
Abstract
Introduction
Pain is a significant concern for cancer patients, particularly those in advanced stages of the disease, and it affects not only physical well-being but also psychosocial and emotional aspects. Effective pain management is critical in cancer care, with nurses playing a pivotal role in assessing and managing pain.
Objectives
This study aimed to evaluate nurses’ knowledge and attitudes regarding pain assessment and management at a specialized cancer center in Amman, Jordan.
Methods
A descriptive, cross-sectional study was conducted at a specialized cancer center. A total of 260 questionnaires were distributed to nurses, and 184 responses were received, resulting in a response rate of 70.8%. A convenience sample of registered nurses participated, completing the “Knowledge and Attitudes Survey Regarding Pain” (KASRP). Data were analyzed using SPSS with continuous variables presented as means and standard deviations (SD), and categorical variables as frequencies and percentages, Pearson correlation examined relationships among age, experience, and knowledge scores; multiple regression identified factors influencing total knowledge.
Results
The study had a response rate of 70.8%. Nurses’ knowledge scores ranged from 10 to 38, with a mean score of 22.98 (SD = 6.11). A weak but positive correlation was found between total knowledge scores and both age and years of nursing experience. Key gaps in knowledge were identified, particularly regarding cancer-related pain, substance abuse, and physical dependence. More than 50% of nurses correctly answered 26 of the 41 KASRP items, while 15 items had a correct response rate of less than 50%.
Conclusion
The study revealed significant gaps in nurses’ knowledge and practices regarding pain management, especially in areas related to cancer-related pain and opioid use. Increased experience in oncology nursing was associated with improved knowledge and practices. The findings highlight the need for targeted educational interventions to enhance pain management competencies among nurses, ultimately improving patient outcomes.
Introduction
Pain is a common and significant issue for cancer patients, particularly those with advanced or metastatic disease. It is not only a physiological stressor but also affects psychosocial, emotional, and financial well-being (Snijders et al., 2023). Despite pain acts as a protective mechanism that prompts individuals to seek medical attention, its impact is often negative, necessitating effective management strategies (D’emeh et al., 2016). As a universal human experience, pain affects individuals of all ethnicities, genders, ages, and socioeconomic backgrounds, making it a global health concern. In cancer care, addressing pain is a critical component of nursing practice, requiring adequate knowledge, positive attitudes, and effective approaches to pain assessment and management (Mangolian Shahrbabaki et al., 2024).
Various standardized instruments have been developed to assess pain and related outcomes. For example, the Brief Pain Inventory (BPI) is widely used in cancer research to evaluate both the severity of pain and its impact on daily functioning, including mood, activity, and sleep (Harrington et al., 2018). This study utilized the Knowledge and Attitudes Survey Regarding Pain (KASRP), a well-established and widely used instrument designed to evaluate healthcare providers’ knowledge and attitudes toward pain assessment and management, encompasses key domains such as pain physiology, opioid use, pain assessment principles, and clinical decision-making, making it a suitable tool for assessing nurses’ competencies in cancer pain management (McCaffery & Robinson, 2002).
Literature Review
Approximately 50%–80% of hospitalized patients report experiencing pain, making it one of the most prevalent and distressing symptoms during hospitalization (Anekar et al., 2025; Gregory & McGowan, 2016). Ethically, no patient should endure avoidable pain. International human rights law recognizes the right to receive appropriate and effective pain relief as fundamental, contributing to an improved quality of life (AL-Sayaghi et al., 2022). Despite advancements in pain research and its prioritization in healthcare, between 39% and 60% of cancer patients report insufficient pain management, often due to inadequate analgesic care (Liu et al., 2021).
Pain assessment in nursing practice involves subjective measures, such as patient self-reports, as well as objective indicators, including nonverbal cues and facial expressions (Miller & Newton, 2006). However, challenges remain, as many nurses in general practice settings lack the necessary skills and confidence to assess and manage pain effectively. Their attitudes toward pain assessment also influence the quality of care provided (Ung et al., 2016). Despite evidence-based guidelines and technological advancements, inadequate pain management continues to affect patients (Gentile et al., 2011), and traditional pain assessment tools may not always be suitable for cancer patients.
