
Abstract
Cardiac rehabilitation programs (CRPs) improve outcomes and reduce mortality among patients with cardiovascular disease; however, referral rates remain suboptimal. This cross-sectional study investigated factors influencing referral decisions to CRPs among healthcare providers in Riyadh City. A self-administered online questionnaire was distributed to physicians, nurses, and allied healthcare professionals working in hospitals and primary healthcare centers. A total of 166 participants completed the survey. Overall, approximately 40% of participants reported referring patients to CRPs, with nurses demonstrating the highest referral rate. Referral likelihood was significantly associated with years of professional experience, with the highest referral rates observed among participants with 5–10 years of experience (p = 0.04). The most commonly reported barriers to referral included limited availability of cardiac rehabilitation centers, patient refusal, limited patient mobility, and shortages of trained or experienced staff. Patient comorbidities and lack of awareness regarding CRP benefits were also identified as important barriers. Regarding CRP delivery models, most participants preferred hospital-based programs, although many also considered home-based cardiac rehabilitation to be a practical and convenient alternative. These findings highlight the need for strategies aimed at improving CRP accessibility and strengthening referral practices in Saudi Arabia. Expanding rehabilitation services, improving healthcare provider training and awareness, and integrating structured referral pathways into healthcare systems may help increase referral rates and patient participation in CRPs. Further studies using larger and more representative samples are recommended to better evaluate referral practices and identify effective interventions for improving CRP utilization.
Keywords
Introduction
Cardiovascular diseases (CVDs) remain a significant global health challenge, contributing substantially to morbidity and mortality worldwide. 1 CVDs encompass a group of disorders affecting the heart and blood vessels, with risk factors including smoking, obesity, an unbalanced lifestyle, genetic predispositions, and infections.1,2 Among the most common forms of CVDs are coronary artery disease, heart failure (HF), angina, myocardial infarction, hypertension, and stroke. 3 Notably, CVDs are the leading cause of death globally, responsible for 17.8 million deaths annually, one-third of which are premature, occurring in individuals under the age of 70. 1
The burden of CVDs is particularly pronounced in the Arab Gulf region, with Saudi Arabia reporting CVDs as the cause of 24.34% of total annual deaths. 4 This elevated prevalence imposes substantial healthcare costs, predominantly driven by hospitalization expenses. In Saudi Arabia, the direct medical cost for heart failure patients is approximately $9,563 per patient each year, with hospitalization accounting for the largest share of this expense. 5 Similarly, a study conducted at King Fahad Cardiac Centre (KFCC), King Saud University Medical City, reported an average annual cost of approximately $8,137 per heart failure patient, with hospital admissions and readmissions representing the major cost drivers. 6
To mitigate the impact of CVDs, the American Heart Association and American College of Cardiology recommend cardiac rehabilitation (CR) as a Class I indication for secondary prevention in patients with cardiovascular conditions. 7 Reinforcing this, Kwan and Balady (2012) emphasized CR as a primary strategy for patients recovering from myocardial infarction, acute coronary syndrome, heart failure, and post-coronary artery bypass surgery. Participation in CR has been shown to reduce mortality by 13% to 24% and rehospitalizations by 31%. 8 Moreover, a meta-analysis of 63 randomized clinical trials involving 14,486 patients from 1974 to 2014 demonstrated that CR significantly reduces cardiovascular-related mortality, hospital admissions within one year, and healthcare costs, while also improving patients’ health-related quality of life. 9
Despite the established benefits of CR, Saudi Arabia currently lacks a national policy for cardiac rehabilitation programs.10,11 Referral decisions are typically left to the discretion of individual physicians, resulting in inconsistent referral rates and unequal access to care. This lack of standardization highlights the need for research to understand the factors influencing healthcare providers’ referral decisions and to advocate for clear national guidelines. Addressing these barriers is essential for improving patient outcomes and expanding access to CR services in Saudi Arabia.
Methods
This was a cross-sectional study aimed at exploring the factors that influence healthcare providers’ decisions to refer patients to CRPs in Riyadh City. In this study, “referral” was defined as any action by a healthcare provider including physicians, nurses, or other professionals that directs a patient to participate in a CRP. This includes formal referrals, such as completing referral forms or scheduling appointments, as well as informal recommendations or guidance to encourage patient participation.
