
Abstract
Civility, encompassing respect and courtesy, is fundamental to healthy workplace environments but remains inconsistently addressed in academic medicine. This study investigates whether United States (U.S.) medical schools include civility as a criterion in Appointment, Promotion, and Tenure (APT) policies. From August to October 2024, we reviewed publicly accessible APT documents from 143 U.S. medical schools and identified 103 eligible schools. We conducted a keyword-based content analysis using 21 civility-related terms grounded in peer-reviewed literature. While 58.3% of documents referenced professionalism and 23.3% referenced respect or collegiality, only 4.9% mentioned terms like “civil,” “bully,” or “mistreat.” Although 26.2% of APT documents referenced codes of conduct, none included accessible links or consequences for uncivil behavior. Our findings align with the American Association of University Professors’ (AAUP) position that discourages civility as a promotion criterion. However, excluding civility from APT policies may allow incivility to persist unchecked, which can ultimately negatively impact patient care and the healthcare environment. These results suggest the need for standardized institutional processes to report and address incivility, supporting a safe academic environment.
Introduction
Civility is an essential feature of daily human interactions and involves basic courtesy and respect toward other people.1,2 Incivility includes behaviors such as microaggressions, verbal abuse, racism, sexual harassment, bullying, gossiping, intimidation and exclusion. 3 Incivility impacts both individuals and the overall workplace culture. On a personal level, those subjected to uncivil behavior may be excluded from organizational processes, representation, and the collaborative efforts essential to daily work. 4 Others may experience rejection of their contributions such as having one’s expertise, knowledge, suggestions, or practical work dismissed from patients, colleagues and superiors. Moreover, some individuals may experience disempowerment via negative talk such as yelling, berating, belittling, or being scrutinized by colleagues. 5
At the organizational level, incivility is associated with lower job satisfaction, reduced commitment and engagement, and higher turnover. 6 In healthcare, however, incivility is often rationalized or dismissed. Bar-David describes common justifications, including “in a high-pressure environment, it’s okay to skip the niceties;” “people shouldn’t be so sensitive—if you want to enter the kitchen, you have to tolerate the heat;” and “physicians can’t be held accountable for abrasive behavior,” “we’re like a family—we don’t have to monitor everything we say to one another.” 7 These beliefs create blind spots that obscure the problem of incivility among faculty. Moreover, exposure to and experience of uncivil behaviors can perpetuate a cycle of further incivility. 4
Evidence suggest that faculty experienced incivility directly extends to patient care. Freedman et al found that experiencing or witnessing incivility was associated with a 19-75% reduction in the odds of key safety behaviors including teamwork, reporting patient safety events, organizational learning/improvements, management support for safety, and communication openness. 8 Higher rates of reported incivility are also associated with increased risk for near misses, medication errors, nosocomial infections, falls, post-operative complications, and poorer procedural and diagnostic clinical performance.8-14 Collectively, incivility undermines concentration, communication, ability to learn, confidence, interpersonal trust, and workplace psychological safety. 15 Therefore, given these negative impacts on healthcare providers and their patients, addressing incivility in academic medicine is imperative.
Unfortunately, uncivil behaviors are rampant in healthcare, with nearly 90% of health-care workers reporting frequent exposure to incivility.1,16,17 Healthcare providers frequently experience incivilities within their own professional discipline, such as nurse to nurse, instead of across disciplines such as physician to nurse. 18 For academic medical faculty, perpetrators of incivility most commonly are first superiors and colleagues, followed by nurses and patients.19,20 In fact, a mere 5% of faculty and administrators perceive that faculty members work well together. 21 Almost one-third of physicians report receiving weekly or daily rude, dismissive or aggressive communication from other doctors. 22 This is especially relevant in academic medicine since faculty not only educate the future healthcare workforce but also simultaneously provide patient care. While medical and allied health professional leaners, students, residents, and fellows are technically protected from incivilities by policies of training governing bodies, similar protection policies for practicing physicians are institution-dependent and lack standardization.23,24 Additionally, implementing consequences for perpetrated incivility depends on leaders being and feeling empowered by their institutions. These data underscore a pressing need for institutional and national standards that promote civility, explicitly prohibit discourteous and egregious behavior, and foster a psychological safe environment that supports all members of the healthcare team in delivering high-quality patient care.
