
Abstract
Background
The right to choose a mode of delivery is an essential aspect of compassionate and respectful care that promotes both maternal and neonatal health, as ignoring the mother’s preferences heightens the risk of postpartum depression and post-traumatic stress. This study utilized the Health Belief Model as a theoretical foundation for understanding pregnant women’s beliefs regarding their preferred mode of birth and its associated factors.
Objective
This study aimed to assess birth mode preferences and associated factors among Jordanian pregnant women.
Method
A cross-sectional study was conducted in northern Jordan from March to May 2025. The respondents were recruited by convenience sampling. The data was collected through online-administered questionnaire utilizing a valid and reliable instrument, which was based on the five core domains of the Health Belief Model. The data analysis was preformed through SPSS software (Version 28).
Results
The total number of participating pregnant women in this study was 330. 23.4% of the respondents preferred cesarean section and 76.4% preferred vaginal delivery. Women who preferred cesarean section had higher mean scores for perceived benefits, lower mean scores for perceived susceptibility and severity of cesarean section compared to those who preferred vaginal delivery. Predictors of CS preference included age (OR = 3.203, p = 0.000), economic status (OR = 8.250, p = 0.00), previous type of birth (OR = 2.570, p = 0.000), complications in previous birth (OR = .172, p = .042), parity (OR = -.795, p = 0.042) and hospital type planned for birth (OR = 1.692, p = 0.013).
Conclusion
Women often prefer the mode of birth which they perceive to have benefits that outweigh potential risks and complications. Therefore, maternity health care institutions should develop antenatal education programs based on the Health Belief Model about the benefits, risks and complications of both modes of birth.
Introduction
Except in situations where medical complications require a cesarean section (CS), a normal vaginal delivery (VD) has historically been thought to be the safest and most appropriate method of childbirth. Prematurity, fetal distress, malpresentation, cephalopelvic disproportion, multiple pregnancies, maternal health conditions, and failure to progress during labor are some examples of complications requiring a cesarean section (Dhakal-Rai et al., 2021). However, the number of CS births has increased dramatically in recent years, sometimes due to maternal preference and frequently without a clear clinical indication.
The rates of CS have increased significantly worldwide exceeding the recommended CS rate of 10-15% set by World Health Organization (WHO) (WHO, 2015). For instance, according to trend analysis review research included 158 countries; the global rate of CS births was 21% (Betran et al., 2021). In the Middle East, the CS rate in Egypt increased from 52% in 2014 to 72.2% in 2021. Furthermore, the rates of CS were 35 % in Saudi Arabia in 2023 and 33.2% in Iraq in 2018 (MOHP, 2014; World Population Review, 2025). In comparison with VD, planned CS is associated with an increased risk of maternal and newborn complications, including wound infection, urinary tract infection, deep vein thrombosis, post-partum hemorrhage, uterine adhesions, rupture of uterine scar, neonatal respiratory distress, meconium aspiration, and neonatal death (Dahlquist et al., 2022; Keag et al., 2018).
Obstetricians and other medical professionals respect pregnant women’s right to select the birth method of their choice (Mascarenhas Silva et al., 2024). A woman’s personal beliefs regarding various birth modes frequently impact her decision (Preis et al., 2019). These beliefs differ from one person to another and are impacted by cultural, social, emotional, and environmental factors (Abraham & Sheeran, 2015). A popular conceptual framework for comprehending how people base their health-related decisions on their belief patterns is the Health Belief Model (HBM). This model states that people are more likely to take a particular health action or make a certain decision if they believe the potential benefits of that action (perceived benefits) outweigh the potential drawbacks (perceived barriers) and that they are susceptible to a given condition (perceived susceptibility) and complications (perceived severity). Also, external motivation, such as experience, social influence, and medical advice, can influence decision-making (cues to action) (Abraham & Sheeran, 2015).
In Jordan, the rate of CS has increased significantly in recent decades. It increased from 22.9% in 2010 to 42.8% in 2023 (HPC, 2024). A retrospective study conducted in a major university teaching hospital in Amman indicated that 22.78% of all births in 2022 were cesarean sections performed based on the mother’s request (Fram et al., 2023). Maternal request has been reported as one of the most common reasons for cesarean birth without clinical indication (Al-Rawashdeh et al., 2022).
