
Abstract
Non-Steroidal Anti-inflammatory Drugs (NSAIDs) are widely used for pain and inflammation relief and are available over the counter in India. Despite common adverse drug events (ADEs), formal reporting and patient awareness remain low. This cross-sectional study in a primary care facility in Haridwar, Uttarakhand, assessed 201 patients aged 18 to 75 years using NSAIDs for at least three months for chronic pain. A structured de novo questionnaire (Cronbach’s α 0.85) evaluated their knowledge, attitude, practices (KAP), risk factors, and self-reported ADEs. Results showed 47% lacked NSAID knowledge, 66% held negative attitudes, and 55% did not comply with prescriptions. Around 63% were at risk of complications, and 67% experienced ADEs. Most (68%) wanted to stop NSAIDs, while 58% favored alternative therapies for pain management. The study revealed limited awareness of NSAID risks in this region, with many experiencing ADEs and at risk of complications. The findings highlight the urgent need for educational programs and revisiting current NSAID usage guidelines to prevent ADEs and promote safer alternatives in India.
Plain Language Summary
This study explored how people use Non-Steroidal Anti-inflammatory Drugs (NSAIDs) which are common pain killers, for long-term pain conditions, their knowledge, along with attitude towards these medicines. NSAIDs are common medicines used to reduce pain and inflammation, but many people experience side effects with their use. We surveyed 201 adults in Haridwar, India, who had been using NSAIDs for at least three months. The results showed that 66.66% of users reported side effects, such as stomach problems, heart issues, skin related or other complications. Despite this, 63.20% continued using NSAIDs even though they were at risk of serious health issues.
We found that 68% of participants wanted to stop using NSAIDs due to concerns about side effects and effectiveness over time. Meanwhile, 58% preferred using alternative therapies like traditional or complementary medicines for managing chronic pain. Our study also revealed differences based on socioeconomic status: people in higher-income groups had better knowledge and practices related to NSAID use, while those in lower-income groups needed more education to use these medicines safely.
This research highlights a need for better education programs about safe NSAID use, especially in lower socioeconomic communities. It also suggests that health providers like doctors and nursing staff should discuss alternative pain management options with patients. Improving awareness and understanding of NSAID risks can help reduce harmful side effects amongst patients. If certain new policies are made regarding NSAIDs prescription, it will further reduce hospital visits by patients due to complaints of side effects with these drugs, thereby saving money and providing better health care.
1. Introduction
Non-steroidal anti-inflammatory drugs (NSAIDs) are commonly used across the world for musculoskeletal pain relief, fever and inflammation. The World Health Organization (WHO) has cataloged NSAIDs on the list of essential medicines. 1 In India, NSAIDs are frequently prescribed as analgesics and antipyretics and are also available over the counter. This makes it difficult to conduct surveillance activities pertaining to NSAIDs. Healthcare infrastructure is often inadequate, especially in remote areas, leading many individuals to self-medicate, regardless of possible adverse events and serious drug interactions at times. 2
Extensive pharmaco-epidemiological studies highlight multiple health hazards associated with prolonged NSAIDs use, especially gastrointestinal and cardiovascular complications, damaging vital organs. 1 Common side effects include dyspepsia, peptic ulcer and upper gastrointestinal bleeding. NSAIDs also affect the central nervous system causing dizziness, headache, and sleep disturbances. Other documented adverse effects involve pulmonary issues such as bronchospasm, and cardiovascular risks including elevated blood pressure, heart failure, and thrombosis. 3 Hepatic and dermatologic adverse events, ranging from elevated liver enzymes to severe reactions like Stevens-Johnson syndrome, have also been reported. 4 A nationwide cohort study from Korea found non-selective NSAIDs were more linked to development of Anemia, celecoxib being associated with cerebrovascular accidents and all the NSAIDs except meloxicam caused renal toxicity. 5 These adverse events have an impact on the health and financial situation of the patient, adding to their stress. 6 In clinical practice, this limits drug use and dose escalation, resulting in poor compliance and a barrier to drug use by the patient. NSAIDs pose increased risks for patients with chronic conditions such as hypertension, diabetes, coronary artery disease, and chronic kidney disease. 7 Patients with chronic pain sometimes fail to perceive precise adverse reactions. 8 Especially in the geriatric population, NSAIDs enhance the risk of side effects and drug interactions owing to polypharmacy.9,10 Polypharmacy is associated with risk of falls, poorer health outcomes and increased cost that burdens the patient further. 11
Considering these facts, increased mortality and morbidity due to NSAIDs has been implicated in the elderly with multi-disease focused prescriptions.12,13 Surveys from other countries indicate a growing dissatisfaction towards prescribed analgesics in patients with chronic pain, calling for newer treatment approaches to address the unmet need for safer analgesia.14,15 Half of the patients were reported to have tried alternative medicine, experienced adverse effects and taken over-the-counter medicine in addition to prescribed NSAIDs, showing their changing preferences for care.15-17 However, no study has so far described the attitude of patients and the risks of NSAIDs usage in the Indian population.
More specifically, previous studies have focused on NSAID-induced adverse drug events (ADE) in orthopedic inpatients
18
with detailed gastrointestinal, renal, and cardiovascular complications.
19
However, limited research has explored patient Knowledge, Attitude, and Practices (KAP) regarding NSAIDs consumption. KAP theory is a widely used cognitive framework that emphasizes the role of positive beliefs and comprehensive knowledge in imparting better health care practices.
