
Abstract
As virtual care becomes embedded in healthcare delivery, understanding the capabilities patients need to engage with these services is critical to safe, equitable access. This study aimed to identify patient capabilities for virtual care engagement described in existing guidance and support resources. Document analysis was used to examine patient-focused documents from Australia and New Zealand. A comprehensive search was conducted across the websites of 83 government departments, healthcare agencies, private healthcare organisations, and consumer organisations. Thematic framework analysis was applied to synthesise the findings. Three overarching capability themes with nine sub themes were identified: (1) Technology and Infrastructure (2) Literacy and Advocacy and (3) Service Engagement capabilities. Most documents prioritised technology and task-based engagement with limited attention to equity, advocacy, safety, privacy and support for priority groups. Findings highlight essential patient capabilities for virtual care and reveal important gaps. However, this study was limited to publicly available documents from two countries and may not fully capture informal or practice-based support available for virtual care use. Future research should examine how these capabilities are enacted in real-world settings and explore patient perspectives across diverse populations to inform more inclusive and equitable virtual care design.
Background
Healthcare delivery is shifting toward greater reliance on digital technologies, with virtual care now a key feature of many health systems following the COVID-19 pandemic.1,2 Virtual care broadly refers to the delivery of health services at a distance using digital and telecommunication technologies, including video and telephone consultations, secure messaging, and remote monitoring tools. 3 This transformation has demonstrated enduring benefits including reduced costs, 4 higher patient and provider satisfaction,5,6 lower infection risks 7 and more efficient use of healthcare resources.8,9 For patients and families, the ability to receive care in the comfort of their homes 10 and gain access in underserved areas has been particularly valuable.11,12
Despite these advantages, patient uptake and the benefits of virtual care remain uneven. Engagement with virtual care is shaped by the “digital divide”, 13 reflecting disparities in technology access, internet connectivity, and digital literacy. 14 Priority groups, including older adults, 15 individuals in lower socioeconomic areas, 14 people living with disabilities, 16 and people from culturally and linguistically diverse (CALD) backgrounds, 17 are most affected. Limited digital and health literacy, concerns around privacy, and a lack of resources can prevent many patients from fully participating in virtual care. 13 These barriers risk reinforcing existing health inequities rather than alleviating them. 18
The rapid shift to virtual care during the pandemic left limited time to assess and address capabilities required by patients, families, and carers to use digitally enabled services. Without adequate support and consideration of these capabilities, healthcare users (i.e. patients, family members or carers), particularly those from priority groups, may be less likely to benefit from virtual services. 18 In the context of virtual care, capability includes not only access to digital devices but also a range of competencies such as using software, managing data, articulating health concerns, and assessing when virtual care is appropriate. 19 , 20
As virtual care becomes increasingly integrated into healthcare delivery, identifying and supporting the capabilities patients need is critical to ensuring positive and equitable patient engagement. While most research has focused on organisational and provider readiness, patient readiness has received less attention.21,22 This study addresses that gap by analysing patient-facing documents from Australia and New Zealand to identify the capabilities patients and families need for effective engagement with digitally enabled care.