A study conducted in Jordan surveyed 1,005 women who had previous history of at least one CS. Approximately 53% of respondents reported their reason for choosing CS was fear of labor pain (Abuhammad et al., 2021). Additionally, more than half of participated women believed that CS do not harm infants, and do not cause any potential risks for mothers. The main source through which they acquired information were reported to be the internet (36.2%), and personal networks such as family and friends (31.6%) (Abuhammad et al., 2021).
A national retrospective study conducted between 2017 and 2018, surveying 6,525 women, found that CS rates were prominently higher among women aged 40 years and older, as well as in private healthcare settings (Al-Rawashdeh et al., 2022). However, this increasing trend in CS rates highlights the need to explore pregnant women’s beliefs which shape their choice regarding their preferred mode of birth. The findings of this study will provide insight to government, health care system, and health care providers to adopt strategies that are effective in overcoming the problems which contribute to the increasing rates of CS. In Jordan, the literature on the preferred mode of birth and its associated factors among pregnant women is scarce. Therefore, this study aimed to assess birth mode preferences and associated factors among Jordanian pregnant women.
Specific Aims
1. Estimate the prevalence of pregnant women who prefer vaginal birth versus cesarean section. 2. Compare beliefs of women in the two groups regarding modes of birth based on the health belief model domains. 3. Determine predictors of preferred mode of birth based on socio-demographic and obstetric characteristics.
Review of Literature
There are various factors influencing women’s preference for the delivery method. For instance, 68% of pregnant women in a cross-sectional descriptive study in Pakistan using convenience sampling preferred VD. Such preference was attributed by 58.4% to a fast recovery, 22% due to less postpartum pain, and 20% due to a lower risk of complications, for both the mother and newborn (Khan et al., 2023). However, 32% of respondents said that they preferred CS, 40% were afraid of labor pain, 20% believed that CS would be safer for the baby, and 16% had traumatic vaginal birth previously. Increased maternal age, inadequate communication with the physician, unawareness of the risks and complications associated with CS, as well as the existence of pregnancy-associated diseases like diabetes mellitus or hypertension, had a strong association with the choice of CS (Khan et al., 2023). In another Saudi Arabian study, sampled approximately 342 primigravida, women chose CS as the desired birth method primarily due to fears from childbirth. Women reported fears from pain, harm or injury to the baby, lack of control over their body during delivery, fear of the unknown, or lack of decision-making autonomy. The finding of this study indicated that women were more likely to decide CS when they are younger and have high incomes (Elgzar et al., 2023).
Furthermore, pregnant women often prefer a mode of birth that is the same as their previous birth experience (Anaman-Torgbor et al., 2022; Saxena et al., 2019). Women who choose CS often do so due to concerns regarding maintenance of their body shape, following current trends, encouragement by their doctors, or imitating others (Tavassoli & Dizaji, 2021). Further concerns include discomfort with frequent per-vaginal examinations and potential complications of VD, such as urinary incontinence, perineal tears or trauma, and pelvic organ prolapse (Khatony et al., 2019). On the other hand, women who choose VD often considered it a natural process, had a desire to experience each stage of labor, and they had a perception that it fosters early contact between mother and baby, and facilitate early breast feeding (Kalyan et al., 2024).
Additionally, a recent systematic review encompassing 14 studies from East Africa, including 47,561 respondents, revealed the proportion of women who prefer VD was 75% whereas those who prefer CS mode of birth was 25%. Women who had regular antenatal care visits, had a history of previous CS, lived in urban areas, were unemployed, had a higher educational level, and those who had delivered in governmental hospitals were more likely to opt for CS (Taye et al., 2025).
A descriptive cross-sectional study in Egypt using the HBM framework was conducted to determine predictive factors of the preferred mode of birth of 398 women. The results of this study emphasized that perceived severity, perceived benefits and perceived susceptibility had a profound influence on women’s preferences (Darwish et al., 2019). Women who preferred CS perceived themselves at a lower risk of complications such as prolonged recovery period, wound infection, anesthesia complication, and uterine adhesions. Those with the preference for CS overestimated the benefits of cesarean birth, including avoiding labor pain, long labor, frequent discomfort of per vaginal examination, and maintaining the integrity of perineum. Additionally, recommendations from physician, family, and peers influenced some women’s preference for CS (Darwish et al., 2019).