20
Patient KAP is an important aspect that leads to the identification patterns, and misconceptions that negatively impact safe use. Risk is another factor that influences the intake of NSAIDs, as polypharmacy is common in older patients, highlighting the need for thorough medical history taking by physicians to avoid unnecessary prescriptions and educating them about the risks of self-medication.
21
This study aims to fill these gaps by assessing KAP, risk factors and ADE among NSAID users with chronic pain conditions in North India (Figure 1). Its findings will provide essential insights to inform targeted educational programs and policy interventions for safer NSAID use in this population. Conceptual framework of the study.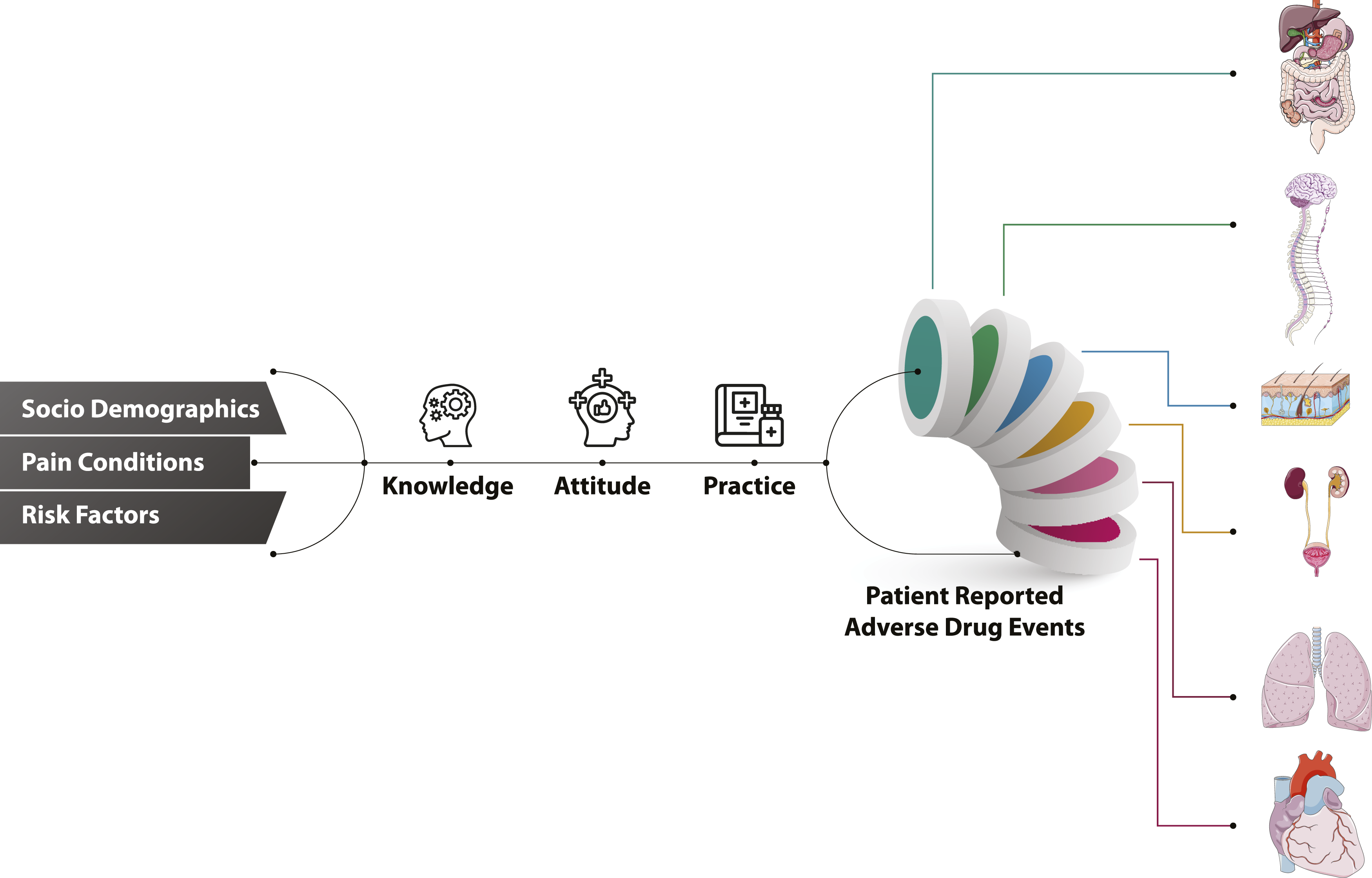
2. Materials and Methods
2.1 Sample and Settings
This was a cross-sectional observational study of all individuals visiting a hospital in Haridwar, Uttarakhand, India, between December 2022 and February 2023. Pre-trained researcher(s) approached OPD patients in order to evaluate their eligibility for the study. All of those patients who met the inclusion criteria were duly informed about the study; and were enrolled in the study after taking informed consent from each participant. Eligibility criteria included age 18-75 years, and on regular or intermittent use of NSAIDs for ≥ 3 months, for pain-related complaints. Ethical approval for the study was obtained from the Institutional Ethics Committee, and the STROBE statement was followed for the entire study. A structured case record form was used for data collection. Skilled interviewers collected data after providing comprehensive details to the participants regarding the study, its purpose, and the voluntary nature of participation. Prior to the data collection, written informed consent was obtained from each participant.
