
Abstract
Introduction
Humanistic leadership has gained increasing attention in nursing as an approach that highlights empathy, respect, and ethical care for others. Although it has the potential to improve nurses’ professional growth and work environment, evidence regarding humanistic leadership among nurse interns remains limited. In clinical training settings, workplace violence and caring behavior are still major issues often affecting interns’ professional identity and overall performance. Little is known about how humanistic leadership is linked to workplace violence and caring behavior among nurse interns, or whether professional identity can explain these relationships.
Aim
This study aimed to investigate the role of humanistic leadership in reducing workplace violence and promoting caring behavior through the mediating effect of professional identity among nurse interns, using structural equation modeling.
Methods
A correlational cross-sectional design was conducted among nursing interns in Zagazig and Mansoura University hospitals, Egypt. Four standardized questionnaires were used to examine perceptions of humanistic leadership, professional identity, workplace violence, and caring behavior. The study’s hypothetical model was examined using AMOS structural equation modeling (SEM).
Results
A total of 1170 completed questionnaires were returned and considered valid for analysis, conforming to a response rate of 93.6%. Humanistic leadership revealed significant and positive correlations with nurse interns’ professional identity (r = 0.589, p < 0.001) and caring behavior (r = 0.426, p < 0.001), whereas it showed a negative and significant correlation with workplace violence (r = - 0.199, p < 0.001). Professional identity partially mediates the relationship between humanistic leadership and nurse interns’ workplace violence (β = – 0.04, p = 0.01, 95% CI [– 0.079, –0.008]). Likewise, professional identity partially mediates the effect of humanistic leadership on caring behavior among nurse interns (β = 0.33, p = 0.001, 95% CI [0.265, 0.401]).
Conclusions
Humanistic leadership is associated with a supportive and safe work environment for nurse interns. Additionally, by strengthening professional identity, humanistic leadership is associated negatively with workplace violence and positively with caring behaviors.
Introduction
Violence against healthcare workers is a well-documented and widespread problem. The World Health Organization (WHO) defined violence as the intentional use of physical force or power, whether threatened or actual, against oneself or others, which results in or has a high likelihood of resulting in injury, psychological harm, or deprivation (World Health Organization [WHO], 2002). Within healthcare settings, workplace violence represents a complex and multifaceted phenomenon, with healthcare workers frequently exposed to aggression from patients and visitors at various stages of their careers (Liu et al., 2019).
Workplace violence in healthcare extends beyond physical acts to include psychological forms that often precede or accompany overt aggression. These behaviors may begin with subtle forms of harassment and escalate into more severe manifestations such as verbal abuse, intimidation, humiliation, and social or professional exclusion. Importantly, violence occurs across hierarchical levels, including interactions between senior and junior nurses as well as among peers, reflecting the presence of both external (patient or visitor related) and internal (worker to worker) sources of aggression (Pariona-Cabrera et al., 2020).
In this context, bullying, lateral violence, and incivility are recognized as interconnected forms of internal workplace violence. Evidence suggests that such negative interactions are influenced by multiple antecedents, including organizational factors (e.g., leadership style, workplace culture, and resource availability), work-related stressors (e.g., workload and staffing issues), and individual characteristics (e.g., interpersonal and emotional skills). In some cases, these behaviors may become normalized within the work environment, reflecting a form of organizationally tolerated hostility that perpetuates dysfunctional professional norms (Chirico et al., 2022).
Exposure to workplace violence has substantial implications for both individuals and the organization. At the individual level, healthcare workers may experience physical injuries, psychological trauma, emotional distress, and long-term mental health problems. At the organizational level, exposure to violence has been associated with decreased staff morale, reduced teamwork, increased absenteeism and turnover, and the development of a toxic work climate. Collectively, these effects compromise both staff well-being and the quality of patient care (Liu et al., 2019).
Given these consequences, nurse leaders play a pivotal role in mitigating workplace violence and fostering a positive work environment (Saleh et al., 2026). Effective leadership involves establishing a culture of respect, implementing clear policies, and empowering staff to report and manage incidents of violence. However, evidence suggested that although nurse leaders may be aware of bullying and lateral violence, they often lack the strategies or confidence to address these challenges effectively (Vessey & Williams, 2020).
In response to these challenges, humanistic leadership has emerged as a promising approach. This leadership style emphasizes empathy, ethical decision-making, and employee well-being, focusing on personal and professional growth while fostering a purpose-driven and inclusive work culture. Leaders who adopt those behaviors foster positive climates, encourage open communication, and demonstrate respect can influence workplace dynamics and mitigate the risk of violence (Fu et al., 2020).
Moreover, different forms of workplace violence may arise from distinct underlying factors, requiring tailored leadership responses. For instance, patient/visitor aggression often stems from stress, frustration, or illness-related conditions, whereas lateral violence and bullying among colleagues are more closely linked to team dynamics and organizational culture. In contrast, organizationally tolerated hostility may emerge from weak management oversight or ineffective policy enforcement. Humanistic leadership can address these challenges by promoting accountability, strengthening communication, and fostering a culture of fairness and respect (Pompeii et al., 2020; Spector et al., 2014).