Methods
Study Design
A cross-sectional study was conducted to determine the percentage of pregnant women who chose each mode of birth and the factors affecting their choice of birth mode by using the Health Belief Model. Cross-sectional designs involve investigations that examine data from a population at a certain moment. The implementation of this design is crucial in providing initial evidence for the planning of a subsequent advanced investigation (Wang & Cheng, 2020). Additionally, this design is frequently employed to elucidate health factors and characterize demographic attributes. Furthermore, it is typically cost-effective and straightforward to execute (Wang & Cheng, 2020).
Sample and Sampling Technique
The research utilized a non-probability convenience sampling technique to recruit respondents. This strategy was employed because of its adaptability, cost-effectiveness, and minimal time demands for respondent selection (Golzar et al., 2022). Eligibility criteria for inclusion involved pregnant women living in northern Jordan; able to read and write Arabic, had gestation age between 8 and 40 weeks with a live fetus. On the other hand, women with high-risk pregnancies or medical indications for CS, such as multiple pregnancies, antepartum hemorrhage, preeclampsia, gestational diabetes, or previous two or more cesarean sections were excluded from participation.
The necessary sample size was determined utilizing G*Power software (Version 3.1.9.7; Faul et al., 2009). According to a two-tailed logistic regression analysis, a minimum of 276 individuals was deemed necessary, based on a low to medium odds ratio (2), a conservative probability (0.5), a significance level of (0.05), and a statistical power level of (0.8). A 15% over-sampling method was employed to address incomplete replies, resulting in a total requisite sample size of 330 respondents.
Measures
The study employed questionnaire in collecting data. The survey was designed in two sections. The first part of the instrument collected demographic variables for (age, education level, occupation, income, place of residence, and type of health insurance coverage) and obstetric history including (gravidity, parity, previous modes of birth, planned place of birth, and preferred mode of birth). The second part was adapted from the instrument developed by Loke, Davies, and Li (2015), which was utilized due to alignment with the research objective, and proven validity and reliability. The instrument consists of 47 items to assess the beliefs of pregnant women on both modes of birth (21 for VD and 26 for CS). These items were developed based on the five core domains of the HBM, including perceived susceptibility, perceived benefits, perceived severity, perceived barriers, and cues to action. Responses were measured on a 4-point Likert scale from 1 (strongly disagree) to 4 (strongly agree), the scores for all items of each core domain was calculated, and the higher scores suggested a stronger belief (Loke et al., 2015).
The instrument has a strong psychometric properties, a content validity index (CVI) of 0.94, and high internal consistency, as indicated using Cronbach’s alpha coefficient of 0.89 (Loke et al., 2015). The instrument was translated to Arabic and then back to English by two linguists to ensure content validity. A pilot test of 30 respondents resulted in acceptable internal consistency and reliability using Cronbach α = 0.74 for the entire questionnaire.
Data Collection
Data collection commenced subsequent to clearance from the Institutional Review Board (IRB) of (X institution). A convenient sampling technique was employed to attract potential respondents based on their availability and willingness to engage in the study. Women were approached while entering or exiting selected public and private hospitals in northern Jordan to receive antenatal care. The data was collected over two months from March to May, 2025.
The study instrument consisted of an online-administered questionnaire. Demographic information and the primary data from the questionnaire were gathered. The data was gathered utilizing Google Forms, followed by exportation as an Excel file. The researchers supplied a Google Form link that included the questionnaire to the study respondents who fulfilled the inclusion criteria via social media (WhatsApp and email). The first page provided the respondents detailed information about the purposes and significance of the study, the expected time to fill the questionnaire (10 -15 min), and their right to withdraw from the study at any time without any penalty. Additionally, the email address of the researcher was included on this page to answer any additional inquiries. The prepared Google form was anonymous; thus, it did not include any personal information about the respondents. Also, to maintain respondent confidentiality, the data acquired from the questionnaires was encoded, and only the researchers were authorized to access it. Ultimately, the data was safely saved on a computer that necessitated a password for entry.