Data were collected using a self-administered online questionnaire distributed through social media platforms. Convenience and snowball sampling were used, where participants were asked to invite other eligible healthcare professionals. This approach was used to reach a wider group of healthcare providers across Riyadh. The study included general practitioners, cardiologist, nurses, physiotherapists, and other healthcare professionals working in hospitals or primary healthcare centers in Riyadh who were actively involved in treating patients with cardiovascular disease. Healthcare providers working in universities or those not directly involved in managing patients with cardiovascular disease were excluded.
The survey instrument used in this study was adapted from a previously developed and validated questionnaire by Aldhahir et al, 12 designed to assess healthcare providers’ perceptions of and barriers to referral to cardiopulmonary rehabilitation programs. The questionnaire comprised three main sections. The first section collected demographic and professional characteristics, including profession, years of experience, clinical responsibilities, and prior referral of patients to cardiac rehabilitation programs. The second section assessed healthcare providers’ perceptions and attitudes toward cardiac rehabilitation using Likert-scale statements rated on a five-point scale ranging from strongly disagree (1) to strongly agree (5). The third section evaluated patient-related and process-related factors influencing referral and non-referral decisions, which were rated using an influence scale (no influence, some influence, strong influence). For analysis, responses were summarized using frequencies, percentages, and mean scores for individual items. No composite or total scores were calculated; each item was analyzed independently. Example items included statements such as “Limited availability of cardiac rehabilitation centers influences my referral decision” and “Patient mobility limitations encourage referral to cardiac rehabilitation.” The original questionnaire demonstrated acceptable content validity and internal consistency, as reported by Aldhahir et al, and has been applied in similar healthcare provider populations in Saudi Arabia.
Ethical approval for this study was obtained from the Institutional Review Board of the Ministry of Health (MOH), Saudi Arabia (IRB Log No. 23-83 M). The study was approved under an expedited review category. Participation was voluntary, and informed consent was obtained electronically from all participants prior to completing the survey. No personally identifiable information was collected. All data were anonymized and stored securely on password-protected devices accessible only to the research team, in accordance with MOH regulations and ethical guidelines.