Nursing interns represent a particularly vulnerable group within healthcare settings. Previous studies have shown that approximately 17%–53.2% of nursing interns experience adverse nursing safety events, although most incidents go unreported (Stevanin et al., 2018). Despite this risk, a considerable proportion of interns receive limited training on how to prevent or cope with workplace violence (Yang et al., 2023). Nurse interns in Egypt are graduates of a Bachelor of Science in Nursing (BSN) program. They complete four academic years of theoretical and clinical coursework followed by a one-year (12-month) internship across diverse clinical settings, including medical-surgical, pediatric, maternal-newborn, and critical care units. This period is critical for developing the competencies required for professional practice (Akeel & Kabeel, 2023).
Despite growing awareness, little is known about how humanistic leadership is associated with violence and caring behavior among nursing interns, particularly through the lens of professional identity. Evidence suggests that repeated exposure to workplace violence can weaken interns’ professional identities and compromise safe practices, according to evidence (Yang et al., 2023). Conversely, humanistic leadership has been associated with stronger professional identity and improved caring behaviors (Wang et al., 2023).
Workplace violence may undermine interns’ sense of purpose, belonging, and alignment with professional values, leading to reduced caring behaviors (Abdel-Sattar et al., 2020). In contrast, humanistic leadership may buffer these negative impacts by promoting professional identity, thereby encouraging caring behaviors even in challenging or stressful situations (Saleh et al., 2024). Previous research has demonstrated that exposure to violence can significantly impair nursing students’ professional self-concept, with long-term implications for performance and career development (Ata et al., 2024; Yang et al., 2023). Addressing these dynamics is critical for enhancing leadership, strengthening professional formation, and improving both staff wellbeing and patient care outcomes (Saleh, 2018; Saleh et al., 2021).
Although prior studies have explored the relationship between workplace violence and professional identity, as well as the relationship between professional identity and caring behaviors, most have focused on experienced nurses rather than nurse interns (Chang et al., 2023; Saleh et al., 2025a; Yang et al., 2023). Consequently, the role of humanistic leadership in shaping these relationships, especially among nurse interns, remains insufficiently understood, particularly regarding the potential mediating effect of professional identity. To address this gap, the present study aimed to examine the role of humanistic leadership in workplace violence and caring behavior among nurse interns through the mediating effect of professional identity.
Review of Literature
This study is grounded in humanistic leadership and professional identity theories. Both theories have been increasingly applied in nursing and healthcare studies to explain how self-concept and leadership behaviors affect caring behaviors and professional outcomes. Humanistic leadership, rooted in humanistic psychology (Rogers, 1995), emphasizes ethical concern, empathy, and recognition of the inherent worth of each individual. According to recent research, nurses’ professional identities are favorably predicted by humanistic leadership, with psychological security acting as a mediating factor in this relationship (Wang et al., 2023). Evidence supports that this leadership style demonstrates links to improved staff well-being, reduced workplace violence, and improved work engagement (Fu et al., 2020; Pompeii et al., 2020; Spector et al., 2014). The social identity framework (Ashforth & Mael, 1989) suggests that individuals find motivation and purpose in their work, which affects behavior and stress tolerance. It has been found that, in nursing settings, professional identity mediates the effects of the work environment on burnout and caring behavior (Wang et al., 2024; Yang et al., 2023).
Workplace violence is conceptualized broadly to include nonphysical forms of violence, particularly verbal abuse, bullying, intimidation, and hostile behaviors encountered by nurse interns within clinical settings, humanistic leadership is a values based approach that centers on human dignity, ethical responsibility, and relational engagement in guiding organizations and people, are believed to reduce the occurrence and impact of workplace violence (Yang et al., 2023). International studies indicate that healthcare organizations with supportive leadership reported lower rates of bullying and physical aggression, higher perceptions of fairness and organizational justice, and enhanced professional commitment (Pompeii et al., 2020; Spector et al., 2014). Research indicates that workplaces led by leaders who genuinely care about their employees’ well-being have fewer reports of bullying and higher perceptions of organizational justice, which then enhance employees’ commitment and pride. Nurse interns are particularly receptive to these leadership cues because their professional identities are still forming. When leaders actively validate interns’ responsibilities, they are more motivated to care for others and less likely to accept negative behaviors as simply “part of the job” (Wang et al., 2024; Zhu et al., 2022).
Hypotheses
Based on the foregoing literature and theoretical deliberations, this study proposed the following hypotheses: 1. H1: Humanistic leadership is negatively associated with workplace violence and positively associated with caring behavior among nurse interns. 2. H2: Humanistic leadership is positively associated with the professional identity of nurse interns. 3. H3: Nursing professional identity mediates the relationship between humanistic leadership and both nurse interns’ workplace violence and caring behavior
Methods
Study Design
The existing study employed a correlational cross-sectional design conducted across multiple healthcare locations from the end of March to the end of May 2025. The study was designed and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to ensure methodological precision and transparency. This methodological approach was deemed appropriate as it allows for the examination of relationships among variables at a single point in time without experimental manipulation. Moreover, it provides a practical and cost-effective means of exploring naturally occurring associations within real-world nursing contexts (Flanagan & Beck, 2024).