Methods
A document analysis was undertaken of patient resources designed to guide the use of virtual care in Australia and New Zealand. Virtual care in this study was defined as any clinical interactions between patients and healthcare providers delivered via telephone or internet-based platforms. Document analysis is a qualitative research method involving the systematic review and interpretation of documents to elicit meaning and develop empirical understanding. 23 It is commonly used in health research to analyse policy and guidance materials and to triangulate findings from other data sources. 23 Given its suitability for analysing documentary evidence, document analysis was considered an appropriate approach for this study to synthesise materials drawn from diverse sources. 24 Data generation, extraction, and analysis followed the READ approach, a recognised method in health systems research comprising four steps: 1) Readying the materials, 2) Extracting data, 3) Analysing data, and 4) Distilling findings.24,25
Readying the Materials
Eligibility Criteria
Documents were considered relevant if they were patient or health care user facing resources designed to support or guide the use of virtual care. Relevant documents from Australian and New Zealand federal and state government departments, healthcare agencies, private healthcare and consumer organisations that addressed patient capabilities for using virtual care, that were publicly available were included in the analysis. The document search was restricted to Australia and New Zealand to ensure relevance to local health policy and delivery context. Capability was defined as the combination of skills and experience as well as the context, environment, and tasks necessary for using virtual care. 26 To capture both pre- and post-COVID-19 perspectives, documents published between 2014 and 2024 were considered. For documents without an explicitly stated publication date, eligibility was determined using contextual indicators of currency, including copyright information, active website maintenance, and references to contemporary virtual care policies, including COVID-19–related expansions. Documents focusing on provider or organisational capabilities related to virtual care were excluded and were addressed separately due to its distinct nature. 21
Document search and Selection
The initial search was conducted by two authors (RW, SO) in August 2024, with the search strategy iteratively refined in collaboration with the research team. Websites of 83 state and federal government health agencies, private healthcare organisations, consumer groups, and health service networks were systematically identified (Supplementary Table 1). A structured search strategy was applied, using key terms organised into three concept groups: (1) virtual care (e.g., telehealth, telemedicine, eHealth, mobile health, remote monitoring); (2) capabilities (e.g., devices, digital skills, digital literacy, guidance, competence, environment); and (3) patients and carers. Searches were conducted manually using site-specific search functions. Additionally, reference lists of eligible documents were reviewed to identify any additional relevant resources.
Data Extraction
A data extraction table was created to capture information aligned with the study’s objectives, with fields informed by literature on digital health competencies and refined through team discussions. The table was initially tested by RW and RH with two documents and then refined through collaboration with the team. The extracted information included the document title, country, type of organisation, organisation name, type of health services, mode of delivery, year of publication, purpose of the document (e.g., guidelines, decision-making support), capability types (technology or other capabilities), and the languages in which the document is available (Supplementary Table 2). Technology-related capabilities were extracted separately to highlight their central role in virtual care. Data extraction was completed by one reviewer (RW) and verified by a second (RH) for accuracy and consistency.
Data Analysis
Extracted data were analysed narratively using an inductive five-stage thematic approach: familiarisation, indexing capabilities, charting categories, mapping to themes, and interpreting findings. 27 Analysis was conducted in Excel to organise and code data. An initial list of 45 capabilities indexed by RW and reviewed by RH was streamlined to 26 after removing duplicates. As no existing framework fit the data, a new thematic structure was developed inductively, with capabilities grouped by conceptual relatedness. An inductive approach also allowed themes to be generated from the data rather than imposed a priori through a deductive framework, enabling the identification of capability domains grounded in the content of the documents. 27 Themes were iteratively refined through team review and discussions with researchers, clinicians, managers, and patients.
Distilling Findings
Preliminary findings were reviewed by the wider research team and discussed with a seven-member steering committee, comprising policy leaders in virtual care, clinicians, and two patient representatives. The role of the steering committee is to provide strategic oversight and advisory input to the study. The committee was distinct from the research team and did not undertake data collection or analysis. Patient members were included based on their lived experience of accessing healthcare services, including virtual care, and their prior involvement in consumer advisory or research activities. Research team and steering committee members provided feedback on the interpretation, relevance, and clarity of findings, and this input was incorporated into the final analysis and reporting.