Questionnaire and its Administration
A team of physicians, pharmacists, and scientists reviewed the questionnaires to ensure accuracy. Unrelated questions were eliminated or replaced, to align with study objectives. Subsequently, 20 individuals were invited to verify the understanding and compatibility of the questionnaire with the study objectives. A case record form was used to collect data from each participant. The first section of the case record form contained information on the demographic characteristics, medical history and social history of the individual. The second section consisted of questions probing KAP. There were five questions on knowledge, 8 questions of attitude and six on practice. Each question had three possible answers (Figure 2 BCD). Knowledge-related questions focused on the awareness of risk, interaction, disease precipitation, dependence, and the presence of healing properties. The first four attitude-related questions covered pain alleviation, cost-effectiveness, satisfaction, and the desire to continue therapy. The final four questions inquired about receptivity to different treatments, whether allopathic or alternative, and general beliefs in alternative medicine. There were various options for each practice-related question, which were then further divided into categories of good, bad, and not so good practices. The first question asked how long the drug had been used, with options of 3 months to 2 years, 2-10 years, and > 10 years. Other options included 1-3 times per week, 4-7 times per week, and more than 7 times per week to score the frequency of drug use. Prescription modalities were also recorded with options including medical doctors, pharmacists, and self-prescriptions. Dosage was assessed based on whether it was in accordance with the prescription, exceeded the prescription, or whether the patient was uninformed about the dosage. The use of NSAIDs and antacid consumption was also probed, with the response options being yes, no, or uninformed. The last question pertained to the use of drugs before, after, or at any point in relation to meal. For practice-related questions, each of the aforementioned possibilities received ratings ranging from good, bad, and severe respectively. The third section of the questionnaire discussed the adverse effects of the medication on various organ systems, based on the symptoms described by individuals. According to the NICE guidelines, associated risk factors such as anticoagulants, corticosteroids, aspirin, SSRI, comorbidities, and conditions that may enhance NSAID-induced concerns were listed (NICE, 2018). A. Chronic pain conditions for which participants were taking NSAIDs; B. Current Knowledge, C. Attitude, and D. Practices (KAP) followed by participants who were taking NSAIDs for pain relief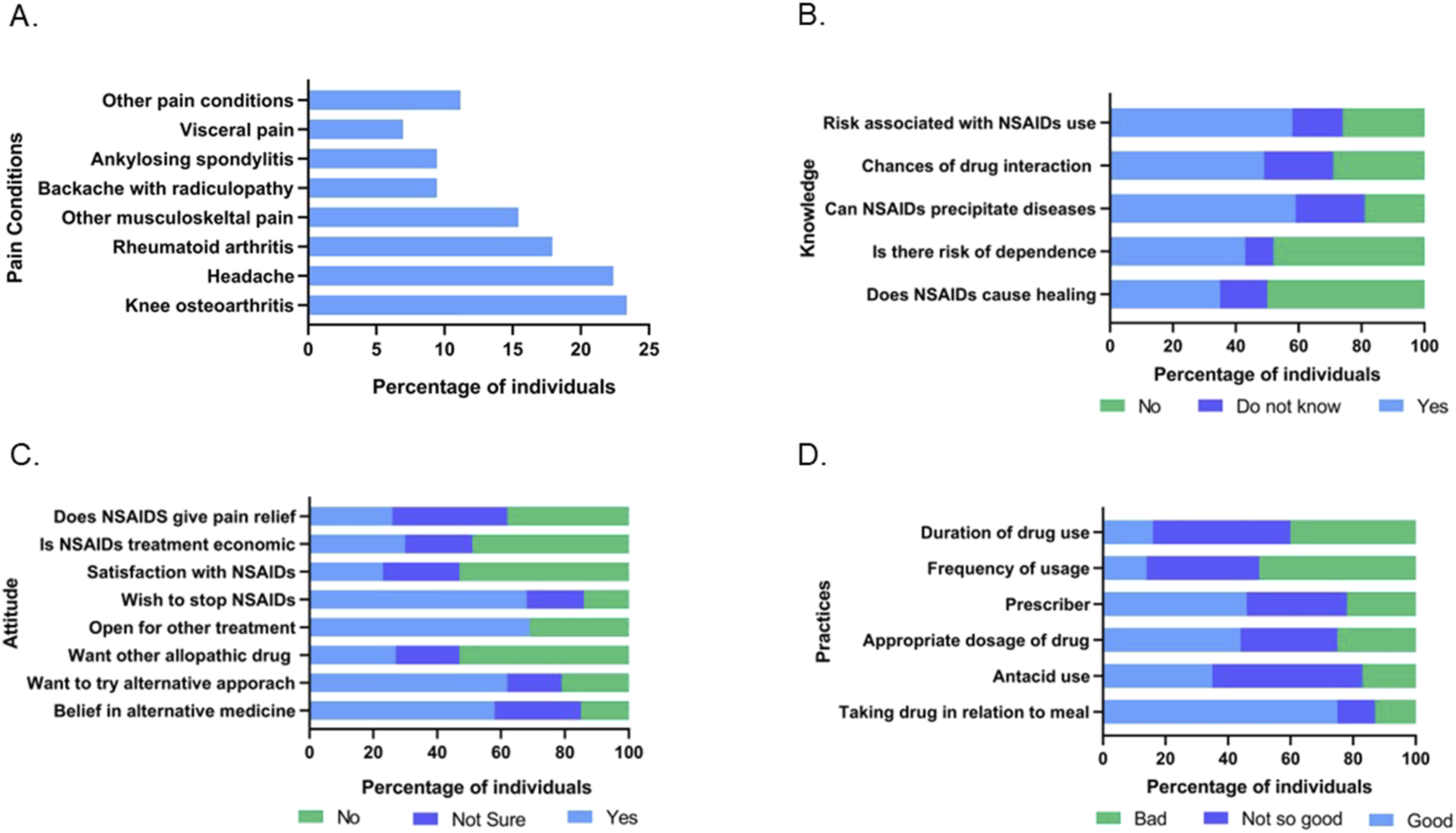
2.2 Statistical Analysis
The analysis was performed using Microsoft Excel and IBM SPSS software (version 26.0). Categorical data were explained in terms of frequencies and percentages. Continuous data was expressed as mean and standard deviation (SD). Pearson’s correlation coefficient was utilized to determine correlations among variables. The minimum required sample size was determined to be 186 using Raosoft (https://www.raosoft.com), with a margin of error of 5%, confidence level of 95%, population size of 3600, and a response distribution of 85% based on prior study. 19
The questionnaire had Cronbach’s α value of 0.85, indicating good reliability. All the answers were marked from 1 to 3, from more desirable to less desirable. Each answer of the section was added to provide a total. The good and bad categories of KAP score were determined based on the median value of the total score. Ethical principles listed in the Declaration of Helsinki and all applicable laws and regulations, including data privacy laws, were strictly followed.