Since academic medical institutions rely on policies to shape the cultural norms within which faculty work, it follows that these same policies could articulate expectations for civility. One powerful governance mechanism with the potential to function as an upstream determinant of the healthcare environment are Appointment, Promotion and Tenure (APT) policies. Advancement in academic medicine is marked by a sustained record of excellence and impact across clinical care, teaching, research, and service. These same domains are the very categories that affect patient care. Since promotion serves as a major incentive, one potential strategy for addressing incivility is to incorporate expectations for civility into promotion criteria, or, conversely, to prohibit academic advancement when such behavior is absent. Notably, the American Association of University Professors (AAUP) argues that civility should not factor into promotion decisions, 25 yet the well-documented consequences of incivility in academic medicine suggest that APT policies could play a foundational role in shaping faculty culture, and by extension, the conditions under which clinical teams collaborate.
The central aim of this study was to determine whether United States (U.S.) medical schools assess civility within their APT documents. By systematically examining these documents for the presence—or absence—of civility as a criterion for academic advancement, we sought to understand if these powerful documents play a role in articulating expectations for professional conduct.
Methods
From August-October 2024, we used publicly available websites to access APT governance documents from 143 U.S. accredited M.D-granting medical schools. If website searches did not yield results or required an institutional login access, that school was excluded.
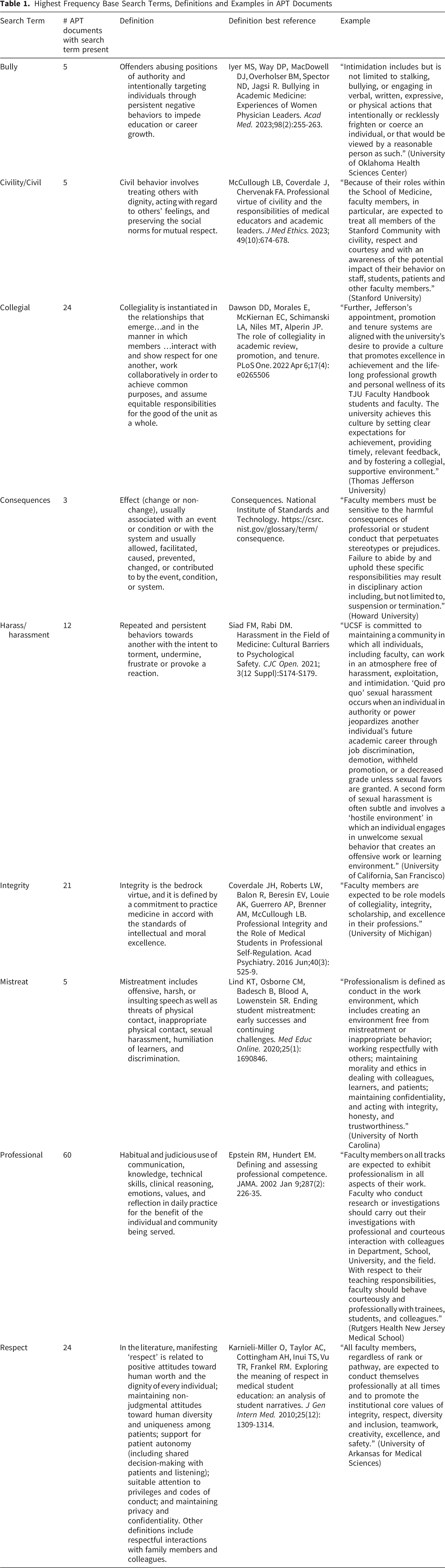
Two reviewers conducted independent searches of keywords associated with civility within each of the accessible APT documents and any discrepancies were resolved though discussions and cross referencing to consensus definitions established through a comprehensive analysis of peer-reviewed literature (Table). Although concepts such as civility, professionalism, collegiality, and mistreatment are often described together, each represents a distinct construct with partially overlapping boundaries. Civility refers to behaviors that promote respect and considerate interpersonal interactions.1,2 Professionalism encompasses the broader ethical and behavioral standard expected of clinicians and faculty, including accountability, integrity, and commitment to excellence. 26 Collegiality reflects behaviors that facilitate effective collaborations, shared decision making and mutual support among peers. 27 In contrast, mistreatment includes behaviors that violate professional norms such as harassment or bullying. 28 We included these constructs, along with 17 additional keywords (accept, behavior, bully, conduct/code of conduct, consequences/repercussions, considerate, courtesy, decorum, defend, discrimination, genial, harass, hostile, integrity, polite, respect, and tact) because they are often referenced when interpreting workplace behaviors, suggesting that they function as an interconnected but not interchangeable framework. This also reduced the risk of overgeneralizing any single construct to all forms of interpersonal or organizational behavior. We used descriptive statistics to analyze the data. This study was approved by Nationwide Children’s Hospital Institutional Review Board.