Results
Documents Characteristics
The search identified 22 relevant resources,28-49 18 from Australia28-36,38-44,48 and four from New Zealand.45-47,49 Four documents were from federal organisations,35,45,46,49 nine from state government agencies,28,31,33,34,38,39,42,43,47 five from professional non-profits,30,36,40,41,48 and four from consumer organisations.29,32,43,44 Seventeen documents included publication dates, ranging from 2020 to 2024. However, the publication date of five documents could not be determined.35,36,38,41,47 Sixteen documents focused on healthcare services in general,28-31,34,35,38-40,42,43,45-47,49 while others addressed specific areas, such as psychology (n=2),36,44 specialist services (n=1), 33 dermatology (n=1), 48 paediatric care (n=1), 32 and cancer care (n=1). 41
Twelve documents focussed on videoconferencing,32,34-36,38-40,42-44,47 seven included both video and telephone,29-31,33,41,48,49 two incorporated patient portals and email alongside video and telephone,45,46 and one addressed all virtual care modalities. 28 While all documents aimed to inform patients, the majority focused on the process of virtual consultations. Only two were available in 21 languages other than English.42,47
Patient Capabilities for Virtual Care
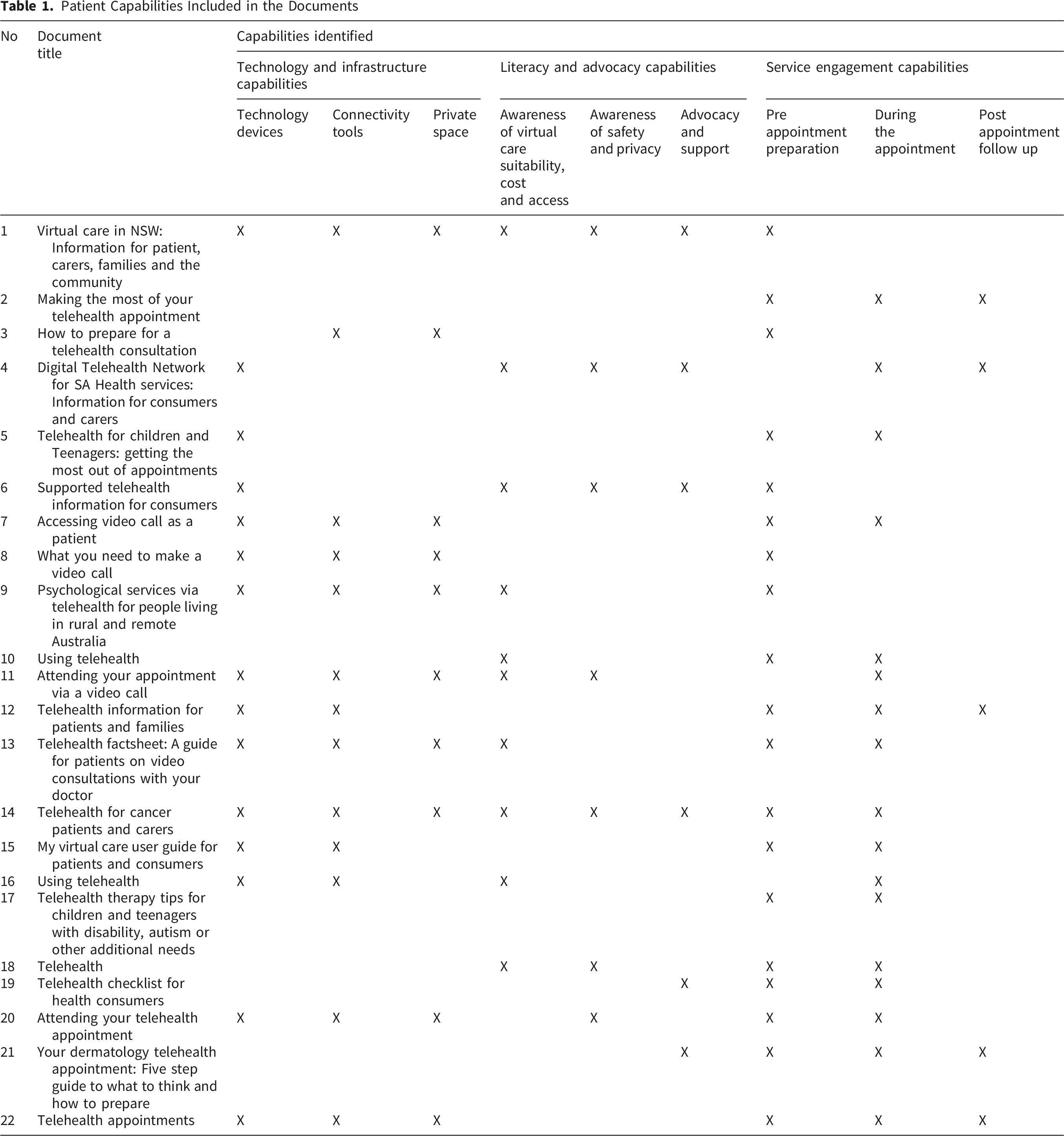
The capabilities identified within the frameworks were initially categorised into nine sub themes, which were then mapped into three overarching themes. An overview of these themes and sub themes is presented in Figure 1. The capability groups included in each document are detailed in Table 1. Notably, no document referenced all identified capability themes and sub themes. Patient capabilities for virtual care identified from the documents Patient Capabilities Included in the Documents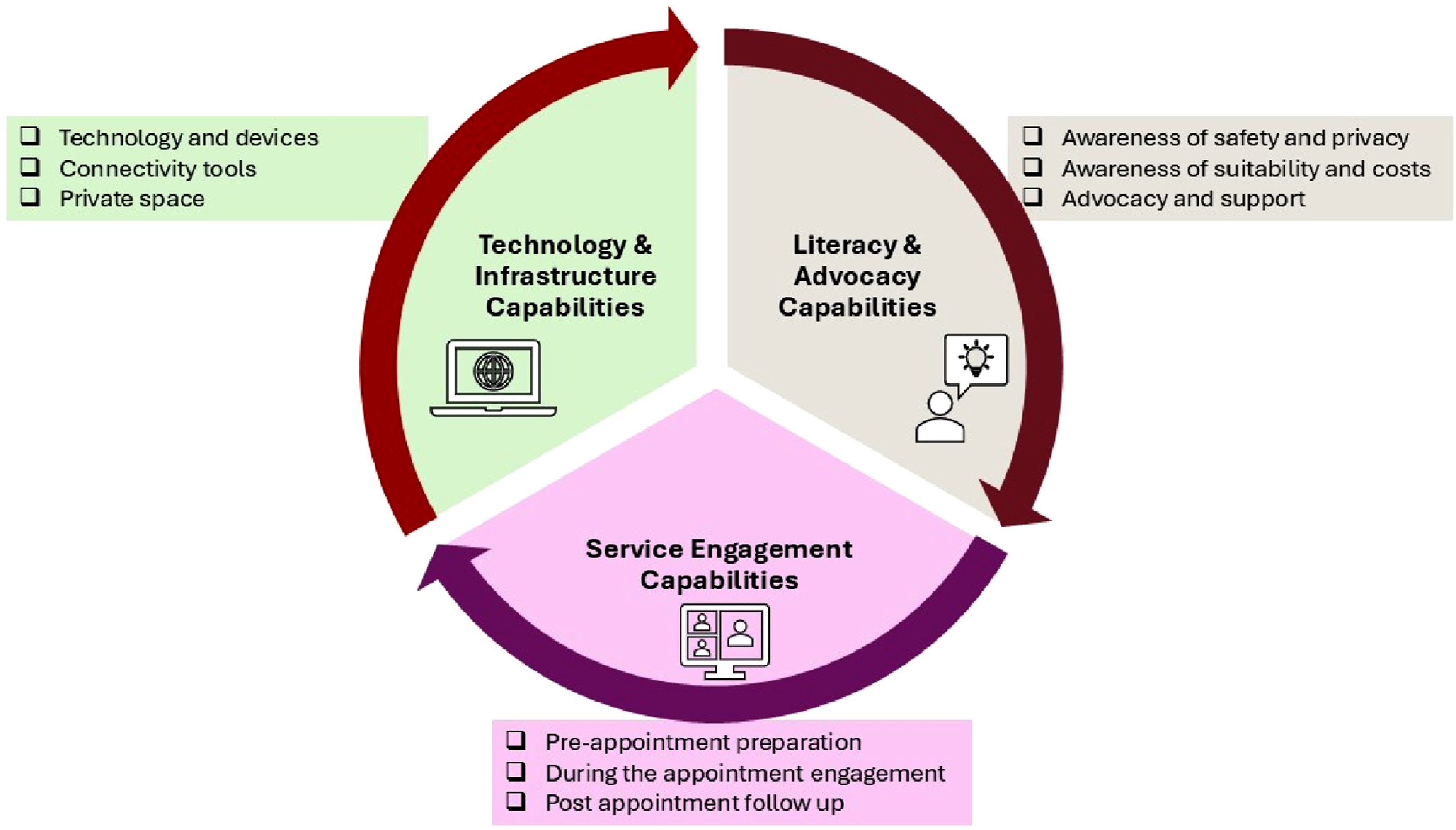
a. Technology and Infrastructure Capabilities
The theme ‘Technology and Infrastructure capabilities’ was synthesised from three sub themes: technology devices; connectivity tools; and private space. Fifteen of the 22 documents emphasised the need for suitable technology devices with camera and microphones, such as a smartphone, laptop, or tablet, for virtual consultations,28,31-36,38-43,47,49 with some recommending up-to-date web browsers, including Google Chrome, Safari, Firefox, or Internet Explorer.34,38,42,47 Two documents from New Zealand specifically advised installing Zoom app.47,49 Two documents also noted the option of accessing virtual services through devices at local service points like community centres or general practitioner (GP) offices.31,36
Connectivity tools were a key consideration in 14 documents,28,31,34-42,47,49 stressing the importance of reliable internet28,30,34-36 and communication tools, such as email or phone number28,49, 41 to book and access virtual care. The private space requirements were discussed in 10 documents, highlighting the necessity for a secure, well-lit, and interruption-free environment to protect confidentiality and support comfort during consultations.28,30,34-36,38,40,41,47,49