3. Results
A total of 273 individuals with chronic pain were screened at a hospital in Haridwar, India. Among them, 218 participants aged 18-75 years met the inclusion criteria for NSAID use; after excluding 17 incomplete cases, 201 were analyzed.
3.1 Demography
Demographic Details of the Participants, Along With Comorbidities
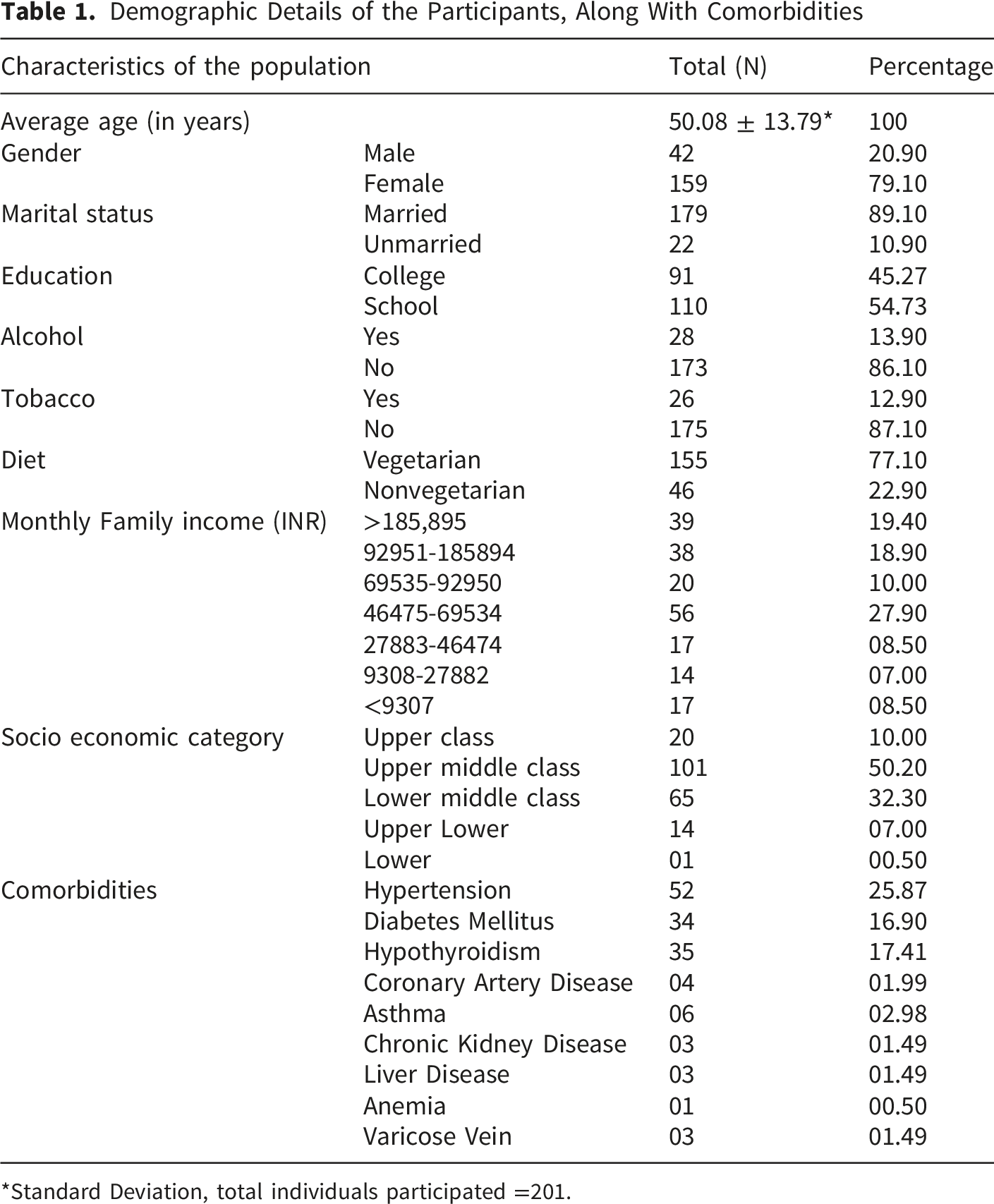
*Standard Deviation, total individuals participated =201.
3.2 Pain Conditions and KAP
NSAIDs were primarily used for knee osteoarthritis, headache, rheumatoid arthritis, and other musculoskeletal pains (Figure 2A). KAP of the individuals is depicted in Figure 2B-D. Knowledge assessment showed 26% perceived no risk from NSAIDs, with 58% aware of associated risks such as drug interactions (49%) and disease precipitation (59%) (Figure 2B). When inquired about dependence and healing properties of NSAIDs, 43% opined that one could become dependent and 35% had an incorrect notion that NSAIDs could heal. Nearly half (47%) lacked adequate knowledge and required education.