Following approval, the online survey was distributed via social media platforms from November 2023 to February 2024. All participants were provided with a clear explanation of the study’s purpose, and informed consent was obtained through a preamble statement and a Consent Statement before starting the survey. Participants were also informed of their right to withdraw from the study at any point without any consequences.
The collected data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 25.0. Descriptive statistics, including means, standard deviations, frequencies, and percentages, were used to summarize the demographic characteristics of the participants, their referral patterns, and their perspectives on cardiac rehabilitation programs. Associations between categorical variables were assessed using chi-square tests or Fisher’s exact tests, as appropriate. A significance level of p < 0.05 was used.
Results
Participant Characteristics
Demographic Characteristics of Participants
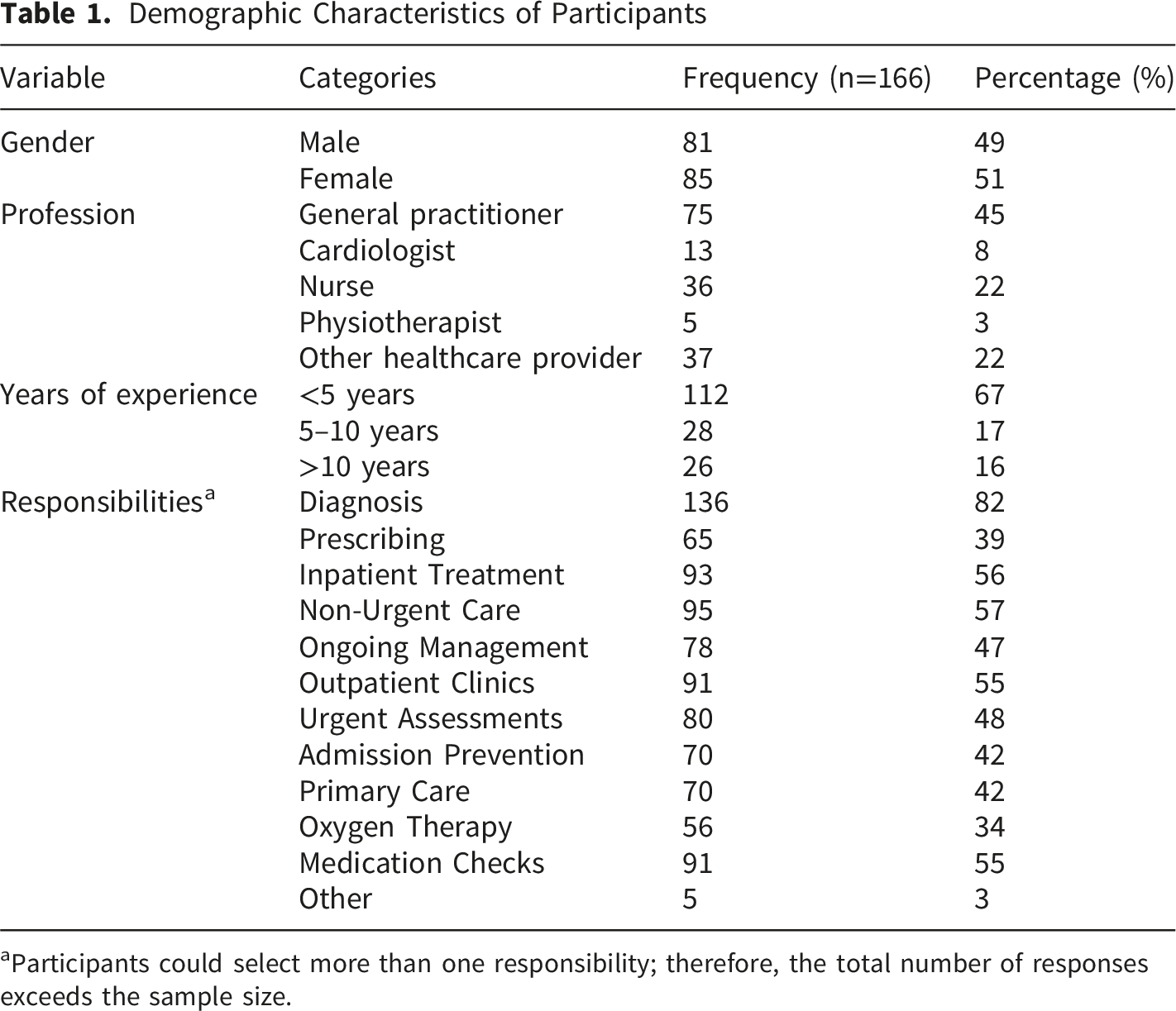
aParticipants could select more than one responsibility; therefore, the total number of responses exceeds the sample size.
Referral Decisions by Demographics
Referral According to Demographic Variables
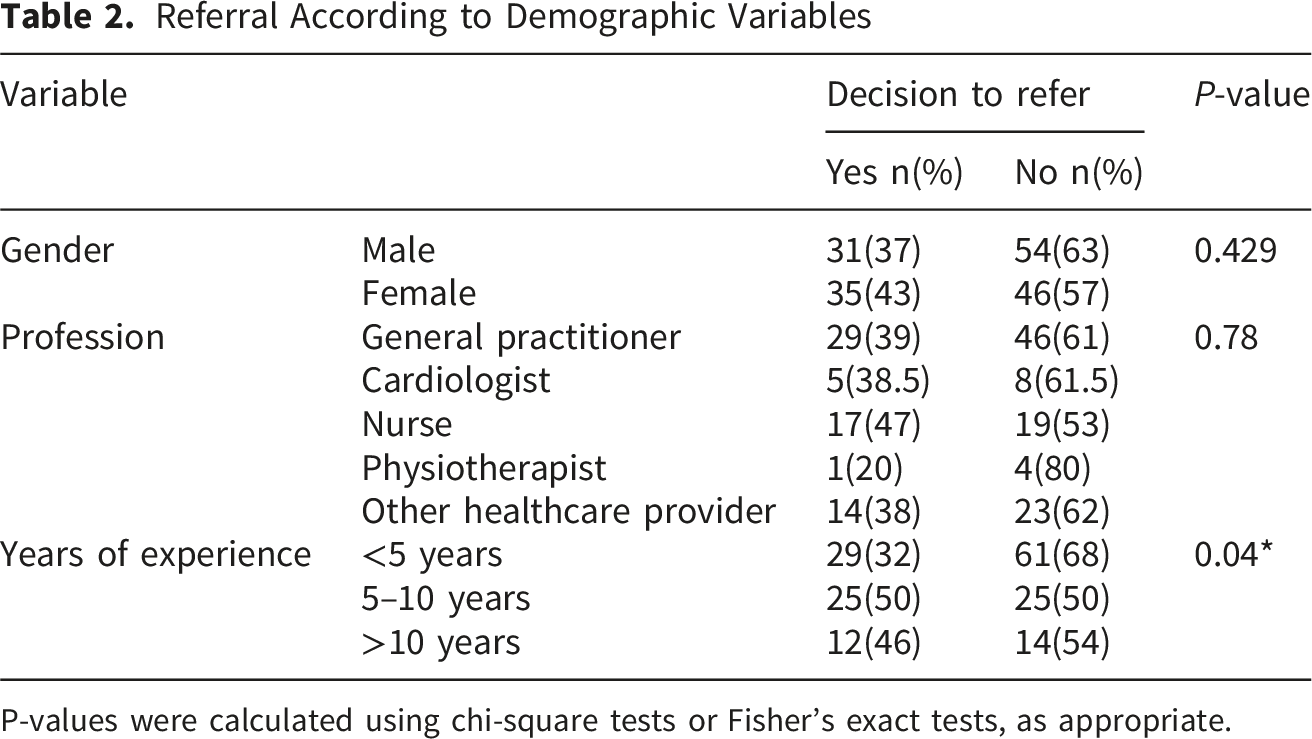
P-values were calculated using chi-square tests or Fisher’s exact tests, as appropriate.
Preferred Delivery Methods for CRPs
Regarding preferred methods of delivering CRPs, 66% of participants favored hospital-based programs. Home-based delivery was considered more convenient by 58%, while 37% preferred online formats and 38% supported follow-up through phone calls.
Negative Factors Influencing Non-referral Decisions
Factors Influencing the Decision Not to Refer Patients to a Cardiac Rehabilitation Program

Responses were rated on a 3-point Likert scale: 0 = no influence, 1 = moderate barrier, and 2 = major barrier. Higher mean scores indicate greater perceived influence on non-referral decisions.
Positive Factors Influencing Referral Decisions
Factors Influencing Referral Decisions (Positive) by Professional Role and Years of Experience

Values represent mean scores based on a 3-point Likert scale (0 = No Influence, 1 = Some Influence, 2 = Strong Influence). One-way ANOVA tests were used to compare mean scores across professional groups and years of experience.