Ethical Consideration
Permission for data collection was obtained from the Research Ethics Committee of (institution name with reference number retracted), which follows Helsinki guidelines. The researchers provided the respondents full description about the methodology and purposes of the study, ensured the confidentiality, anonymity, and voluntary participation.
Data Analysis
Statistical Package for the Social Sciences (SPSS; version 28) was utilized to analyze the data. Descriptive statistics were used to identify and compare demographic and obstetric information between the two groups of respondents (those who preferred VD versus CS). Inferential statistics using chi-square test (χ2) was applied to explore the associations between women perception regarding modes of birth (VD and CS) and their preferred modes of birth. In addition, t-test was used to compare the means of perception for the five domains of HBM between the two groups; binary logistic regressions were used to examine important predictors of birthing preference. The regression coefficients and the odds ratios of these coefficients, along with the 95% confidence intervals for each coefficient, were shown alongside the regression results. The adequacy of model fit was determined by the Hosmer-Lemeshow test. A non-significant p value (p > 0.05) suggests that our model fits the data well. For all inferential analyses, a statistical significance was defined as p < 0.05 a priori.
Results
Socio-Demographic Characteristics of Respondents
A total of 330 pregnant women participated in this study. Approximately half of the respondents were 26-35 years old (n=163, 49.4%). Most of the respondents attained a secondary level of education, held diploma or baccalaureate degree (n=152, 46.1%, n= 138, 41.8%) respectively. The vast majority of respondents (n=254, 77%) were homemakers and (n= 201, 60.9%) received between 400 and 800 JOD monthly. Also, nearly 53.6% of respondents live in urban area (n=177) and 51.8% have governmental insurance (n=171). Moreover, most of the respondents were gravida two, para one (n=163, 49.4%), in third trimester (n=198, 60%), had VD in previous pregnancies (n=202, 61.2%), did not report any complications in previous births (n=279, 84.5%), planned to birth in governmental hospitals (n= 236, 71.5%). Overall, approximately 76.4% of pregnant women reported preference for VD mode of birth (N=252) while 23.4% preferred CS (N=78).
Socio-Demographic Characteristics of Respondents (n=330)

Notes: n: Sample Size; %: Percentage; VD: Vaginal Delivery; CS: Caesarean Section; JD: Jordan Dinar; BSC: Bachelor of Science; NVD: Normal Vaginal Delivery.
*: Significant p ≤ 0.05.
Perception of Pregnant Women Towards Vaginal Delivery
Perception of Pregnant Women Toward Vaginal Delivery Using the Health Belief Model (n=330)

Notes: n: Sample Size; %: Percentage; VD: Vaginal Delivery; CS: Caesarean Section.
*: Significant p ≤ 0.05.
Meanwhile, there were significant differences between the counter groups in respect to items of perceived severity, barriers, cues to action and preferred mode of birth (p < 0.05). Pregnant women who preferred vaginal delivery had fewer concerns regarding risks of VD. For example, 55.2% of respondents who preferred vaginal mode of birth expressed concerns regarding fetal injuries that may occur while the fetus passes through vaginal canal compared to 75.3% who preferred CS (p=0.000). In addition, only 27.2% of pregnant women who preferred VD have insurance to give birth in private hospitals while 43.6% of those who preferred CS have insurance to give birth in private hospitals (p=0.005). Furthermore, more than two thirds of the respondents who preferred VD revealed that they were recommended to birth vaginally by their doctors (81.8%), friends, and relatives (83.3%) versus 46.2% and 42.3% in the compared group.