Results
Highest Frequency Base Search Terms, Definitions and Examples in APT Documents
Discussion
The majority of U.S. medical schools do not consider civility as a category for promotion and tenure. While less than one-third of U.S. medical schools refer to codes of conduct to help guide proceedings regarding civility in the workplace, these codes exist separately from the APT guidelines, further suggesting that there is not a standardized set of criteria for incivility in promotion and tenure evaluations.
These data align with the AAUP’s stance that civility should not be included in the criteria for academic advancement.
25
The AAUP also argues that collegiality—a term we searched for in APT documents—should not be used as a standalone metric for promotion. They caution that “the current tendency to isolate collegiality as a distinct dimension of evaluation…poses several dangers…[including] threaten[ing] academic freedom…and invit[ing] the suppression of dissent…when even the occasional malcontent [has] been known to play an invaluable and constructive role in the life of academic departments and institutions.”
29
However, in the same statement, the AAUP also asserts that “professional misconduct or malfeasance should constitute an
Because promotion is a highly valued
APT documents are uniquely powerful because they determine career advancement, making them stronger drivers of behavior than stand-alone codes of conduct. When civility is not embedded in APT criteria, there is little formal incentive to prioritize it. Reevaluating APT content--and at minimum linking these documents to codes of conduct--could better align institutional expectations with professional behavior and shape upstream conditions in the clinical environment.
Given the current absence of a unified national standard for civility in academic medicine and while simultaneously upholding academic freedom without compromising the core values of academic discourse, U.S. medical schools may consider delineating other pathways to foster civility.25,29 Such efforts may be framed and grounded in the principles of humanism in medicine, including human interests, values, dignity, empathy, and compassionate care. Humanism-aligned professionalism emphasizes that relational behaviors, such as respect, trustworthiness, and ethical engagement, are essential to high quality medical education and clinical care.1,32-34 For example, recognizing that uncivil behaviors undermine the moral goals of healthcare and erodes the humanistic foundation of medicine, institutions could develop zero-tolerance and zero retaliation policies for reporting incivility through confidential mechanisms.23,24,35,36 Given incivility’s documented harms, institutions should also empower leaders to have crucial conversations about lapses in civility and support them in delivering consequences for continued egregious behavior. 37 Finally, beyond linking codes of conduct within APT documents, institutions could foster civility by developing programs that provide restorative support for affected individuals, thereby aligning institutional expectations with the humanistic ideals essential to the practice of medicine.
Implications for Patient Experience
Patient experience was not measured in this study. Nevertheless, these findings informs the understanding of upstream structural conditions, including the inherent hierarchy in academic medicine that shape clinical environments. Future research could use other evaluative methods such as 360-degree evaluations, workforce engagement/pulse surveys, psychological safety reports to determine whether civility is being cultivated through institutionally established mechanisms.
Limitations
While we successfully obtained and evaluated APT documents from over 70% of U.S. M.D.-granting medical schools, we did not include similar documents from D.O.-granting institutions, potentially missing references to civility and consequences for uncivil behavior. Additionally, we did not conduct a separate review of the referenced codes of conduct to determine whether incivility could affect a faculty member’s academic advancement or evaluate if these codes had a minimal set of criteria that would raise concern for incivility. Finally, we did not triangulate the APT documents with institutional governance policies to assess whether consequences for incivility might be enforced through mechanisms other than promotion.
Conclusions
Our study highlights that most U.S. medical schools do not use civility as a criterion for promotion and tenure. Since incivility is prevalent in academic medicine, institutions may consider developing standardized processes that allow faculty to report incivility and also creating programs that support leaders in addressing uncivil behaviors. The impact of incivility cannot be overstated, as it adversely affects faculty members, their teaching, scholarship, and service—core tenets emphasized by both the AAUP and medical schools in consideration for promotion. More importantly, incivility carries significant negative consequences for targeted individuals, affecting their well-being, performance, and professional engagement, the workplace culture, and above all, the quality of care that they provide to patients.
Footnotes
Ethical Considerations
This study (STUDY00003551) was approved by Nationwide Children’s Hospital.
Consent to Participate
Patient consent is not required or applicable for this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data is available and can be shared.