P-values < 0.05 are considered statistically significant and marked with an asterisk (*).
Discussion
This study evaluated factors influencing healthcare providers’ referral decisions to CRPs in Riyadh City. Years of professional experience showed a significant association with referral practices, with healthcare providers who had 5–10 years of experience demonstrating the highest referral rates. In contrast, lower referral rates were observed among healthcare providers with less than five years of experience. Similar findings were reported by Aldhahir et al, who observed higher referral rates among physicians with greater clinical experience in the management of heart failure patients. 12
More than half of healthcare providers reported that they do not routinely refer eligible patients to cardiac rehabilitation programs. Cardiologist also reported notable non-referral rates, although interpretation should be cautious because of the small number of cardiologist in the sample. Previous studies have similarly identified nurses as central contributors to cardiac rehabilitation delivery and patient education, consistent with European recommendations recognizing nurses as key healthcare providers within CRPs.13,14 A Swedish study further demonstrated the contribution of nurses to patient education, medication adjustment, blood pressure control, and lipid management within cardiac rehabilitation settings. 15 Previous literature has also shown that nurse-led counseling interventions can improve psychological outcomes, including anxiety and depression, among cardiac patients.15,16
Limited availability of rehabilitation centers was identified as a major barrier by 91% of participants, including those reporting either “some” or “strong” influence (Table 3), while shortages of trained staff were also reported as an important obstacle to CRP referral and implementation. These findings are consistent with previous studies in Saudi Arabia, where inadequate training, limited awareness among healthcare providers, lack of trained personnel, and inadequate infrastructure were identified as major barriers to establishing outpatient cardiac rehabilitation services. 17 Similar barriers have also been reported from the patient perspective, with Aldhahir et al finding that 59.9% of patients identified limited availability of CRPs as a major barrier to participation. 18 Although most participants in the present study supported hospital-based CRPs, home-based rehabilitation was also frequently preferred because of its greater convenience and accessibility.