Pain in cancer patients presents unique challenges that differ from those in the general hospitalized population. Cancer-related pain is often multifactorial, arising not only from the disease itself but also from treatments such as chemotherapy, radiation, and surgery (Paice & Ferrell, 2011). It significantly impacts patients’ physical, emotional, and social well-being, thereby diminishing quality of life (Schmitz et al., 2021). Managing this pain requires a multidimensional approach that addresses both the sensory and affective components of pain, necessitating specialized knowledge and skills among oncology nurses (Mestdagh et al., 2023).
Despite advances in analgesic options, cancer patients frequently experience undertreated pain due to barriers, including inadequate assessment tools, misconceptions about opioid use, and lack of specific oncology-focused training among nursing staff (Obaid et al., 2023). These barriers mean that traditional tools such as the Numeric Rating Scale (NRS) and Visual Analogue Scale (VAS), while widely used for pain assessment; they may not fully capture the complexity of cancer-related pain. Recent studies suggest that multidimensional tools like the Brief Pain Inventory (BPI) provide a more comprehensive evaluation, considering both pain severity and its impact on daily activities. The (BPI) was specifically developed for use with cancer patients to assess both pain intensity and its interference with daily functioning, providing an advantage over unidimensional scales like the NRS and VAS, which may underestimate the complexity of cancer-related pain (Harrington et al., 2018).
Effective pain management is a critical indicator of nursing and healthcare quality. As frontline caregivers who spend more time with patients than other healthcare providers, nurses require a strong knowledge base in pain assessment, management, and patient education to effectively alleviate pain across all healthcare settings. Achieving adequate pain relief requires interdisciplinary collaboration, however the responsibility for ensuring patients’ comfort and quality of life is shared throughout the healthcare team. To fulfill this role, nurses must stay informed about pain management principles and develop the appropriate attitude and skill sets for assessing and managing pain (AL-Sayaghi et al., 2022).
Several studies have examined nurses’ knowledge and attitudes toward cancer pain management. Al Qadire et al. (2012) focused on general hospital nurses and reported low overall pain knowledge, with many lacking recent pain-related education. Similarly Alnajar et al. (2019) examined oncology nurses and found only fair knowledge and attitudes, identifying gaps in pharmacologic pain control and negative attitudes toward opioid use and routine pain assessment. Othman and Al-Atiyyat (2022) further assessed barriers and general pain management practices and reported similar knowledge deficits. However, none of these studies specifically evaluated pain assessment practices, an area critical for oncology patients who frequently experience significant pain.
The current study was conducted at a specialized oncology center with trained oncology nurses and a dedicated pain management team, providing a unique setting to examine how pain assessment was conducted in practice. By evaluating nurses’ knowledge, attitudes, and practices regarding cancer pain assessment and exploring how factors such as educational level, years of experience, and clinical unit influence these outcomes, this study provides new, context-specific insights that can inform targeted educational strategies and improve pain assessment and patient care in oncology settings.
Given these gaps, exploring nurses’ knowledge, attitudes, and practices regarding pain assessment among cancer patients is essential, as effective pain assessment forms the foundation for developing robust pain management strategies, ensuring patient comfort, enhancing quality of life, and improving clinical practice (Kiwanuka & Masaba, 2018).
Purpose of the Study
This study aimed to evaluate nurses’ knowledge, attitudes, and practices regarding pain assessment and management at a specialized oncology center.
Methods
Study Design
A descriptive, cross-sectional design was employed in this study. This approach allowed for a snapshot of the existing knowledge and attitudes among the nursing staff, providing valuable insights into areas that may require targeted educational interventions or policy changes to improve pain management practices.
Research Question
How did nurses’ knowledge and practices in cancer pain management vary by educational level, experience, and work setting?
Study Setting
The study was conducted at a Specialized Oncology Cancer Center. Potential participants were recruited among nurses working in various clinical units within the cancer center, including medical oncology, surgical oncology, hematology, and palliative care units of the cancer center.
Study Population
The sample included registered nurses who met the inclusion criteria, which required having aminimum of six months of experience working at the center and a willingness to participate in the study.
A convenience sampling method was employed to recruit participants; the study was conducted over six months, from November 2022 to May 2023. Investigators clearly explained the aim and purpose of the study to each potential participant. Those who agreed to participate were asked to complete a questionnaire, which was accompanied by a cover letter detailing the study’s objectives, procedures, and ethical considerations.
Inclusion Criteria
Registered nurses with a minimum of six months of clinical experience were included. This timeframe was selected to ensure that participants had adequate exposure to oncology-related pain assessment and management practices, as well as sufficient time to adapt professionally and become familiar with institutional protocols. Participation was voluntary, and all participants were required to possess sufficient proficiency in English to understand and complete the questionnaire, which was administered in English, investigators confirmed that all participants met these inclusion criteria before enrollment.