There were eight questions related to attitude (Figure 2C); the first four asked about their perception towards NSAIDs and the last four asked if the person wanted to switch to another treatment. There were 38% of individuals with no pain relief. Thirty percent of respondents considered NSAIDs to be economical, and 49% considered it expensive. Satisfaction with NSAIDs was low as 53% showed clear dissatisfaction with NSAIDs. When asked if they wanted to stop current treatment, 68% affirmed yes. Survey responses showed that 69% of participants wanted to try another treatment. It is interesting to note that 53% refused to try another drug for pain relief and only 27% were ready for it, while 20% were uncertain of it. However, when asked if they were ready for an alternative and complimentary medicine, 62% agreed and 21% disagreed. Majority of the respondents (58%) showed firm belief in alternative and complementary medicine, while 15% disagreed. Briefly, three quarters of population (66%) held a negative attitude towards NSAIDs and only 34% showed positive attitude towards NSAIDs.
Figure 2D showed responses to practice-related questions on NSAIDs use. There were 16 % respondents who were taking NSAIDs for less than two years, 44% from two to ten years, and 40% for more than ten years. A pattern of frequent NSAID use was also observed. The frequency of taking the drug in last month of up to <4 times a week accounted for 14%, 4-7 times a week for 36% and > 7 times a week for 50% of the participants. Prescribing trends accounted for 46% by doctors, 32% by pharmacists and 22% of self-referrals. As many as 44% agreed that they were taking appropriate dose, 31% were taking more than prescribed and 25% responded that they were uncertain, implicating a divergence from good practices. In this study, 35% of individuals strictly