members who are joined by guest speakers (alumni, staff from career services, public health community leaders, etc.) who engage in a dialogue with the students. Guest speakers discuss career trajectories, navigating the transition from graduate school to work, and creating space in public health for BIPOC and first-generation public health practitioners. Discussion with guest speakers emphasizes the experiences of BIPOC students, faculty, staff, and alumni to provide potential tools for academic and professional success based on the experiences of others in navigating an academic public health institution and careers in public health. Each semester, MOSAIC meets roughly seven times as a group, consisting of two faculty members and a cohort of students from all departments. Students can arrange one-on-one meetings with faculty members as desired. It is critical to note that MOSAIC partners with existing resources at the university (student affairs, student wellness, writing center, etc.) and helps organize individualized events for MOSAIC students with those university resources and connections. This is vital as students are sometimes not as comfortable reaching out for support or do not know where to look for existing opportunities.
The desired effects of MOSAIC are intended to be multifold and include impacts on individual and community level wellbeing and success. The intention is to create an increased sense of community between students and faculty and peer-to-peer along with increased self-sufficiency and ability to navigate academia and professional public health contexts confidently. Process data to date, as evident by the growth of MOSAIC over 2 years, is encouraging for the programmatic appeal of MOSAIC amongst BIPOC graduate students. For long term impact, there is an ongoing impact evaluation to measure outcomes including improved student engagement with the community, improved academic performance, improved retention of BIPOC and first-generation public health graduate students, greater professional development, and improved navigation skills for academic and professional public health settings.
Lessons for the Field
This case study of a comprehensive anti-racism graduate mentorship program, Mentoring of Students and Igniting Community, shows one possibility of how schools of public health can engage in anti-oppressive mentorship practices to potentially meet the needs of BIPOC and first-generation students and institutional anti-racism goals. Experience with MOSAIC to date and past research has demonstrated how valuable mentorship can be for the creation of community among first-generation and students of color in institutions, including schools of public health, that have historically valued and centered whiteness (Brunsma et al., 2017; Clark et al., 2012). MOSAIC strives to establish sustainable mentorship and take actionable steps toward the achievement of an anti-racist community at a school of public health. For many institutions of higher education, there is a long way to go to dismantle systems of racism; however, MOSAIC offers a small step forward in anti-racist programming and support for BIPOC and first-generation students.
While there are several faculty of color-led mentorship programs across other disciplines, MOSAIC is the first faculty-to-graduate student group mentorship program of its kind at a school of public health, the only graduate-level mentorship program taking a multidimensional approach, and unique in its comprehensive, anti-racist mentorship mission. The unique aspects of MOSAIC that set it apart include: (1) Faculty and student involvement—MOSAIC is not a peer-to-peer mentorship program, but instead involves faculty and students in a group mentorship model; (2) Involvement of alumni—MOSAIC programming includes alumni involvement to create networking opportunities and expose current students to a range of career paths; (3) Flexible curricular scaffolding—MOSAIC’s approach to curriculum provides the major domains but allows for flexibility to meet the changing student needs; and (4) Anti-racist framework—MOSAIC takes an anti-racist approach by responding to the disparities among students caused by racism, racial, and socioeconomic inequities and acting as a resource for BIPOC and first-generation students to help them navigate graduate school.
Previous research has demonstrated the critical importance that mentorship can play for students of color in higher education (Brown et al., 2021; Brunsma et al., 2017; Davidson & Foster-Johnson, 2001; Reddick & Young, 2012; Thomas et al., 2007). The results of the scoping review of faculty-to-student mentorship programs at schools of public health, indicate that there is a clear gap in graduate mentorship at the schools of public health. MOSAIC recognizes that faculty mentorship is often unavailable yet especially beneficial to students from underserved groups pursuing graduate education (Brown et al., 2021; Brunsma et al., 2017; Thomas et al., 2007) and aims to fill this gap through its programmatic model. Diverse faculty mentors can serve as role models and provide social and intellectual capital to students that are underrepresented in graduate schools and in the field of public health.
MOSAIC was partially birthed out of necessity because of undue mentorship burdens for faculty of color. That is, the group mentorship approach allowed faculty to simultaneously better utilize their time and meet student needs (Lechuga, 2011). However, the growth of MOSAIC is likely rooted in its ability to create community between faculty and students, reaffirm BIPOC and first-generation students belonging in a school of public health, and challenge systems of racism that are pervasive in institutions of higher education. Several of the involved faculty are racism and health researchers, and those faculty recognize that being anti-racist is a continuous challenge to and recognition of one’s own racist beliefs.
MOSAIC is situated at a large research university where diversity has increased over time with 53% of 2021 to 2022 students identifying as racial and ethnic minorities (8% Black, 28% Asian, 12% Latinx, and 5% two or more races) and 14% identifying as first-generation. Given the large subset of the school’s population with the potential to be served by MOSAIC programming, MOSAIC has been supported at the school and university level, which helps solidify its role in the institutional anti-racism efforts. MOSAIC continues to overcome challenges, as is the nature of any anti-racist effort, including engaging students from across the school including all departments, acquiring financial resources for programmatic efforts and student support, and recruitment of additional faculty mentors. Despite these challenges, MOSAIC is a potential programmatic model for increasing equity and educational justice with the possibility of improving student learning and professional development outcomes through mentorship (to be determined by an ongoing impact evaluation). For any size program or school of public health, the primary resource requirement of MOSAIC is a minimum of two willing faculty members to meet with a group of BIPOC students twice monthly to offer programing through the key tenets of the model and as preferred by their students.
The MOSAIC model outlines institutional practices and processes for first-generation and students of color that could change the institutional structure by emphasizing anti-racism for potential replication at other schools of public health. Investing in mentorship in the institutional spaces that train a diverse public health workforce could strengthen the pipeline and potentially have significant impacts on the health outcomes of marginalized populations (Blenner et al., 2021; Derreth et al., 2021; Liburd et al., 2021; Perez et al., 2021). As the national conversation about racial equity continues, it is critical that innovative, institutional programs like MOSAIC are supported and replicated to help institutions of higher public health education meet their anti-racism goals (Merino, 2019) and to help the public health workforce better succeed in tackling health disparities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The research was supported by the Columbia Mailman School of Public Health Dean’s Office and the Columbia University Office of the Provost. The content is solely the responsibility of the authors and does not necessarily represent the official views of Columbia University.