Previous studies in Saudi Arabia have identified several patient-related barriers to cardiac rehabilitation participation, including limited referral from healthcare providers, logistical difficulties, and long travel distances to rehabilitation centers. 19 Studies evaluating the Arabic version of the Cardiac Rehabilitation Barriers Scale also identified time constraints, comorbidities, and health system limitations as major barriers to participation. 20 In addition, studies examining physical activity among Saudi adults reported low motivation, limited facilities, long working hours, and cultural barriers as common obstacles to regular physical activity, particularly among women. 21
Several patient-related factors were identified as barriers to referral to cardiac rehabilitation programs. Approximately 80% of participants reported patient refusal as a major obstacle to referral. Limited mobility due to breathlessness or physical deconditioning was identified by 75% of participants as a barrier to referral, while 84% considered mobility limitations an important indication for CRP referral when present. In addition, 73% of participants identified patient comorbidities as a barrier to referral. Similar findings have been reported in previous studies demonstrating lower cardiac rehabilitation enrollment among heart failure patients with multiple comorbidities. 12
Regarding the mode of cardiac rehabilitation delivery, 66% of participants preferred hospital-based CRPs, whereas 58% favored home-based CRPs. Similar findings were reported by Nkonde-Price et al, who demonstrated comparable clinical outcomes between home-based and center-based cardiac rehabilitation programs, with lower hospital readmission rates observed in home-based models. 22 Comparable benefits between the two delivery approaches have also been reported in previous review articles involving cardiac populations.22,23 Home-based CRPs are often associated with greater convenience and lower financial burden for patients, which may improve adherence and participation.22,23 Nevertheless, hospital-based CRPs remain important for elderly patients and individuals requiring closer clinical supervision during physical activity.24,25
Access to cardiac rehabilitation programs remains limited for many patients in Riyadh, Saudi Arabia. This reflects trends reported in several countries worldwide, regardless of economic status. However, within the framework of Saudi Arabia’s Vision 2030, our findings emphasize the opportunity to address this gap through expanding CRP availability and strengthening workforce training while aligning with ongoing national healthcare transformation initiatives. Expanding CRP accessibility and improving healthcare provider training may enhance patient awareness, acceptance, and participation in rehabilitation services, ultimately contributing to reductions in cardiovascular morbidity and mortality.
Improving cardiac rehabilitation referral practices in Saudi Arabia requires expanding the availability of rehabilitation centers, strengthening healthcare provider training, and increasing awareness of cardiac rehabilitation services among healthcare professionals. Integrating structured referral pathways into hospital systems may further improve referral rates and patient participation in cardiac rehabilitation programs.
This study has several limitations. The use of convenience and snowball sampling may have introduced selection bias and limited the generalizability of the findings. Data collection through a self-administered online questionnaire may also have resulted in social desirability bias, with possible overreporting of positive referral practices and favorable attitudes toward cardiac rehabilitation. Distribution of the survey through social media platforms may have underrepresented healthcare providers with lower social media engagement. In addition, the relatively small number of cardiologist included in the sample limited profession-specific comparisons. Finally, the reliance on self-reported responses rather than objective referral records may not fully represent actual clinical practice.
Conclusion
Referral rates to cardiac rehabilitation programs in Riyadh remain suboptimal despite the established benefits of CRPs in improving cardiovascular outcomes. Limited availability of rehabilitation centers, shortages of trained staff, and patient-related barriers including limited mobility, comorbidities, and lack of awareness were identified as major factors influencing referral practices. Expanding CRP availability, strengthening healthcare provider training, and integrating structured referral pathways into routine clinical practice may improve referral rates and patient participation. Home-based cardiac rehabilitation programs may also improve accessibility for selected patient groups. Further multicenter studies with larger and more representative samples are needed to evaluate referral practices and assess interventions aimed at improving CR utilization in Saudi Arabia.
Footnotes
Acknowledgement
The authors would like to thank all healthcare providers who participated in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.