b. Literacy and Advocacy Capabilities
The theme ‘Literacy and Advocacy Capabilities’ was derived from three sub themes: awareness of virtual care suitability and cost; awareness of safety and privacy; and advocacy and support. This theme highlights the personal skills required by patients to navigate virtual care, including their ability to make informed decisions about the suitability and cost of virtual services, understand safety and privacy in digital interactions, and effectively advocate for themselves while seeking the support they need.
Awareness of virtual care in terms of suitability, cost, access and choice was addressed in 10 documents,28,31,33,36-38,40,41,43,45 focussing on the capability of patients to evaluate and use virtual care, based on their needs. This included understanding when telehealth is an effective mode of care and when in-person visits may be more suitable.28,43 Financial awareness was discussed in eight documents in the context of understanding the costs associated with telehealth services.28,31,33,36,38,41,45,48 Patients’ ability to find available virtual care services and suitable health professionals who provide those services was also frequently discussed.28,36,37,39,45 Patients’ ability to choose or deny virtual care was highlighted only in 3 documents.28,31,43
Safety and privacy were identified as a critical capabilities in seven documents,28,31,33,38,41,45,47 which generally reassured patients about secure platforms and data protection.28,31,33,38,45,47 Two documents recommended further precautions, such as closing other applications and browsers during virtual consultations.45,49
The advocacy and support category included all capabilities related to the patient’s ability to actively advocate for their health needs within the digital system and seek support when needed. Advocacy and support-related capabilities were discussed in 7 documents28,30,31,33,41,46,48 and included seeking assistance when issues arise32,38 or when dissatisfied with the experience,38,41 requesting interpreters or support persons, when necessary,28,30,48 ensuring clear communication, 30 and requesting privacy for sensitive discussions. 33 One document also stressed clarifying prescriptions, results, and instructions as part of advocacy. 46
c. Service Engagement Capabilities