adhered to prescribed antacids or proton pump inhibitors along with NSAIDs, 48% were noncompliant, and 16% were ignorant. When asked about the intake of NSAIDs related to meal a total of 75% confirmed they took it post prandial, 11% took before meal and 12% took anytime during the day. Briefly, 55% of respondents were following bad practices, while 45% were following good practices regarding the use of NSAIDs.
3.3 Adverse Drug Events
NSAID-related adverse events were noted in a total of 66.66% individuals. In the present study, the gastric system was impacted the most, with 30.85% individuals complaining of it, followed by an impact on nervous and integumentary systems with 8.96% and 7.46% respectively (Figure 3A ). Percentages of individuals with complaints related to renal, respiratory system and cardiac system were 4.98%, 3.48% and 3.48%, respectively. When the adverse effects associated with drug use were evaluated, we found that paracetamol, diclofenac and ibuprofen, showed the maximum adverse events (Figure 3B). Celecoxib and piroxicam showed minimal impact, whereas doloxicam and ketorolac showed no adverse impact among the participants. A total of 43.78% of individuals were taking a combination of paracetamol and other NSAID, which has shown maximum number of Adverse Drug Events (ADE). In addition, there were 46 (22.38%) participants having adverse drug effects involving more than one organ system. A. Adverse drug events (ADE) reported by participants impacting various organ systems; B. Drugs taken for pain relief along with ADE.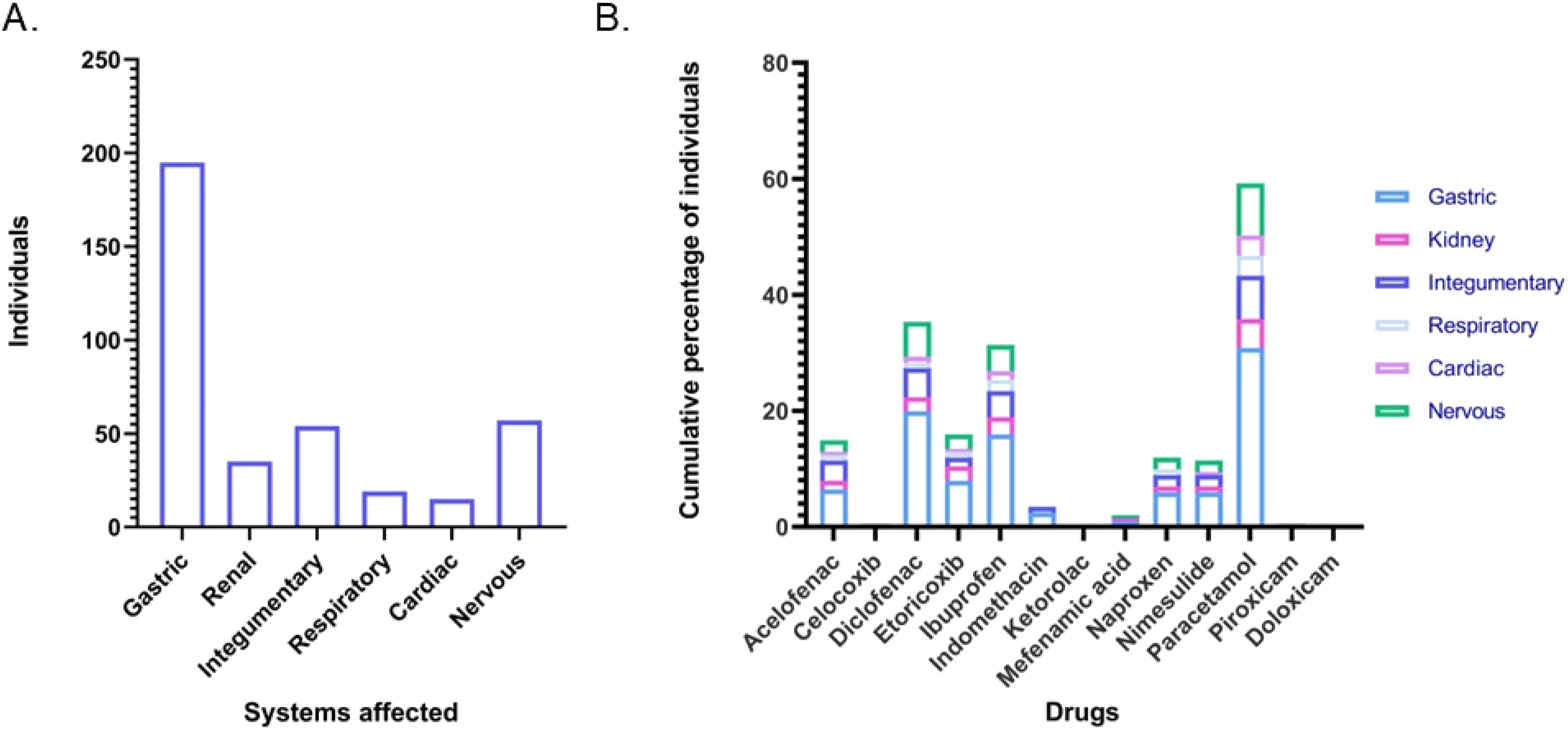
3.4 Risk Factors
Risk Factor* Analysis in NSAID Users With Chronic Pain
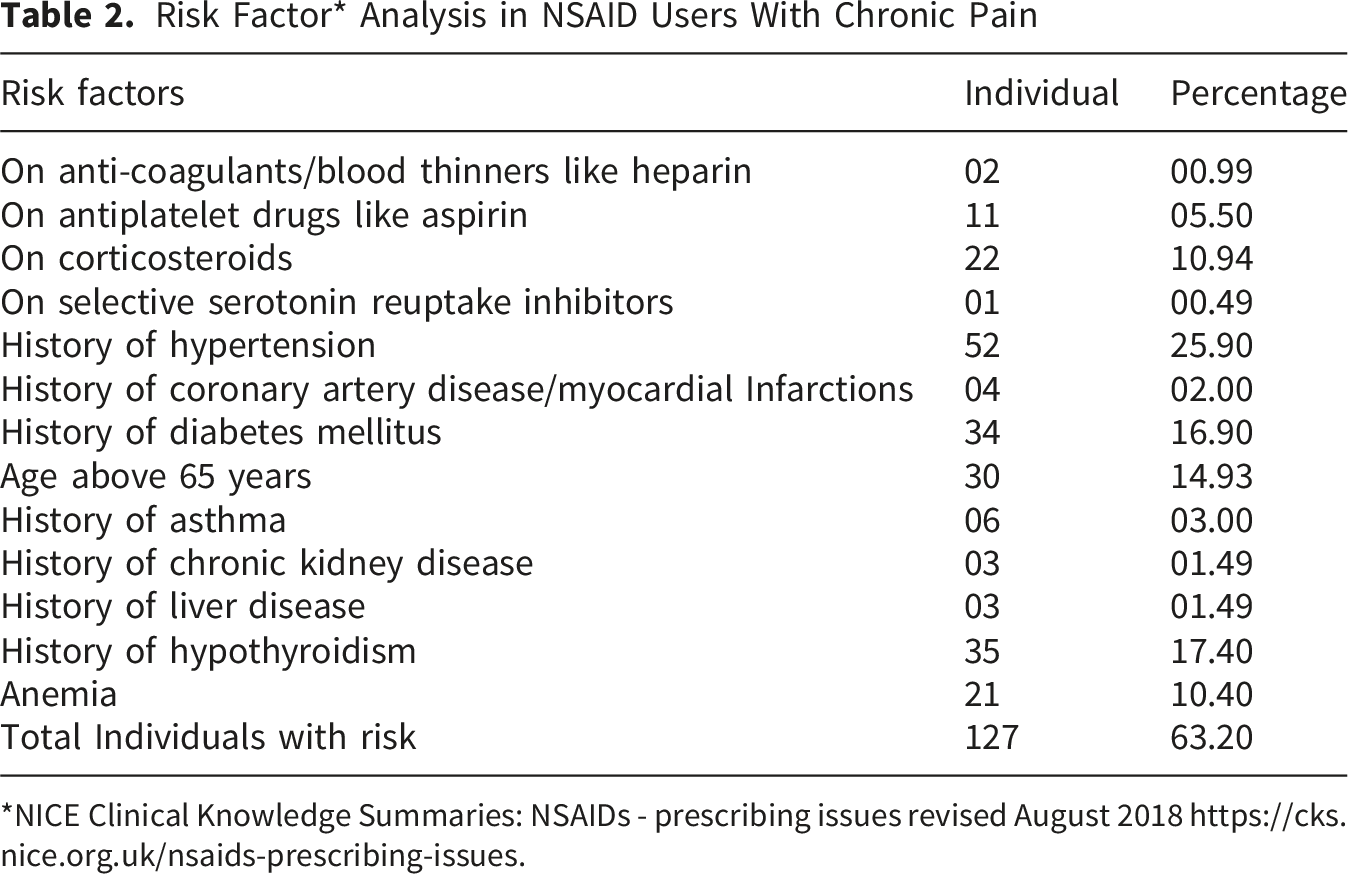
*NICE Clinical Knowledge Summaries: NSAIDs - prescribing issues revised August 2018 https://cks.nice.org.uk/nsaids-prescribing-issues.