Perception of Pregnant Women Toward Cesarean Section
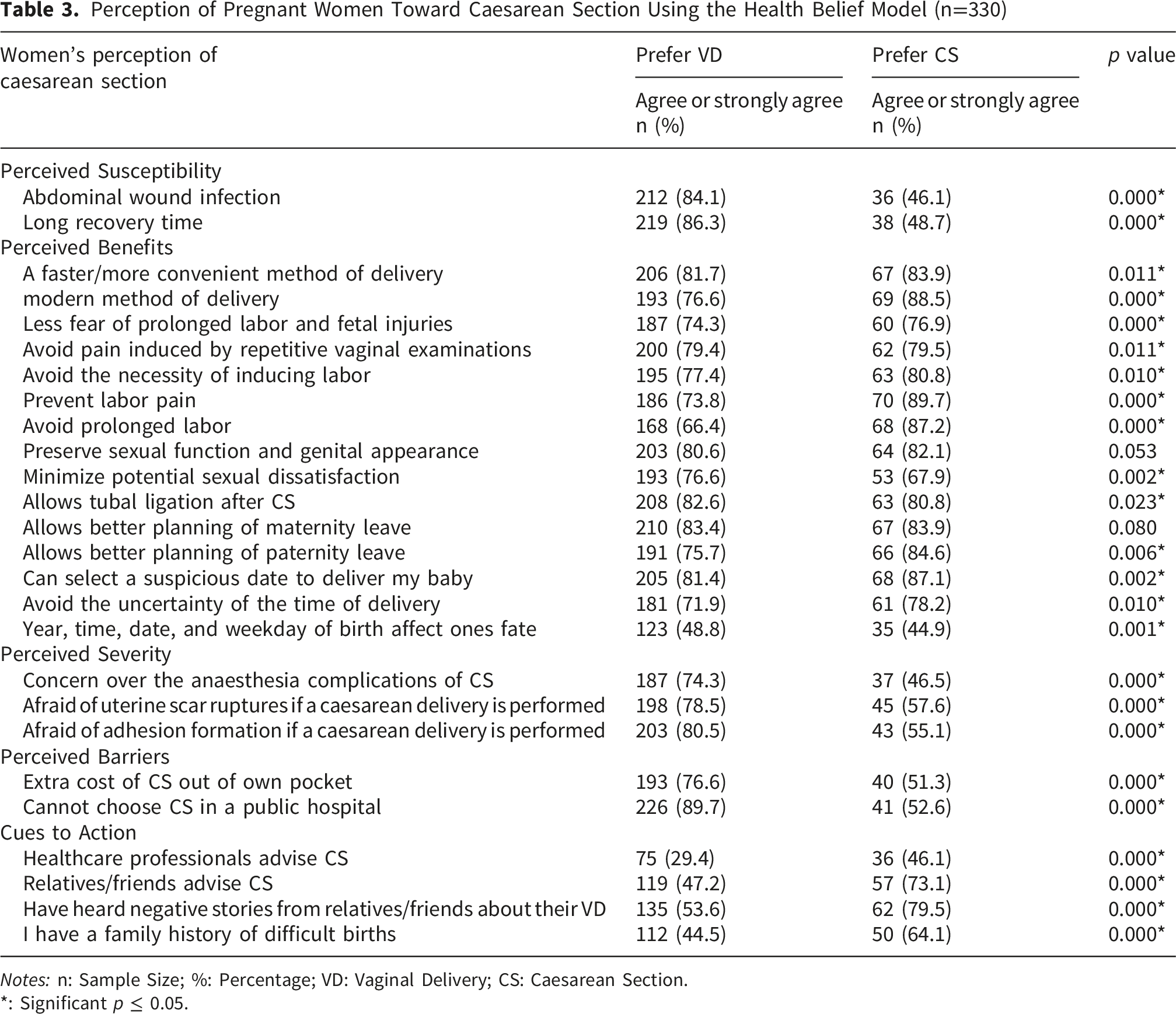
Perception of Pregnant Women Toward Caesarean Section Using the Health Belief Model (n=330)
Notes: n: Sample Size; %: Percentage; VD: Vaginal Delivery; CS: Caesarean Section.
*: Significant p ≤ 0.05.
Comparison of Mean Scores of Health Belief Model Domains Between Women Who Prefer Vaginal Delivery and Caesarean Section (n = 330)

Notes: n: Sample Size; SD: Standard Deviation; VD: Vaginal Delivery; CS: Caesarean Section.