The service engagement capability theme was derived from three task-oriented sub themes: pre-appointment preparation, during the appointment engagement, and post-appointment follow-up. Pre-appointment preparation, highlighted in almost all documents (n=19),28,30,32-37,39-42,44-49 stressed the need for patients to be well-informed about appointment details, know how to join the virtual consultation, and what to expect.28,30,32 The need to test video and audio quality, ensure a stable internet connection, and confirm the setup ahead of time was mentioned as important.35,39,40,42 Patients were encouraged to prepare by compiling questions and relevant medical information such as conditions, medications, allergies, family history, test results, imaging, and advance care plans.29,30,45 One paediatric focused document advised caregivers to prepare children by discussing what to expect, practicing communication and reassuring them regarding the session. 32
Engagement capabilities required during the appointment were outlined in 17 documents.29,31,32,34,37-49 These included joining the consultation correctly, maintaining eye contact and sharing accurate health information.40,43 Patients were encouraged to speak clearly,41,48 ask questions,39,40,48 provide address details for prescriptions or test requests, 39 and to take notes on any instructions.30,46 In the event of technical issues, it was suggested that patients wait for the healthcare provider to rejoin the session and follow any disruption protocols communicated early in the appointment.31,32,49 Paediatric guidance also emphasised updating clinicians on changes, encouraging verbal communication, and avoiding pressure on children to engage. 32
Post-engagement requirements were less extensively covered (n=3) in the documents but were addressed primarily in relation to follow-up actions, such as completing tests, attending follow-up appointments, and managing medications.29,31,39 One document also recommended providing feedback on the appointment experience, 49 while another emphasised the importance of managing emotions afterwards. 29
Discussion
Examination of 22 documents identified provided insights into patient capabilities required for effective virtual care navigation. These capabilities were grouped into three themes: technology and infrastructure, literacy and advocacy and service engagement capabilities. Most documents focused on task-based engagement and technology requirements, while literacy and advocacy capabilities received less attention, particularly related to safety and privacy, the ability to actively choose or refuse virtual care, and the capacity for self-advocacy and help-seeking. Equity considerations were scarce; only two documents offered multilingual resources for CALD communities. Although the search included documents from 2014 onward, all materials with identifiable publication dates were from 2020 or later, suggesting they were developed during or in response to the COVID-19 pandemic to guide patients through the rapid transition to virtual care. Patient involvement in document development was unclear and likely minimal. Although grounded in the Australian and New Zealand