Study Setting
The current study was carried out at two university hospitals affiliated with major Egyptian governorates, namely Mansoura and Zagazig. These sites were chosen for their comprehensive nursing internship programs, diverse clinical settings, and institutional cooperation. Both universities simplified access to nurse interns, confirming a smooth and efficient data collection process.
Sample
The study included nurse interns from the academic year 2024–2025 at Mansoura and Zagazig University Hospitals, a total enrollment of 1912 interns. To estimate the necessary sample size, the researchers utilized an online sample size calculator at https://www.calculator.net/sample-size-calculator.html, based on an estimated maximum population of 1912 nurse interns across the two governorates. With a 95% confidence interval, 5% margin of error, and 50% population proportion, the minimum required sample size was calculated to be 980 nurse interns. To account for possible attrition and non-responses, the sample size was increased to 1250, yielding 1170 valid responses. This escalation confirmed that, even after accounting for probable dropouts and incomplete questionnaires, the study would maintain the appropriate statistical power and confidence levels. The ultimate distribution of interns incorporated 388 nurse interns from Zagazig University Hospitals and 782 nurse interns from Mansoura. University Hospitals, bringing the total final sample to 1170 participants.
Inclusion Criteria
Eligible contributors had to be currently enrolled in the internship program and to have provided voluntary electronic informed consent to participate in the study. They should actively participate in hands-on patient care and clinical rotations in hospitals, have completed 3–6 months of the internship program to ensure familiarity with leadership style and professional identity, and express a voluntary desire to participate in the study.
Exclusion Criteria
Nurse interns not yet involved in clinical rotations or direct patient care, and interns who were on leave or with less than 3 months of internship experience were excluded because they might not have sufficient clinical exposure relevant to the study variables.
Sampling Technique
A nonprobability quota sampling method was utilized, with quotas proportionally allocated according to the number of nurse interns in each hospital, based on the latest official statistics. Applicants were chosen based on their availability, accessibility, and willingness to participate in the study across the selected hospitals, consistent with the definition of non-probability sampling provided by Boswell and Cannon (2022). This scheme was selected for its practicality, enabling the researchers to proficiently access a considerable number of nurse interns during their planned clinical training and internship activities, however, confirming balanced representation from each hospital despite logistical and time constraints inherent in clinical settings.
Recruitment Process
Eligible nurse interns were approached during their clinical rotations and informed about the study purpose, procedures, and ethical considerations. Those who met the eligibility criteria received an invitation to participate and were assured that participation was voluntary and confidential. An electronic informed consent was obtained from all participants before data collection.
Instruments Used in the Study
This study utilized four standardized measurement instruments, originally developed in English and subsequently translated into Arabic, in addition to a demographic data section, to collect and analyze the study variables.
Humanistic Leadership Behavior Scale
This scale was originally developed by Song (2018) as part of a master’s thesis conducted in China, to assess nurse leaders’ humanistic leadership behaviors toward nurses as evaluated by nurse interns. It consists of 26 items covering three dimensions: Work support (13 items), interpersonal communication (8 items), and managerial quality (5 items). Responses are measured using a five-point Likert scale (1=disagree at all, 2=basically disagree, 3=uncertain, 4=basically agree, and 5=fully agree). The items’ scores were summed and allocated by the total number of items to get the mean score, which was then multiplied by 100 to calculate the mean percentage score. The total possible score ranges from 26 to 130, with higher scores indicating higher humanistic leadership behavior displayed by nurse managers to nurse interns.
The original study demonstrated excellent validity and reliability. The internal consistency was high (Cronbach’s α = 0.908; all subscales α > 0.80), Content Validity Index (CVI) was strong (CVI = 0.964) (Wang et al., 2023). In this study, the scale confirmed an excellent reliability, with a Cronbach’s α of 0.97 for the overall scale and from 0.89 to 0.95 for its subscales.
Nurses’ Professional Identity Scale (PIS)
This scale was originally developed by Liu et al. (2011) to measure nurses’ professional identity across multiple dimensions. The scale comprises 30 items distributed among five dimensions: Professional cognitive evaluation (9 items), professional social support (6 items), professional social skills (6 items), professional frustration response (6 items), and occupational self-reflection (3 items). The statements were rated on a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), producing a total score between 30 and 150. The items’ scores were summed and allocated by the total number of items to get the mean score, which was then multiplied by 100 to calculate the mean percentage score. Professional identity levels are classified as follows: < 60% specifies a low level, 60%–80% denotes a moderate level, and > 80% designates a high level of professional identity (Pan et al., 2024).