3.5 Correlation Between Variables
The correlation among knowledge, attitude, practices, risk factors, ADEs and various demographic factors are tabulated (Supplementary Table 1). Interestingly, the risk factors showed a positive correlation with age and a negative correlation with income. Individuals with prolonged pain conditions showed a positive improvement in KAP. Education and higher income showed a positive relationship with good knowledge, and lower socioeconomic status was correlated with improper practices.
4. Discussion
This is the first study from India to indicate a growing demand for alternative and complementary systems for the management of chronic pain, in addition to providing NSAID-induced adverse events along with risk and KAP. By providing a unique opportunity to analyze the effects of NSAIDs on the population lacking adequate knowledge and compliance towards NSAIDs usage, highlighting a need to improve the prescription patterns, including self-medication in India.
The results unambiguously revealed that half of the population lacked adequate knowledge and was noncompliant. Almost two-thirds of the population wanted to discontinue NSAIDs. In order to maintain safe and effective use of NSAIDs, it is imperative to take into account an individual’s knowledge, attitudes, and practices. 24 Lack of knowledge, time restrictions, unpredictability, and insufficient training in Adverse Drug Reaction (ADR) diagnosis remain major barriers to the inadequate reporting of NSAID-related adverse drug events (ADE) in India. 25 ADE reporting is a complex and time-consuming process but becomes easier, effective and quicker when patients report themselves. 26 Current study highlights the incidence of patient-reported NSAID-induced adverse drug events seen in 66.66% of the study population, with 63.20% having risk for complications. The increased dissatisfaction expressed in the responses indicates an interest in alternative and complementary medicine.
4.1 Knowledge Attitude and Practices (KAP)
Our findings reveal notable gaps in knowledge, with over half of participants unaware of potential drug-drug interactions despite 59% acknowledging the risks of NSAIDs use. Similar reports from other populations highlight that inadequate awareness contributes to improper use and increased risk of adverse outcomes, underscoring the need for targeted patient education. 27 Attitudes towards NSAIDs were ambivalent, with 53% of participants dissatisfied due to adverse effects and higher cost. A significant proportion (62%) expressed openness to alternative or complementary therapies, and 58% reported strong confidence in their efficacy. This aligns with global trends where patients increasingly seek integrative approaches, such as yoga and traditional medicine, to manage chronic pain while minimizing adverse drug events.28,29 Such preferences are consistent with international clinical guidelines that recommend non-pharmacological and mind-body practices as adjuncts in knee osteoarthritis management. 30 Patients are themselves opting for alternative medicine practices owing to dissatisfaction with the current regimen. 15 In chronic progressive painful conditions like osteoarthritis, they often experience declining effectiveness of the pain medicine due to worsening of the disease, further adding to discontentment. About practices, one-third of participants reported consuming higher-than-recommended NSAIDs dosages, and 11% used them on an empty stomach. Only 35% were taking prescribed concomitant gastroprotective agents, leaving a large proportion at risk of gastrointestinal complications. Practice and knowledge can be enhanced by improving communication between patients and healthcare providers. Prescriptions by specialists, including physiatrists, rheumatologists, traumatologists, and pain management specialists, may enhance the outcomes. Currently, it is common for general practitioners to prescribe pain medicine, and specialists are less involved, so patients can benefit if they can be directly referred to a specialist, reducing the time for appropriate care and education. 31 Specialists may pay attention to certain common practices which may be potentially harmful, for example, steroids and NSAIDs together enhance the chances of gastrointestinal bleeding, as steroids prevent ulcer healing, which may be missed by general practitioners. 32 Study findings are consistent with international reports of suboptimal NSAID practices and reflect the challenges of self-medication, particularly in low- and middle-income countries.33,34 Collectively, our findings highlight the need to enhance patient awareness, promote rational prescribing, and integrate safe complementary approaches to optimize pain management, with particular attention to individuals from lower socioeconomic groups to improve their knowledge, attitudes, and practices.