context, the capability domains identified are conceptually consistent with broader scholarship on virtual care and patient engagement, suggesting potential transferability to other healthcare settings implementing virtual models of care.50-52 The prioritisation of task-oriented and technology-focused capabilities mirrors international trends. Resources from Canada and the United States (US), such as the Virtual Care Guide developed by the Canadian Medical Association 53 and materials from the US Department of Health, 54 also prioritise technical skills and procedural guidance. Advocacy and literacy capabilities, when included, were usually confined to assessing care suitability or understanding costs. While this narrow scope is understandable, given that technology and service engagement capabilities remain the leading barrier to virtual care adoption and outcomes,18,55 the documents often stopped short of encouraging patient empowerment. This pattern is notable given evidence that effective patient engagement extends beyond technical instruction, requiring collaboration, usability, proactive communication, and organisational support to ensure safe and active participation. 51 One exception to the otherwise strong focus on technology and infrastructure was the limited recognition of the need for a private space during virtual consultations, a factor essential for ensuring privacy and safety. 56
The limited focus on literacy and advocacy indicates that current guidance helps patients complete virtual care interactions but does little to empower them as active, informed participants in their healthcare journey, a gap with serious equity and experience implications. 57 Given that virtual care inherently introduces a sense of distance between patients and healthcare providers due to the unique nature, 58 it is especially important that patients feel safe to share information, make informed choices, advocate for themselves, and seek support, particularly those facing additional barriers to care.
A key concern identified was the limited discussion regarding safety and privacy in virtual consultations. Few documents provided reassurance on data protection or guidance for safe use, despite these being critical to patient trust. 56 These issues are becoming increasingly complex with the growing integration of artificial intelligence into virtual care, where the use of algorithms to make decisions and the lack of clarity about how data is handled may heighten patient anxiety and erode confidence in providers and the system. 59 Insufficient attention to these concerns may leave patients feeling hesitant to engage with virtual models of care. Addressing this gap through clear reassurance and actionable guidance on privacy protection and virtual safety measures would foster trust and promote a safer virtual healthcare experience.