Wang et al. (2023) stated that the PIS for nurses demonstrated strong internal consistency, with a total Cronbach’s α of 0.84 and 0.90 for its subscales. In this study, the scale confirmed an excellent reliability, with a Cronbach’s α of 0.95 for the overall scale and from 0.74 to 0.92 for its subscales.
Workplace Violence Scale
The Workplace Violence in Healthcare (WPVHC) questionnaire was developed and validated by Kumari et al. (2021) to assess various dimensions of workplace violence experienced by healthcare professionals. The instrument consists of 37 items divided into five main domains: Forms of violence (2 items), impact of violent incidents (5 items), reporting of incidents (7 items), and mitigation strategies (11 items), and risk factors (12 items). In this study, the total WPVHC score was used to signify the whole experience of workplace violence, including both actual exposure to violent incidents (forms and impact) and related awareness and management behaviors (reporting, mitigation, and risk factors).
Each domain employs specific Likert-scale response formats to capture detailed information, ranging from five-point scales for violence frequency to three-point scales for assessing impact, reporting attitudes, mitigation strategies, and perceived importance of risk factors. The items’ scores were summed and allocated by the total number of items to get the mean score, which was then multiplied by 100 to calculate the mean percentage score. The total possible score ranges from 37 to 120. Workplace violence exposure levels are classified using the following cut-off points: < 60%, suggesting low exposure, 60%–80% denotes moderate exposure, and > 80% designates high exposure to workplace violence.
Kumari et al. (2021) reported that the WPVHC questionnaire confirmed a strong internal consistency, with a Cronbach’s α of 0.86. The sampling adequacy was established by a Kaiser Meyer Olkin (KMO) value of 0.82 and a significant Bartlett’s test of sphericity (p < 0.01), supporting its construct validity. In this study, the scale confirmed a good reliability, with a Cronbach’s α of 0.85 for the overall scale and from 0.72 to 0.92 for its subscales. For explanatory precision, sensitivity analyses were directed focusing on the forms/impact subscales as the constituent most closely related to direct exposure to violence.
Caring Behavior Inventory (CBI)
The Caring Behaviors Inventory (CBI) was originally developed as a 42-item instrument and later refined by Wu et al. (2006) into a concise 24-item version, known as the CBI-24. This tool evaluates nurses’ caring behaviors across four primary dimensions as follows: Assurance of human presence (8 items), knowledge and skills (5 items), respectful deference to the other (6 items), and positive connectedness (5 items). Each item is rated on a five-point Likert scale ranging from 1 = Never to 5 = Always. The items’ scores were summed and allocated by the total number of items to get the mean score, which was then multiplied by 100 to calculate the mean percentage score. Although the original instrument does not specify cutoff points for categorizing caring behavior levels, several studies have interpreted results using mean-based classifications. For example, Ahmed et al. (2022) considered nurses with mean percent scores ≥ 50% demonstrating a high level of caring behaviors, whereas those scoring < 50% were categorized as exhibiting a lower level of caring behaviors.
The inventory confirmed strong reliability and validity across studies. Previous research reported high internal consistency (Cronbach’s α = 0.95) (Wu et al., 2006) and excellent content validity (CVI = 0.94), with acceptable construct validity (RMSEA = 0.074) (Labrague et al., 2017). In the current study, the overall scale reliability was 0.96, and subscale reliabilities ranged from 0.83 to 0.90.
Demographic Data of Study Participants
Demographic data collected from the participants included age, gender, and marital status.
Validity of the Tools
To ensure that the contributing students, whose native language is Arabic, clearly understood the study instruments, all items were converted into Arabic. The initial translation was reviewed by a panel of seven university professors fluent in both Arabic and English. Subsequently, a second panel of seven bilingual professors conducted a back-translation of the instruments into English. To further establish content and face validity, five nursing professors specializing in nursing administration carefully appraised the instruments, confirming their appropriateness and validity for use in this study.
Pilot Study
A pilot study was carried out to evaluate the clarity and quality of the study materials, the time needed for data collection, and the feasibility, validity, and reliability of the study instruments. It was conducted on 117 nurse interns (10% of the sample size) but was not included in the main study sample. The results indicated that no modifications were necessary, as the instruments were clear and appropriate for use.
Ethical Considerations
Ethical approval was obtained from the Ethics Committee of the Faculty of Nursing, Zagazig University, Egypt (Reference No. 387–25). The first section of the questionnaire outlined the study’s purpose and nature. Informed consent was obtained electronically, secured by participants selecting ‘agree’ before proceeding. They were assured of confidentiality, anonymity, and the voluntary nature of their participation, with no impact on academic standing. All data were stored securely and accessed only by the research team, and the data were used for research purposes only. The study was conducted in accordance with the Helsinki Declaration, and participants were informed (both verbally and in writing) of their right to withdraw at any time without any penalty.