4.2 Adverse Drug Events (ADEs)
Although NSAID use in our study was predominantly intermittent, the incidence of ADEs remained high, with 66.6% of participants reporting at least one event. Gastrointestinal complications were most frequent (30.8%), presenting as acidity, dyspepsia, abdominal pain, and constipation. This aligns with previous reports identifying gastrointestinal problems as the predominant adverse effect of NSAIDs. 35
Other organ systems were also affected, although less frequently. Central nervous system complaints (8.9%) included dizziness and headaches, while dermatological reactions (7.5%) involved hair loss, pigmentation, and rashes, consistent with prior reports. 36 Paracetamol, often perceived as safer, was also implicated in gastrointestinal and cardiovascular events, particularly when combined with NSAIDs, which doubles the risk of gastric bleeding. 37 To optimize treatment selection, active dialogue between patients and healthcare providers is essential. Such communication fosters shared decision-making, by not only sensitizing the patient against the risks and benefits of their treatment, but also enhancing the overall quality of clinical practice by facilitating the prescriber adopt a more individualized approach, as per the patient’s unique risk-to-benefit profile. 8 During outpatient consultations, patients should be thoroughly informed about the potential adverse effects of NSAIDs, existing health conditions, and any previous allergic reactions. Furthermore, patients must be educated and motivated to promptly report any adverse drug reactions (ADRs) to a nearby healthcare facility. To prevent ADE, proper monitoring is required through lab tests to ensure liver and kidney health is not being compromised. 12 Individuals expressing dissatisfaction with NSAID therapy may be guided toward safer and evidence-based alternative treatments, including modalities from traditional medicine.38,39 Taken together, our findings highlight the multifaceted ADE profile of NSAIDs across gastrointestinal, cardiovascular, renal, and neurological systems. Safer prescribing practices, dose minimization, the use of topical formulations where possible and a patient-centred approach with shared decision making between prescriber and patient are therefore critical to reducing the burden of ADEs in populations requiring long-term pain management. 40
4.3 Risk Factor
Risk factors significantly influence the likelihood of NSAID-related complications. Current clinical guidelines emphasize that NSAID therapy should be individualized, with risk-benefit assessments conducted prior to initiation and patients closely monitored throughout treatment. 12 In our study, 31.8% of participants were identified as being at risk, particularly those of advanced age. An interesting study showed a similar finding, wherein 51% of patient population was prescribed NSAIDs even when at risk or when not recommended thereby compounding the potential for harm. 41 While prescribing, it is important to note that NSAID use has been associated with gastrointestinal, renal, and cardiovascular complications, and chronic paracetamol consumption may further aggravate blood pressure control. 42 Long-term and frequent analgesic use has also been linked to functional decline and increased morbidity in older adults. 43 These findings highlight the importance of considering comorbidities, age, polypharmacy, and concomitant risk factors when prescribing analgesics. Studies recommend to develop provider patient relationship through communication to allow them to reframe their experience of chronic pain and also to measure their level of satisfaction.44,45 Educational materials in healthcare waiting areas, such as posters and videos, should be used to improve patient awareness and engagement. Use of patient package inserts, which describe possible adverse events and risk factors associated with the drug, is another solution that allows patients to read and understand the cautions and report their exact risk-associated disease conditions to the prescriber and prevent ADE, which gets missed during short communication in OPD visits. 46 Routine laboratory monitoring can help detect toxic effects at an early stage. Use of proton pump inhibitors to prevent gastrointestinal issues and lowering of NSAIDs dose in CV cases is encouraged. 12 During each visit, patients should also be carefully assessed for any current health conditions that may increase risk. Such measures may improve patient satisfaction and reduce treatment-related complications.
Overall, our results reinforce the need for judicious prescribing and careful monitoring to minimize preventable adverse outcomes. Strengthening deprescribing strategies, particularly in high-risk and geriatric populations, remains an important public health priority.
4.4 Limitations of the Study
The present study had a predominance of female participants using NSAIDs under medical supervision and also, a possibility of recall bias may have contributed to underreporting which may limit generalizability. As a cross-sectional design was employed, establishment of causal relationships is not possible. The present study was primarily planned as a descriptive assessment of knowledge, attitudes, practices (KAP), and patient experience, as outlined in the original study plan. Although we explored associations between KAP domains and adverse drug events, with little success, we have therefore chosen not to emphasize these findings in order to avoid overinterpretations of the results.
5. Conclusion
In this study, most participants were on long-term use of NSAIDs and nursed negative attitudes towards the drugs, probably owing to dissatisfaction with their efficacy, higher costs and ADE. About one-third were at risk, and more than half had already experienced ADE. Some participants held incorrect beliefs and practices related to NSAIDs and required education. The participants showed openness to newer and better treatment modalities, which can facilitate integrating complementary and alternative health practices that are believed to be safer and acceptable. We recommend future large sample, multicentric cohort studies to reduce bias and improve generalizability. We also recommend patient education programs and usage of patient information leaflets to improve knowledge and to sensitize patients for appropriate use of NSAIDs. The study findings will be of immense use to Central Drugs Standard Control Organization (CDSCO) to contribute to the guidelines and recommendation of NSAIDs use in India. We propose establishing and implementing optimal guidelines related to NSAIDs prescription to high-risk individuals to control ADE and reduce the burden on the healthcare system.
Supplemental Material
Supplemental Material - Facing the Side Effects: Patient-Reported Adverse Outcomes of NSAIDs for Chronic Pain Management in North India
Supplemental Material for Facing the Side Effects: Patient-Reported Adverse Outcomes of NSAIDs for Chronic Pain Management in North India by Kavita Bakshi, Ritu Tyagi, Garima Jaglan, Priyanka Rani, Acharya Balkrishna, Pratima Singh, Anurag Varshney in Journal of Patient Experience
Footnotes
Acknowledgment
We sincerely thank Patanjali Ayurveda Hospital for their support in enrolling the participants at the study site. We acknowledge the able assistance from Mr. Devendra Kumawat in designing the conceptual framework for the study. We thank Dr. Robindranath Das and Dr. Himanshu Sharma for reviewing the manuscript. We express our gratitude to the participants for taking the time and energy to contribute to this research.
Ethical Considerations
The ethical approval for the study was obtained from the Institutional Ethics Committee of Patanjali Bhartiya Ayurvigyan Evam Anusandhan Sansthan, Haridwar, Uttarakhand, India (vide approval number- PAC/IEC/2022/36).
Consent to Participate
All participants provided written informed consent before enrolling into the study.
Author Contributions
Kavita Bakshi, Pratima Singh, and Anurag Varshney were accountable for the conceptualization and design of the study. Kavita Bakshi, Ritu Tyagi, Garima Jaglan, and Priyanka Rani collected data. Kavita Bakshi analysed and visualized the data under the supervision of Anurag Varshney and Acharya Balkrishna. Kavita Bakshi wrote the first draft of the manuscript and incorporated changes after a review by Ritu Tyagi, Garima, and Priyanka Rani. Anurag Varshney and Acharya Balkrishna held responsibilities for the project study administration. All the authors have read the manuscript and approve of it.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Patanjali Research Foundation Trust, a not-for-profit organisation, Haridwar India.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available on reasonable request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.