Another gap was the lack of attention to the digital divide. Few resources were available in multiple languages to support CALD populations, who already face barriers to care and report lower use of virtual services. 60 Cultural preferences for face-to-face care, the role of family in clinical discussions, and heightened privacy concerns in communities with historical distrust of healthcare or government, 61 were not acknowledged. Similarly, little emphasis was placed on making information accessible for people with varying levels of health and digital literacy, or for those lacking devices and reliable internet. Only two documents mentioned alternatives such as providing access through community centres or GP offices. These omissions reflect broader concerns in the literature that digital engagement is shaped by contextual factors such as age, ethnicity, education, literacy, and provider endorsement, and that rapid expansion of virtual models can risk reinforcing existing inequities if usability and access barriers are not intentionally addressed.50,53
Most documents focused on synchronous virtual care via telephone or video, with little attention to asynchronous models such as messaging, patient portals, or remote monitoring. Patient competencies for these emerging models, including written communication, comfort with self-monitoring technologies and control over shared data were rarely mentioned. Similarly, few documents discussed the communication skills patients need in virtual settings, including asking questions, managing non-verbal cues, and maintaining engagement. The concept of telepresence, which influences the quality of virtual encounters, was also largely absent, despite its growing importance in the literature 62 Encouraging patients to make a conscious effort to connect and collaborate can help overcome some of the challenges of the digital medium. 56
None of the documents reviewed addressed all capability themes identified, reflecting variation in purpose, with some focused only on the mechanics of virtual consultations. A national or regional capability framework incorporating technical skills, digital and health literacy, advocacy, safety, cultural inclusivity, and equity could better support patients to manage their care virtually.
This study is the first to synthesise virtual care guidance for patients across Australia and New Zealand with a focus on patient capabilities. While offering valuable insights, the analysis was limited to publicly available documents from these two countries and excluded scholarly literature. As such, it may not fully capture informal, practice-based or locally adapted support mechanisms that support patients or families for virtual care use. Nevertheless, the review followed a structured, transparent process and was informed by input from patients, academics, and healthcare managers, with relevant scholarly literature consulted to strengthen interpretation. Future research should examine how these identified capabilities are enacted in real-world settings and explore patient perspectives through qualitative methods such as interviews or focus groups. Further work is also needed to understand how these capabilities operate across diverse populations to inform more inclusive and equitable virtual care design.
Conclusions
This study shows that while patients are increasingly equipped for basic participation in virtual care, major gaps remain in the range of capabilities being supported. Addressing these gaps is essential for creating a more inclusive environment where patients are not only technically prepared but also empowered, informed, and confident. Developing a comprehensive patient capability framework, encompassing engagement and technology skills, literacy and advocacy, and sensitivity to cultural, linguistic, and literacy diversity, will be critical to realising the full potential of virtual healthcare in a post-pandemic world.
Supplemental Material
Supplemental Material - Building Patient Capabilities for Using Virtual Care: A Document Analysis of Patient Support Resources and Guidance
Supplemental Material for Building Patient Capabilities for Using Virtual Care: A Document Analysis of Patient Support Resources and Guidance by Ramya Walsan, Ashfaq Chauhan, Rebecca Mitchell, Corey Adams, Sagda Osman, Elizabeth Manias, Anita Vandyke, Prince Peprah, Bronwyn Newman, Nadine Elkabbout, Reema Harrison in Journal of Patient Experience
Footnotes
Acknowledgements
We would like to thank the Smarter Hospitals project partners, Health Infrastructure NSW, Western NSW Local Health District, South Western Sydney Local Health District, UNSW Sydney, Western Health, Northern Health, University of Leeds, Townsville Hospital and Health Service, Monash University and Macquarie University, for their support.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by the National Health and Medical Research Council Partnership Scheme grant number: 2015544.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.