Exclusion Criteria
Nurses working in operating rooms, practical nurses, nurse managers, and directors were excluded from the study to maintain consistent focus on clinical nursing staff directly involved in routine patient care.
Sampling
The sample size was calculated using Cochran’s formula for proportions:

Z = 1.96 (corresponding to a 95% confidence level).
P = 0.5 (assumed proportion of nurses with adequate pain management knowledge; this value maximizes sample size when no prior estimate is available).
E = 0.05 (margin of error).
This calculation gave an initial sample size of 384. Because the total population of eligible nurses was 800, the finite population correction was applied:

Due to practical constraints, a convenience sampling method was used, and 184 nurses who met the inclusion criteria and consented to participate were recruited. While the final sample was smaller than initially calculated, it still provided adequate statistical power to examine nurses’ knowledge, attitudes, and practices regarding pain management.
Data Collection and Instruments
Data were gathered using a two-part, self-administered questionnaire. The first section collected socio-demographic information, including age, gender, years of experience, and educational background. The second section assessed nurses’ knowledge and attitudes regarding pain assessment and management using the standardized “Knowledge and Attitudes Survey Regarding Pain” (KASRP). All data collection was conducted in English, given that the participating nurses were proficient in the language. Consequently, the KASRP was administered in its original, validated English version without the need for translation..
The KASRP, originally developed by Ferrell and McCaffery in 1987, has undergone multiple revisions, with the most recent update in 2014. It has established validity and reliability, with a test-retest reliability coefficient of 0.80 and an internal consistency (Cronbach’s alpha) of 0.70 (Ferrell, 2014). The purpose of the KASRP is to evaluate nurses’ factual knowledge and attitudes toward pain management, especially in clinical decision-making.
The selection of the KASRP was based on its extensive use in both oncology and general hospital settings, as well as its demonstrated validity and reliability within oncology context. (Truong et al., 2024). The tool has proven effective in evaluating nurses’ knowledge and attitudes regarding pain and in assessing the impact of educational interventions aimed at improving pain management practices.
The KASRP demonstrates strong psychometric properties in assessing both knowledge and attitudes related to pain management across diverse clinical settings. Its applicability in oncology nursing has been well-documented, making it a suitable tool for evaluating cancer-specific pain competencies (Ung et al., 2016).
The questionnaire is widely used in various languages and clinical contexts. The KASRP contains 41 items, including 22 true/false questions, 15 multiple-choice questions, and 4 additional multiple-choice questions based on two case scenarios. According to the authors, the items are not strictly categorized as assessing knowledge or attitudes due to the overlap in content, which often measures both variables simultaneously. This structure enables the assessment of both cognitive accuracy and clinical reasoning in pain-related scenarios.
In the case scenarios, nurses are asked to assess and manage pain for two patients with different behaviors. In scenario A, the patient is smiling, talking, and joking with visitors, while in scenario B, the patient is lying quietly and grimacing as they turn in bed. These scenarios aim to explore the nurses’ assessment skills and pain management decisions based on observed patient behavior.
Variables
The primary outcome of this study was the level of nurses’ knowledge and practice regarding pain assessment and management. The key exposures or predictors examined included demographic and professional factors such as age, gender, years of nursing experience, educational level, and the clinical unit in which the nurse worked. Potential confounding variables considered were academic degree, previous experience in oncology nursing, and prior training related to pain management. These factors were assessed to understand their influence on nurses’ competencies and to control for their effects during statistical analysis.
Statistical Analysis
Data were analyzed using Statistical Package for the Social Sciences software (SPSS) version 25. Missing data were addressed by replacing missing values within the mean score of the computed variable on the same scale when more than half of the items were answered (Cappelleri & Bushmakin, 2014).
Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize demographic characteristics and study variables. Independent t-tests were conducted to compare mean total knowledge scores across categorical variables such as gender, educational level, and department. Pearson’s correlation analysis examine the relationships between continuous variables, including age, years of experience, and total knowledge scores.
Multiple linear regression analysis was performed to identify factors associated with nurses’ total knowledge scores. Years of experience, educational level, and department (grouped) were entered simultaneously into the model. A p-value of < 0.05 was considered statistically significant.
