
Abstract
Introduction
Moral distress among intensive care unit (ICU) nurses is a global concern that affects the quality of care and well-being. In Japan, how hierarchy and consensus culture shape nurses’ experiences and ethical perceptions remain underexplored.
Objectives
This mixed-methods study explored moral distress, how Japanese ICU nurses perceive the ethical climate, and the interrelationship between the two.
Methods
An explanatory sequential design was used. Phase one involved a web-based survey of 168 ICU nurses from 54 facilities, employing the revised Japanese versions of the Moral Distress Scale and the Hospital Ethical Climate Survey. Phase two comprised semi-structured interviews with 11 purposively selected nurses based on quantitative findings, followed by content analysis.
Results
Quantitative analysis showed moderate moral distress, with the highest score for “lack of respect for patient dignity” and significant correlations with longer ICU experience. “Organizational support through clear hospital philosophy” received low ratings and was negatively correlated with distress arising from collaboration difficulties. Qualitative findings expanded on these results by identifying themes of powerlessness over futile treatment, communication challenges in multidisciplinary teams, and dissatisfaction with physician-centered decision-making.
Conclusion
Japanese ICU nurses experienced moderate moral distress, with end-of-life care emerging as a salient context. The distress was associated with the ethical climate, particularly the lack of perceived organizational support. These findings emphasize the need to enhance organizational structures, clarify ethical principles, and foster open interprofessional communication. Future research should use longitudinal designs to examine the effects of structured interventions—such as ethical decision-making support systems—on reducing moral distress and improving the ethical climate in ICUs.
Moral distress—the psychological and emotional turmoil experienced when nurses recognize but cannot carry out what they believe to be ethically correct actions due to institutional, organizational, or interpersonal constraints (Jameton, 1984)—is a critical concern in intensive care settings. Intensive care units (ICUs) are high-stakes environments in which critically ill patients require technologically advanced care and rapid, complex ethical decisions. In these settings, nurses frequently encounter ethically challenging situations such as treatment urgency, lack of patient decision-making capacity, conflicting views within multidisciplinary teams, and resource limitations. Despite their central ethical responsibility to safeguard patients’ dignity and best interests, nurses often find themselves unable to implement the care they believe to be ethically appropriate, resulting in profound psychological and emotional distress. Such distress has been internationally linked to burnout, turnover intentions, and compromised quality of care.
In Japan, this issue may be further influenced by cultural and organizational characteristics unique to the healthcare system. Japanese clinical settings are traditionally characterized by a hierarchical structure in which physicians hold dominant authority, and nurses’ ethical concerns may be subordinated to medical decision-making processes. Additionally, cultural norms that emphasize group harmony (wa) and the avoidance of overt disagreement can limit opportunities for nurses to voice ethical concerns or to challenge decisions they perceive as problematic. These systemic patterns suggest that moral distress in Japanese ICUs may have distinct features compared to Western contexts.
Understanding moral distress in Japan, therefore, requires attention to structural, cultural, and organizational dynamics that influence ethical decision-making. Further, because ethical climate—the shared perception of how ethical issues are recognized and addressed within an organization—plays a key role in shaping nurses’ ethical experiences, examining it alongside moral distress is essential for capturing the full organizational context. However, research focusing specifically on moral distress and ethical climate among Japanese ICU nurses remains limited, and few studies have attempted to investigate these issues using a mixed-methods approach that integrates both quantitative and qualitative perspectives.
To address these knowledge gaps and generate contextually relevant insights, this study employed an explanatory sequential mixed-methods design. This study aimed to clarify the extent and circumstances under which Japanese ICU nurses experience moral distress, how they perceive the ethical climate of their organizations, and the relationship between moral distress and the perceived ethical climate. By combining a nationwide survey using validated Japanese instruments with in-depth qualitative interviews, this study sought to provide comprehensive, culturally informed recommendations for alleviating moral distress and improving the ethical climate in Japanese ICUs.
Review of the Literature
Overview of Moral Distress in International Research
Moral distress, originally defined by Jameton (1984) as the psychological and emotional distress experienced when individuals are unable to act according to what they believe is ethically right, has been extensively documented in various healthcare settings. International studies report that moral distress often arises in situations involving life-prolonging treatment, impaired patient decision-making capacity, disagreements among multidisciplinary teams, and resource limitations (Epstein & Hamric, 2009; Whitehead et al., 2015). A systematic review by Lamoureux et al. (2024) in psychiatric nursing identified associations between moral distress, burnout, diminished job satisfaction, and turnover intention. These findings underscore the global relevance of moral distress while also highlighting that its causes and manifestations differ across healthcare systems, organizational cultures, and sociocultural contexts.