Data Collection
Data for this study were collected using self-reported assessments completed by nursing interns. Before data collection, the necessary ethical approval was obtained. The study’s purpose and instruments were explained to the interns during their initial meeting, conducted either via Google Meet or in person at the hospitals. The principal investigator also sought their cooperation in supporting the data collection process. Using the questionnaire’s URL to fill it out and submit it: https://forms.gle/rZwuje4CsYcQ19FP8, a cover letter attached to the questionnaire clarified the study objectives, emphasized the voluntary nature of participation, and assured respondents of the confidentiality of their responses. The questionnaire’s URL is disseminated via different internship networks such as a hospital’s social media platform. To minimize potential bias and ensure privacy, the data collection process was designed to limit direct interaction between participants and the research team, thereby promoting authentic and unbiased responses. To decrease the possibility of duplicate responses, response to the questionnaire is limited to one response per device, responses were monitored for completeness and incomplete submissions were excluded from the final analysis.
Statistical Design
The data were analyzed using Statistical Package for the Social Sciences (SPSS) Statistics for Windows, Version 27 (IBM Corp., 2020). Before conducting the analyses, the normality of the study variables was evaluated using skewness and kurtosis values (within the acceptable range of ±2), as well as the Shapiro-Wilk test (p > .05), representing no deviation from normality (Kline & Santor, 1999). Consequently, parametric statistical analyses were considered appropriate. Moreover, sampling adequacy was confirmed by a KMO value exceeding 0.90, and the absence of multicollinearity was verified by variance inflation factor (VIF) values below 5 (Hair et al., 2010).
Descriptive statistics summarized the interns’ characteristics and study variables. Group differences in humanistic leadership, professional identity, workplace violence, and caring behavior were examined using independent t-tests and analysis of variance (ANOVA), with effect sizes (Cohen’s d) reported for significant comparisons. Pearson’s correlation was used to assess the strength and direction of relationships between variables.
Analysis of Moment Structures (AMOS) 24 (Arbuckle, 2016) was employed to perform Structural Equation Modeling (SEM) to test the proposed model, allowing for the examination of direct, indirect, and total effects and providing a comprehensive evaluation of mediation effects, while accounting for measurement errors. The model fit was assessed using the key model fit indices against the ideal or the acceptable values, including the Chi-square divided by degrees of freedom (χ2/df), the Comparative Fit Index (CFI), the Tucker–Lewis Index (TLI), the Root Mean Square Error of Approximation (RMSEA), and the Standardized Root Mean Square Residual (SRMR) (Hooper et al., 2008; Hu & Bentler, 1999; Schermelleh-Engel et al., 2003).
A bias-corrected bootstrapping procedure with 5,000 resamples and a 95% confidence interval (CI) was applied to assess the indirect effects. Missing data were minimal (<5%), and the cases with missing values were excluded using list wise deletion. Statistical significance was determined using a two-tailed p-value of < 0.05, while a two-tailed p-value of < 0.01 indicated high statistical significance.