Ethical Considerations
This study was approved by the Institutional Review Board of a referral oncology center (Approval No. 22 KHCC 143, dated September 12, 2022). Participation was entirely voluntary, with no pressure or coercion exerted on any participant.. All participants received a cover letter explaining the study’s purpose, procedures, and voluntary nature. Nurses were given adequate time to read the information and ask questions before completing the questionnaire. A waiver of signed consent documentation was approved by the Institutional Review Board to allow for implied consent through questionnaire completion. Participants were informed of their right to withdraw from the study at any time without any penalties. Before participation, all nurses were provided with a detailed information sheet and given the opportunity to ask questions. Privacy was maintained by allowing participants to complete the questionnaire in a private and comfortable room. Confidentiality was ensured by securely storing the hard copies questionnaires in a locked cabinet and the digital files on a password-protected computer. Personal data were protected, and any identifying information was kept confidential.
Results
Participants’ Demographics and Comparison of Total Knowledge Scores (n=184)

Note. *p < 0.05 is statistically significant.
Analysis of total knowledge scores by demographic variables (Table 1) showed that male nurses had a slightly higher mean knowledge score (23.67 ± 6.09) compared to female nurses (22.38 ± 5.50), although this difference was not statistically significant (p = 0.138). Educational level was significantly associated with knowledge scores, with nurses with a postgraduate degree scored higher (mean = 24.00 ± 6.52) than those with a undergraduate degree (mean = 22.13 ± 5.01, p = 0.031). This suggests that advanced education may contribute to better knowledge of pain assessment and management. Furthermore, nurses working in the medical-surgical department scored significantly higher (mean = 23.75 ± 6.25) than those in other departments (mean = 21.20 ± 4.14, p = 0.006), possibly reflecting more frequent exposure to pain management cases in these units.
Correlation
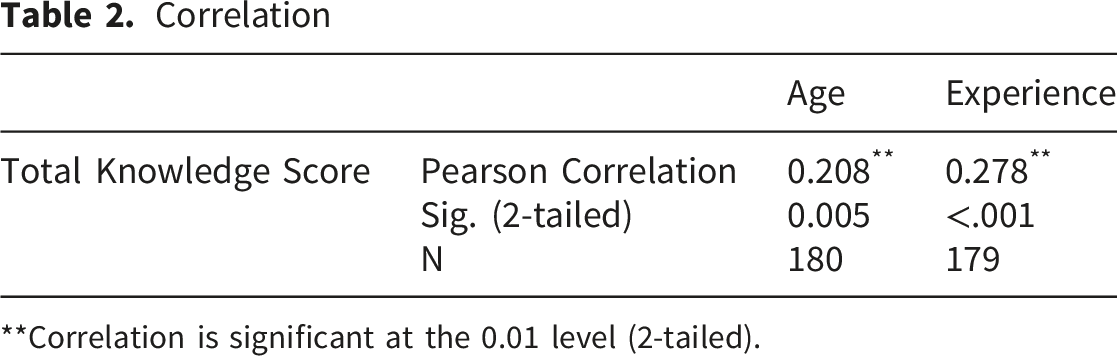
**Correlation is significant at the 0.01 level (2-tailed).
Total Knowledge Score

The Distribution of Correct and Incorrect Responses for the 41 Items on the Questionnaire

Although pharmacological items generally had high correct response rates, further analysis revealed gaps in advanced areas such as opioid titration, management of side effects, and misconceptions about addiction. This highlights the need for ongoing education focused not only on basic pharmacological knowledge but also on complex clinical decision-making. Conversely, 15 items had a correct response rate of less than 50%, with three questions (28, 39, and 41) answered correctly by fewer than 30% of participants. These items were mainly associated with knowledge and practice about cancer-related pain, substance abuse, and physical dependence.
Multiple Linear Regression Analysis of Factors Associated With Nurses’ Total Knowledge Score

aDependent Variable: Total Knowledge Score Model F = 7.593, p < 0.001; R2 = 0.116.
Discussion
This study assessed the knowledge and practices of nurses at the specialized Oncology Center in Jordan concerning cancer pain assessment and management. The findings revealed that increased age and nursing experience were positively associated with better knowledge and practices in pain assessment and management among cancer patients. This highlight that experience in oncology nursing plays a crucial role in shaping competencies in managing cancer pain. However,the identified knowledge gaps in pain assessment principles represent a significant barrier to effective pain management for cancer patients. Recognizing and addressing these deficiencies is a critical step toward enhancing pain management practices in oncology settings.