*: Significant p ≤ 0.05.
Significant Predictors for the Preferred Mode of Birth

Notes: B: Unstandardized Regression Coefficient; S. E: Standard Error.
*: Significant p ≤ 0.05; Hosmer and Lemeshow test (chi-square=3.677, p=.885).
Discussion
In this study, almost one-quarter of pregnant women (23.6%) preferred CS as their mode of birth. This rate is in line with similar studies done in neighboring countries. For example, research in Egypt among 537 pregnant women in Egypt showed that 21% of respondents preferred CS (Ibrahim et al., 2021). Likewise, a study performed in Saudi Arabia on 342 nulliparous pregnant women showed that the preference rate of CS was 25.7 % (Elgzar et al., 2023). The estimated rate of CS preference among Jordanian pregnant women in the current study was greater than what was reported in Norway (5%) or Australia (18.4%) (Coates et al., 2020). On the other hand, this was lower than CS preference in Iran (62.5%), Poland (56%), and Pakistan (32%) (Jodzis et al., 2021; Khan et al., 2023; Matinnia et al., 2017). However, these differences may have resulted from variations in social, economic and cultural background between people in different countries.
The findings of the present study revealed that there were significant factors that influenced pregnant women’s preferred mode of birth. Age was one of these factors where for example, older women were more likely to opt for CS. A cross sectional descriptive study in Pakistan among 500 pregnant women revealed that women over the age of 35 years were more likely to choose CS compared to younger individuals. Similarly, findings of a survey conducted in Jordan showed that women over the age of 40 were three times more likely to undergo CS delivery than those under 20 years (khan et al., 2023; Al-Rawashdeh et al., 2022). A study targeting 1617 pregnant women from the United Arab Emirates indicated that women older than 30 years, with history of CS, and working women were more likely to prefer CS birth (Al-Rifai et al., 2020). Conversely, another Ethiopian study revealed that preference for CS was greater among primigravida and younger women (Welay et al., 2021). The interpretation of these differences could be that older women tend to opt for, or are advised to choose, CS by their doctors because they have a higher risk for health related problems associated with pregnancy. Meanwhile, younger women generally tend to fear VD and perceive CS as a safer or less painful option.
Current preferred mode of birth was also significantly influenced by prior delivery method and birth complications. Women who had previously experienced CS or both VD and CS were more likely to have CS during subsequent pregnancies. Moreover, those with previous birth complications had a higher CS preference (30.8%) than those without (10.7%). The findings of this study were consistent with a Jordanian study on 166 pregnant women with previous history of CS, in their third trimester of pregnancy. More than half of these women preferred to give birth by CS rather than VD (Sindiani et al., 2020). Fear of pain associated with labor contractions due to VD and lack of knowledge regarding complications of CS influenced their decision for the preferred mode of birth (Sindiani et al., 2020). In addition, another cross section design study conducted among 222 pregnant Ghanaian women, showed a direct significant relationship between previous mode of birth and preferred method of birth. In particular, 58% of the respondents who had previous VD and 52% of those who had prior CS stated that they preferred the same method as their previous mode of birth (Anaman-Torgbor et al., 2022).
Moreover, having private medical insurance and high income influenced women preference for CS significantly. 20.5% of women who preferred CS had private medical insurance. In addition, 26.9% of women with higher incomes chose CS, while 9.1% of women with lower incomes chose this mode of birth. Similar results were emphasized by an Iranian study sampled of 200 pregnant women to identify the social determinants of CS preference found that employment and higher income increased preference for CS (Tavassoli & Dizaji, 2021). In Jordan, the rate of CS in private hospitals is about 40% higher than governmental ones (Al-Rawashdeh et al., 2022). The ability of women to choose CS without medical reasons, rapid and easily scheduling processes for CS, fear of natural labor pain, excessive caution by obstetricians to avoid complications, in addition to the high fees of CS for the hospital and obstetrician might increase the rate of CS birth in private hospitals (Omani-Samani R et al., 2017).