Results of the Study
A total of 1170 nurse interns participated in this study, conforming to a response rate of 93.6%, which supports the representativeness and capability of the final sample. The sample included 388 nurse interns from Zagazig University Hospitals and 782 nurse interns from Mansoura University Hospitals.
Profile of the Intentional Nurse Interns by Demographic Factors and Deviations in the Study Variables (n = 1170)

M= Mean. SD= Standard deviation. T = Independent t-test. P = p-value.
Descriptive Statistics of Workplace Violence Among Nurse Interns (n = 1170)
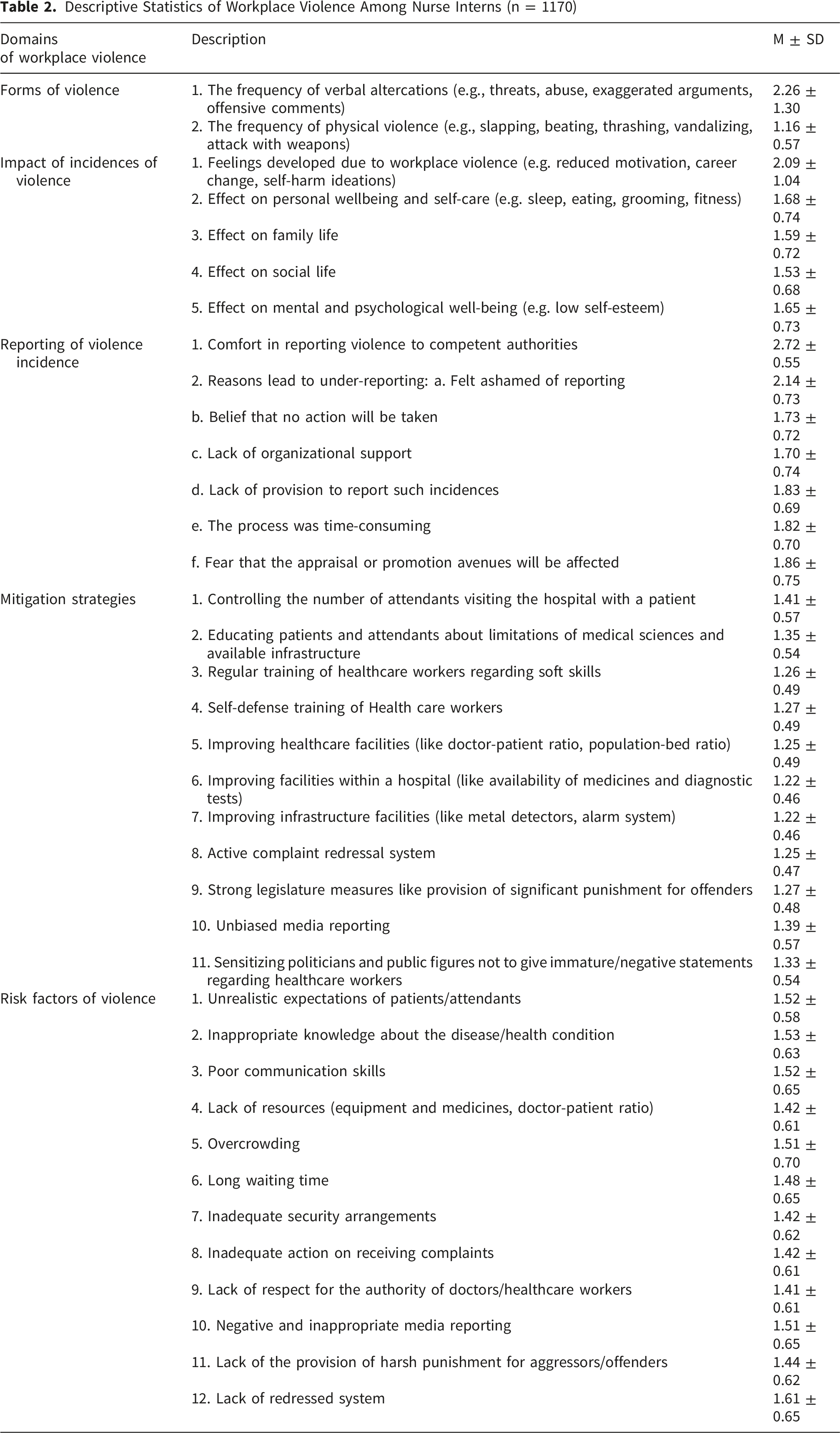
All violence mitigation strategies were considered highly beneficial, with the highest mean scores reported for controlling the number of attendants accompanying patients (M = 1.41), confirming unbiased media reporting (M = 1.39), and educating patients and attendants about the boundaries of medical sciences and available infrastructure (M = 1.35). The most important risk factors identified were the absence of an effective adjusted system (M = 1.61) and insufficient knowledge of disease or health condition (M = 1.53), although lack of respect for the authority of doctors and healthcare workers was observed as the least important risk factor of workplace violence (M = 1.41).
Mean Percent Scores and Cronbach Alpha of Different Study Variables’ as Reported by Studied Nurse Interns (n=1170)

Conversely, workplace violence demonstrated comparatively lower mean percentage scores across its domains, with slight variation between exposure-related dimensions (forms/impact) and response-related (reporting/mitigation/risk factors) dimensions. As shown in the table, nurse interns reported relatively low levels of direct exposure to violent incidents (mean percentage score= 42.7%). In contrast, scores for awareness and management behaviors were comparatively higher (49.8%), reflecting greater engagement in violence-related recognition, reporting, and preventive practices rather than frequent exposure to violent events. The overall workplace violence score (48.1%), therefore, represents a broader violence-related experience, encompassing both exposure and awareness/management behaviors to violence rather than incident frequency alone.
Concerning interns’ caring behavior, knowledge, and skills recorded the highest mean percentage score (93.4%), whereas positive connectedness had the lowest (89.4%). The total mean percentage score was 92.2%, indicating a high level of caring behaviors among nurse interns.
Correlation Matrix of the Key Study Variables (n = 1170)

r=Pearson correlation.
Similarly, nurse interns’ professional identity was significantly and negatively connected moderately with workplace violence (r = – 0.388, p < 0.001), although viewing a large significant positive link with caring behavior (r = 0.527, p < 0.001). This suggests that promoting professional identity not only shelters against violence behaviors but also enriches the quality of care provided. Additionally, workplace violence displayed a medium-significant negative correlation with nurse interns’ caring behavior (r = – 0.399, p < 0.001). This denotes that exposure to aggressive or unsafe surroundings can weaken nurse interns’ capability to deliver compassionate and patient-centered care.
Direct, Indirect, and Mediated Effects (n = 1170)

BC= Biased-corrected percentile method.CI = Confidence interval.