These results are consistent with previous studies in similar settings. For instance (Yildirim et al., 2008), found that nurses with advanced degrees demonstrated significantly better knowledge and attitudes toward pain management. Similarly (Al-Shaer et al., 2011), highlighted that experienced nurses scored higher on knowledge and attitude measures regarding pain assessment and management, which may be attributed to their greater clinical exposure and accumulated practical experience, this is also supported by (Alqahtani & Jones, 2015).
Another study by (Brant et al., 2017) also supports this correlation, noting that nurses with postgraduate education and specialization in oncology scored higher on pain management knowledge assessments. The consistent findings across multiple studies indicate that both education and hands-on experience contribute significantly to improving pain-related clinical decisions and interventions, specifically nurses with higher educational qualifications scored significantly better in knowledge and attitude measures, this likely reflects reflect not only their academic background and clinical experience, but also their increased engagement in evidence-based practice, motivation for continuous learning, and heightened responsiveness to patients’ complex needs. Similar findings have been reported in studies highlighting the role of advanced education in enhancing pain management competencies. (Bernardi et al., 2007; Yildirim et al., 2008).
Despite the positive correlation found in this study, some gaps remain in specific areas of knowledge, particularly concerning the pharmacological management of cancer pain. This reflects findings by (Matzo & Sherman, 2014), who noted persistent misconceptions and knowledge deficits among nurses, even among those with considerable experience, especially regarding opioid usage and side effect management, these findings highlight the critical need for ongoing professional development and specialized training in pain management, particularly in oncology settings. Integrating comprehensive pain management modules into nursing curricula and encouraging participation in continuing education could bridge this existing knowledge gaps.
Furthermore, cultivating a positive attitude toward pain assessment protocols is essential. While knowledge is foundational, a proactive attitude ensures that pain assessment is consistently prioritized in patient care. Studies such as (Bernardi et al., 2007) emphasized the importance of attitude, reporting that nurses who valued pain management were more likely to implement standardized assessment tools effectively.
The response rate of 70.8% indicates a strong interest among nurses in pain management, providing a valuable opportunity to identify areas needing improvement in pain assessment knowledge and practice. Using the KASRP questionnaire enabled an effective evaluation of the nurses’ competencies in pain management. Our results show that while many nurses demonstrated a good level of knowledge and practice concerning pain assessment and pharmacological interventions, there were notable gaps in knowledge regarding cancer-related pain, substance abuse, and the management of physical dependence.
Several factors influence nurses’ approaches to pain management, including their personal experiences with pain management and the use of analgesics. These experiences can significantly shape their attitudes toward pain treatment, potentially impacting their practice and patient outcomes. Understanding these influences can guide strategies to optimize pain management in clinical practice.
The study also alignes with existing literature that suggests nurses may lack sufficient knowledge about pain medications, especially opioids. A study by Ali et al. (2024) highlighted that many nurses report insufficient knowledge of pharmacokinetics and pharmacodynamics of opioids, leading to concerns about their administration in clinical settings. Nurses’ lack of confidence in managing opioid therapy has been linked to the under-treatment of pain, especially in vulnerable populations, such as those with a history of substance use disorder.
A common misconception identified was the ethical concern regarding the administration of opioid analgesia to patients with a history of substance abuse, even if they are experiencing significant pain. (Morley et al., 2015) emphasize that healthcare providers, including nurses, often struggle with the moral conflict of balancing the need to relieve pain with the risk of potential opioid misuse in these patients. Nurses may inadvertently deny effective pain relief to these individuals due to fear of contributing to substance abuse relapse. This aligned with the findings of our study, where misconceptions about the ethical responsibility of providing opioids to patients with substance abuse history were prevalent. Multiple linear regression showed that years of clinical experience and department of practice significantly predicted nurses’ total knowledge score, while educational level did not.
Consistent with previous research, Al Qadire and Al Khalaileh (2012) found that prior pain education, rather than formal education, increased knowledge scores. Brant et al. (2017) reported higher knowledge among nurses with >5 years of experience and recent pain education. Moreover, Al-Sayaghi et al. (2022) showed that nurses’ knowledge varied by department, reflecting the influence of clinical exposure.