With respect to perceived susceptibility, approximately 46.8% and 34.9% of women who preferred VD considered themselves at risk for painful labor and postpartum hemorrhage respectively opposed to 93.6% and 69.3% of those who preferred CS. On the other hand, women who chose CS believed themselves to be significantly at lower risk of wound infections (46.1%) and prolonged recovery periods (48.7%) compared to those who chose VD. A descriptive cross sectional study conducted in Saudi Arabia investigating the knowledge and attitudes of 300 pregnant women revealed that 42% of women declared that they experienced more pain during VD compared to CS (Faden et al., 2022). About 82 % reported that post-partum hemorrhage occurred more frequently in VD than in CS. In addition, 65% reported that susceptibility to infection increased after CS (Faden et al., 2022). Across the literature, evidence ranges from quantitative cohort studies to deep qualitative narratives within a wide cultural context, fear of labor pain has been consistently validated as a significant independent predictor of opting for CS (Colomer et al., 2021; Ibrahim et al., 2021; Junge et al., 2021). For instance, a meta synthesis including 52 studies in different and mostly high income countries found that fear of childbirth pain is one of the major factors underlying preference for CS (Colomer et al., 2021).
With regard to perceived benefits, while most respondents acknowledged the advantages of both VD and CS, they were more likely to appreciate the benefits of the childbirth mode which they preferred. For example, 87.3% of women who preferred VD viewed it as a “natural process”, 88.4% believed that it facilitated early contact with the newborn compared to 71.7% and 73.1%, respectively, among those who preferred CS. This is consistent with the results of a descriptive study conducted in Egypt, which reported that the majority of respondents agreed or strongly agreed with the benefits of both VD and CS (Darwish et al., 2019). Perceived benefits are recognized as a significant predictor in the decision-making process regarding the mode of delivery. Women tend to weigh the perceived advantages and risks associated with each birth mode before making their choice. Women who favored CS believed that it was safest for the mother and newborn, better for sexual relationship and genitalia appearance, avoided labor pain, caused less anxiety, allowed control over the time and date of birth, and was considered a modern mode of birth. On the other hand, women who preferred VD believed that it was better for the health of mother and newborn, ensured faster recovery, and was more convenient for breast feeding (Colomer et al., 2021; Shirzad et al., 2021). In addition, Coates et al. (2020) identified perceived benefits related to safety and recovery as key factors influencing women choice of their preferred mode of birth, whether VD or CS.
Regarding perceived severity and barriers, the results of this study suggest that women who preferred CS had significantly more concerns about the disadvantages of VD compared to those who preferred VD. Specifically, 75.3% of them were worried about potential injury to the baby during the birth process, 76.9% of them feared episiotomy and vaginal laceration or tears, and 80.7% were concerned about complications such as urinary incontinence. By comparison, among women who preferred VD, just 55.2%, 55.6% and 56.8% shared the same concerns. By contrast, women who favored VD also reported greater concern regarding anesthesia side effects on the mother and newborn (74.3%), concomitant complications of CS including uterine rupture (78.5%) and uterine adhesions (80.5%). Just 46.5%, 57.6%, and 55.1% of women who preferred CS had these concerns, respectively. Similar results emerged from a systematic review conducted in Iran which included 91 quantitative and qualitative studies which emphasized that women who preferred CS often expressed concerns about negative outcomes and unanticipated complications associated with VD. Moreover, some women expressed worries about losing control over their body during VD (Shirzad et al., 2021). Conversely, those who preferred VD often expressed fears from side effects of anesthesia, and the potential complications of CS (Colomer et al., 2021).
Women who opted for VD as their preferred mode of birth were more likely to consider the cost of CS as a barrier (76.6%) than those who opted for CS (51.3%). This finding aligns with literature stating that the cost of CS also includes the indirect costs of having protracted recovery from CS and negatively impacting women’s ability to fulfill their responsibilities toward their families and children (Binyaruka & Mori, 2021).