Pathway model elucidating the mediating role of professional identity in the relationship between the humanistic leadership and both workplace violence and caring behavior among nurse interns (n = 1170)
Concerning the mediation analysis, the indirect effect of humanistic leadership on nurse interns’ workplace violence via professional identity was significant (β = – 0.04, p = 0.01, 95% CI [– 0.079, –0.008]), signifying that professional identity partially mediates this relationship. In the same way, the indirect effect of humanistic leadership on nurse interns’ caring behavior through professional identity was also significant (β = 0.33, p = 0.001, 95% CI [0.265, 0.401]), proposing that professional identity partially mediates the effect of humanistic leadership on caring behavior. In general, the total effects determine that humanistic leadership is significantly negatively associated with workplace violence (total β = – 0.15, p = 0.01) and associated positively with caring behavior (total β = 0.41, p = 0.01), emphasizing that the professional identity is a mediator in these relationships.
Supplementary Sensitivity Analysis: The Actual Exposure to Violent Incidents
To address concerns about construct specificity, a sensitivity analysis concentrated on the actual exposure to violent incidents, signified by the forms and impact subscales (7 items). Humanistic leadership was displayed as the independent variable, professional identity as the mediator, and the actual exposure as the dependent variable.
Results (Supplementary Table s2) Confirmed Robustness of the Main Findings
• Direct effect of humanistic leadership to the actual exposure to violent incidents β = −0.08, 95% CI [−0.098, −0.068], p < 0.001 • Indirect effect of humanistic leadership to the actual exposure to violent incidents via professional identity: β = −0.075, 95% CI [−0.101, −0.051], p < 0.001 • Total effect of humanistic leadership to the actual exposure to violent incidents: β = −0.155, 95% CI [−0.182, −0.130], p < 0.001
These results specify that humanistic leadership remains associated negatively with the actual exposure to violent incidents, and the mediating role of professional identity is conserved, compatible with the main analysis using the full workplace violence score.
Goodness of Fit Indices for Structural Equation Modeling Analysis (n = 1170)

Abbreviations: χ2/df = Chi-square/degrees of freedom; CFI= Comparative Fit Index; TLI = Tucker-Lewis Index; RMSEA = The Root Mean Square Error of Approximation; SRMR = The Standardized Root Mean Square Residual.
Discussion
The revolution of medical models has enhanced the association of nursing work, stimulating a shift concerning more humanized and high-quality nursing amenities. Human-centered leadership in health care has developed as a contemporary theory; some might even describe it as a movement, whose time has come. This leadership approach emphasizes the importance of fostering work environments free from bullying, harassment, and threatening behaviors, thereby promoting psychological safety and mutual respect among health care professionals. However, the phenomenon of nursing leadership as a social process, rooted in human interactions within complex micro/macro systems, remains insufficiently documented and explored in the existing literature (Leclerc et al., 2021).
Humanistic Leadership as Regards Workplace Violence and Caring Behavior Among Nurse Interns
This study found that humanistic leadership was negatively associated with workplace violence and positively associated with nurse interns’ caring behavior. These findings indicate that higher levels of perceived humanistic leadership are associated with lower levels of workplace violence and higher levels of caring behaviors among nurse interns. Furthermore, leadership grounded in empathy, respect, and concern for human well-being was associated with psychologically safer work environments. Such environments are, in turn, linked to reduced stress, frustration, and perceived injustice, which are commonly considered precursors of violent behavior. On the other hand, humanistic leadership inspires interns to internalize these values and express them through empathetic patient-centered care.
In agreement with previous studies, Navarro et al. (2022) reported that authentic leadership was associated with lower levels of workplace violence, bullying, and discrimination among nurses. Similarly, Cao et al. (2023) found that change-oriented, relational-oriented, and values-based leadership styles were negatively associated with workplace aggression. Comparable findings were reported by Zhang et al. (2023), who found a positive correlation between authentic leadership and nurses’ caring behaviors. Likewise, Chen et al. (2024) identified a positive relationship between inclusive leadership and caring behavior. In addition, Dehghani-Tafti et al. (2022) demonstrated a positive correlation between ethical leadership and caring behavior. Recently, Saleh et al. (2025b) reported that entrepreneurial leadership was positively associated with nurse interns’ clinical performance.
Humanistic Leadership and Professional Identity of Nurse Interns
The present findings revealed that humanistic leadership was positively associated with nurse interns’ professional identity. This association may be explained by the fact that the ethically oriented characteristics of humanistic leadership are linked to personal growth and a stronger sense of belonging to the profession.
According to Wang et al. (2023) and Haina et al. (2025), humanistic leadership is positively related to nurses’ professional identity. Similarly, Wu et al. (2025) found a positive correlation between inclusive leadership and professional identity. Moreover, the present findings align with prior research emphasizing the pivotal role of leadership in shaping and sustaining nurses’ professional identity; Phillips and Priddy (2023) suggested that supportive leadership is associated with professional identity development. Likewise, Joseph et al. (2021) reported that leadership practices like role modeling, supportive practice environments, and encouragement of lifelong learning are associated with professional identity.