These findings emphasize that practical experience and workplace context are stronger determinants of pain management knowledge than educational level. Nevertheless, even though overall knowledge is influenced by clinical experience and department, targeted educational interventions are still necessary to ensure safe and ethical management of complex cases, such as opioid use in patients with a history of substance abuse. According to (El-Aqoul et al., 2020) an education program focused on the principles of pain management, including the safe use of opioids in high-risk populations, can significantly increase nurses’ confidence and improve their ability to make evidence-based decisions. This highlights the need for targeted training programs to enhance nurses’ skills in managing pain, especially in complex cases involving patients with substance abuse histories. A study by (Bell & McCurry, 2020) demonstrated that pain management education tailored to addressing specific concerns, such as the use of opioids in patients with substance abuse histories, not only improves knowledge but also influences clinical behavior, leading to more appropriate pain management strategies. This is consistent with our study’s conclusion that educational interventions are crucial in overcoming the ethical concerns that arise when administering opioid analgesia to these patients.
Strengths and Limitations
Strengths
This study had several important strengths. First it was conducted in a specialized oncology center, providing a relevant clinical context for evaluating cancer pain management. Second: the use of the validated KASRP instrument supported the reliability of the findings and enabled comparison with previous studies. Third, the relatively high response rate (70.8%) enhanced the representativeness of the sample, fourth, including nurses with varying levels of education, experience, and clinical units offered a comprehensive understanding of factors influencing knowledge and practice. Fifth, the study examined both knowledge and attitudes, offering a more holistic perspective on pain management competencies. Finally, the study provides valuable context-specific insights for Jordanian oncology settings, contributing to the limited literature in this region.
Limitations
This study had several limitations that should be acknowledged. The findings may have limited generalizability to other healthcare settings or regions, as the study was conducted at a single oncology center in Jordan. The self-reported nature of the questionnaire may introduce response bias, as participants might overestimate their knowledge or report socially desirable practices. While the study explored associations between demographic factors and pain management knowledge, the cross-sectional design prevents any conclusions about causality. Additionally, some variables had minimal missing data, and although a mean imputation strategy was used, this may have influenced the accuracy of certain results. Lastly, the questionnaire relied on participants’ recall and self-assessment rather than objective observation of clinical practice, which may affect the validity of the practice-related findings.
Implications for Practice
Nurses require focused, continuing education programs to improve their understanding of complex aspects of cancer pain management.
There is a clear need for support and training for novice nurses, particularly those with less experience and lower educational levels. As these nurses scored significantly lower, indicating that structured mentorship and training programs are important to enhance their professional development and confidence in pain assessment and intervention.
Specific training is also necessary to address the department-specific knowledge gaps. Nurses working outside medical-surgical units had significantly lower scores, emphasizing the importance of providing interdepartmental training to ensure consistent, high-quality pain management.
In-service training can help standardize knowledge and reduce practice variability. This approach can promote evidence-based practice and ultimately improve patient outcomes.
Conclusion
This study highlights the importance of enhancing nurses’ knowledge and practices regarding pain assessment for cancer patients at the Oncology Center in Jordan. The study emphasize the positive correlation between age and clinical experience in developing pain management competency. Furthermore, the study identified knowledge gaps, concerning cancer-related pain, substance abuse, and physical dependence, underscoring the need for ongoing education and training. Addressing misconceptions, especially those surrounding opioid use in patients with a history of substance abuse is essential for effective pain management.
The high response rate to the study reflects a strong level of engagement among nurses, suggesting a readiness for educational initiatives which improve patient outcome. Targeted interventions and continuous professional development programs are essential to delivering optimal pain management and enhancing the quality of care for cancer patients.
Footnotes
Acknowledgements
We express sincere gratitude Nursing Department for their unwavering support and facilitation of essential resources. Acknowledgment is also extended to the Nursing Research Unit for their comprehensive support and oversight of this project.
Ethical Considerations
This study was approved by the Institutional Review Board of King Hussein Cancer Center (Approval No. 22 KHCC 143, dated September 12, 2022).
Consent to Participate
All participants received a cover letter explaining the study’s purpose, procedures, and voluntary nature. Nurses were given adequate time to read the information and ask questions before completing the questionnaire. A waiver of signed consent documentation was approved by the Institutional Review Board to allow for implied consent through questionnaire completion. Confidentiality and privacy were maintained throughout the process.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Mohammad Alkelani, Besan Albaba, and Farah Alqatawneh. The first draft of the manuscript was written by Mohammad Alkelani, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors are committed to providing access to the data and supporting materials upon request.