With respect to cues to action, information and advice provided by health care providers, family members, relatives and friends played an important role in explaining women’s preference for mode of birth. Similar results were observed in a study conducted in Iran that found a significant direct relationship between physician and midwife encouragement for CS and women’s preference for this mode of birth (Tavassoli & Dizaji, 2021). Notably, findings of Sindiani et al., 2020 study in Jordan showed that about half of pregnant women obtained information about modes of delivery from their doctors, whereas the remaining relied on family, relatives, friends, and media sources. In addition, some women opted for CS to preserve their dignity, influenced by stories shared among relatives or friends who experienced maltreatment during VD (Colomer et al., 2021). Similar results were emphasized by an Iranian study. This study was conducted using experimental design. 426 women were asked to read stories of their peers’ experiences regarding their modes of giving birth It demonstrated that birth preference was significantly influenced by these stories; negative stories regarding VD increased the preference of the respondents for CS, while positive stories about VD significantly increased preference for this mode of birth (Miller & Danoy-Monet, 2021).
Regarding perception for VD, the results of this study pointed out that those who preferred VD had lower mean scores for perceived susceptibility and severity but higher mean scores for cues to action as compared to the counter group. Conversely, regarding perception for CS, women who preferred CS had lower mean scores for perceived susceptibility and severity, but higher mean scores for perceived benefits. These results align with previous studies conducted in Iran and Hong Kong, which identified a significant correlation between pregnant women’s perceptions using the health belief model and their choice for mode of birth. Furthermore, women tended to decide their preferred mode of birth based on their beliefs regarding greater benefits, fewer severity and barriers (Dadipoor et al., 2017; Loke et al., 2015; Safari-Moradabadi et al., 2018).
Implication for Practice
The present study findings provide several valuable implications for practice that can be summarized by integrating antenatal education programs into routine antenatal care to provide pregnant women with evidence-based information about modes of birth. Such programs contribute to shaping women’s beliefs about their preferred mode of birth. Also, health care providers, including obstetricians and midwives, should provide pregnant women with personalized counseling by utilizing effective communication while taking into consideration their beliefs, attitudes, and level of knowledge.
Pregnant women revealed that fear from childbirth contraction pain is one of the main reasons for preferring CS. Therefore, health care providers should provide counseling and psychological support to pregnant women during antenatal care to overcome stress and fear. Since the majority of pregnant women who prefer CS obtain advice from their family and friends, the Ministry of Health should employ social media platforms to improve public knowledge and attitudes toward VD. It should also highlight the potential disadvantages and long-term effects of CS when conducted without medical indications.
Strengths and Limitations
The present study was the first study in Jordan to determine women’s preferred mode of birth and its associated factors utilizing the Health Belief Model framework. However, there are several limitations to this study. First, the current study included a small sample size of 330 respondents enrolled by a convenience sampling method, which may limit the generalization of the findings of this study to a wider population. Also, the cross-sectional design and the use of an online based, self-reported questionnaire increased the risk of social desirability bias and selection bias, which may affect the reliability of the results. Moreover, this study overlooked the effects of religion, culture, and emotion in shaping the preferred mode of birth. Future research using a random sampling method, a larger and more demographically diverse sample could improve generalization and determine the factors that guide decisions toward the preferred modes of birth.
Conclusion
The HBM provided a better understanding for perceptions of pregnant women about their preferred mode of birth. Women prefer certain modes of birth when they perceive their benefits to exceed their risks and severity. The prevalence of pregnant women who preferred CS is higher than the recommended rate by WHO. Age, economic status, previous birth modes, experiences of complications in previous births, and type of hospital planned for birth were significant predictors of the preferred mode of birth.
Footnotes
Acknowledgements
The authors would like to express sincere appreciation for all pregnant women participated in this study.
Ethical Considerations
Permission for data collection was obtained from the Research Ethics Committee of Al-Balqa Applied University (Ref. 61/6/2024/2025).
Consent to Participate
Informed consent was obtained online from each participant. The researchers provided the participants full description about the methodology and purposes of the study, ensured the confidentiality, anonymity, and voluntary participation.
Consent for Publication
This manuscript does not contain any individual person’s data in any form (including individual details as name, images, or videos).
Author Contributions
S. A, F. H, M. A. B, E. A, M. E, and L. H contributed significantly in study conception, designing, and data collection. S. A analyzed the data, F. H and E. A interpreted the results, M. E and L. H revised the manuscript and edited it.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Use of AI Software
No AI software was used in this study.