The Mediating Role of Professional Identity
The findings demonstrated that professional identity played a mediating role in the relationship between humanistic leadership and both workplace violence and caring behaviors. Specifically, professional identity partially mediated the association between humanistic leadership and workplace violence, suggesting that higher levels of humanistic leadership are linked to stronger professional identity, which is, in turn, associated with lower levels of perceived workplace violence. Similarly, professional identity partially mediated the relationship between humanistic leadership and caring behavior, indicating that humanistic leadership is associated with caring behavior both directly and indirectly through professional identity.
These findings are supported by Xu et al. (2023), who suggested that leadership associated with stronger professional identity may be linked to lower levels of lateral violence. Additionally, Yang et al. (2023) found that workplace violence was associated with patient safety through its relationship with professional identity and burnout. Furthermore, Wang et al. (2024) reported that professional identity partially mediated the relationship between work environment and caring behavior. Similarly, Wu et al. (2025) found that professional identity mediated the relationship between inclusive leadership and burnout.
Overall, these findings suggest an observable association between humanistic leadership, professional identity, and behavioral outcomes. Humanistic leadership was positively associated with professional identity and caring behavior but negatively linked to workplace violence.
Strengths, Limitations, and Future Research
This study enhances the understanding of leadership in nursing by emphasizing the importance of humanistic leadership in creating a supportive environment for nurse interns. It identifies professional identity as a protective factor against workplace violence and a promoter of positive caring behaviors. The research empirically investigates how professional identity mediates the effects of humanistic leadership on workplace violence and caring behaviors among nurse interns, contributing to leadership and nursing education literature. Limitations include potential biases from self-reported data, restricted sample generalizability, and contextual uniqueness at the study sites. Future research should consider longitudinal and multi-center designs and explore factors like organizational culture and stress management for a deeper analysis of these dynamics.
Implications for Nursing Practice and Research
The study emphasizes the importance of humanistic leadership in nursing to mitigate workplace violence and foster compassion among nursing interns. Nurse leaders should embody respect and empathy to cultivate safer clinical environments. Incorporating humanistic leadership training into development programs is suggested for equipping leaders to advocate for staff. Furthermore, nursing education can enhance interns’ professional values and resilience through mentorship and structured activities. Healthcare organizations are encouraged to prioritize humanistic attitudes and safety measures in their policies. Future research should investigate the effectiveness of these interventions across diverse clinical settings and their impact on interns’ professional identity and patient care outcomes.
Conclusions
This study emphasizes the importance of humanistic leadership in creating a positive clinical environment for nurse interns. Key findings indicate that such leadership is significantly associated negatively with workplace violence and positively with caring behavior, with professional identity acting as a mediating factor. Nurse interns who view their leaders as empathetic and supportive develop a stronger professional identity, leading to enhanced caring behavior and resilience. The results call for healthcare organizations to adopt humanistic leadership in training, focusing on emotional intelligence and mentorship to foster a compassionate nursing workforce and reduce violence.
Supplemental Material
Supplemental Material - The Role of Humanistic Leadership in Workplace Violence and Caring Behavior Through the Mediating Effect of Professional Identity Among Nurse Interns: A Structural Equation Modeling
Supplemental Material for The Role of Humanistic Leadership in Workplace Violence and Caring Behavior Through the Mediating Effect of Professional Identity Among Nurse Interns: A Structural Equation Modeling by Aisha ElSayed-ElAraby Abdelwahid, Manal Saleh Moustafa Saleh, Azza Abdeldayem Ata, Faisal Khalaf Alanazi, Ashraf Amin Eltahan, and Hanan El said Elsabahy in Sage Open Nursing.
Supplemental Material
Supplemental Material - The Role of Humanistic Leadership in Workplace Violence and Caring Behavior Through the Mediating Effect of Professional Identity Among Nurse Interns: A Structural Equation Modeling
Supplemental Material for The Role of Humanistic Leadership in Workplace Violence and Caring Behavior Through the Mediating Effect of Professional Identity Among Nurse Interns: A Structural Equation Modeling by Aisha ElSayed-ElAraby Abdelwahid, Manal Saleh Moustafa Saleh, Azza Abdeldayem Ata, Faisal Khalaf Alanazi, Ashraf Amin Eltahan, and Hanan El said Elsabahy in Sage Open Nursing.
Footnotes
Acknowledgements
The researchers gratefully acknowledge all nurse interns who participated in this research.
Ethical Considerations
Ethical approval was obtained from the Ethics Committee of the Faculty of Nursing, Zagazig University, Egypt (Reference No. 387–25). The first section of the questionnaire outlined the study’s purpose and nature. Informed consent was secured by participants selecting ‘agree’ before proceeding.
Consent to Participate
They were assured of confidentiality, anonymity, and the voluntary nature of their participation, with no impact on academic standing. The process adhered to the Helsinki Declaration, and participants were informed (both verbally and in writing) of their right to withdraw at any time.
Author Contributions
Made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; AA, MS, AA, HE.
Involved in drafting the manuscript or revising it critically for important intellectual content; AA, MS, AA, HE.
Given final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content; AA, MS, AA, HE, FA, AE.
Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. AA, MS, AA,HE,FA,AE.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be available from the corresponding author on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.