Ethical Climate and International Evidence
Ethical climate refers to employees’ shared perceptions of how ethical issues are recognized, discussed, and addressed in their organization, as well as the behaviors that are supported regarding ethical practice (Olson, 1998; Victor & Cullen, 1988). Numerous studies have demonstrated that a positive ethical climate—characterized by open communication, supportive leadership, respect for nurses’ autonomy, and opportunities to voice concerns—plays a protective role in mitigating moral distress (Silén et al., 2011; Whitehead et al., 2015). For example, research among emergency nurses in China showed that a favorable ethical climate can buffer the impact of moral distress on burnout (Wu et al., 2025), while evidence from South Korea indicates that ethical leadership is strongly associated with an improved ethical climate and lower moral distress among hospital nurses (Noh & Kim, 2024). Collectively, these findings highlight the importance of organizational structures and ethical environments in shaping nurses’ ethical experiences and responses to distressing clinical situations.
Cultural and Organizational Characteristics of Japanese Healthcare
Japanese healthcare settings have distinctive structural and cultural characteristics that may influence both moral distress and the ethical climate. The healthcare system is traditionally organized around a hierarchical structure, and strong physician authority may often override nurses’ ethical concerns or clinical judgments (Freidson, 2017; Ruhnke et al., 2000). Additionally, Japanese cultural norms emphasize group harmony (wa) and the avoidance of overt disagreement, which may discourage nurses from openly expressing ethical concerns or challenging medical decisions.
In the context of end-of-life care, Japan also differs from Western countries. A comparative study by Ruhnke et al. (2000) revealed that Japanese clinicians tend to prioritize family preferences and physician decision-making over patient autonomy, a dynamic that may create ethical conflicts for nurses striving to uphold patient-centered care. Furthermore, studies on patient safety culture in Japan have noted challenges related to cross-hierarchical communication and continuous improvement—factors that may directly influence the development of an ethical climate (Fujii et al., 2021). These cultural and organizational factors suggest that Japanese ICU nurses’ experiences of moral distress may have unique characteristics not fully captured in international studies.
Moral Distress and Ethical Climate Research in Japan
To evaluate moral distress in Japanese clinical settings, Ishihara et al. (2018) developed the Japanese version of the Moral Distress Scale-Revised (JMDS-R), reflecting the linguistic and cultural characteristics of Japanese acute care hospitals. Similarly, the Japanese version of the Hospital Ethical Climate Survey (J-HECS) was validated by Inagaki et al. (2020) to measure the ethical climate in a manner that is culturally and organizationally appropriate for Japanese healthcare contexts.
Gaps in the Literature
Despite growing international evidence on moral distress and ethical climate, important gaps remain in the Japanese context. Few studies have examined ICU nurses’ moral distress and perceptions of the ethical climate together, with even fewer using mixed methods to connect prevalence with lived experience. The influence of hierarchical organizational structures as well as the cultural value of wa (harmony) on end-of-life ethical conflicts and nurses’ sense of powerlessness also remains insufficiently explored.
Study Purpose
Given these gaps, this study aimed to identify the extent and circumstances under which Japanese ICU nurses experience moral distress, describe how they perceive the ethical climate of their organizations, and examine the relationship between moral distress and ethical climate using an explanatory sequential mixed-methods approach.
This study employed an explanatory sequential mixed-methods design and is reported in accordance with relevant EQUATOR Network guidelines, including the Mixed Methods Appraisal Tool (MMAT) for mixed-methods research and the Consolidated Criteria for Reporting Qualitative Research (COREQ) for the qualitative component.
Methods
Research Context
The nursing workforce in Japan is predominantly female and exhibits an aging trend. Nurses qualify through multiple educational pathways, including vocational diplomas, junior/associate degrees, bachelor’s degrees, and graduate degrees. These contextual features help interpret the educational profiles reported in Table 2 and the distribution of ICU experience within our sample.
Study Design
This study integrated quantitative and qualitative data to elucidate: (1) the degree and nature of moral distress among Japanese ICU nurses, (2) their perceptions of ethical climates, and (3) the relationship between the two.
Explanatory Sequential Mixed-Methods Approach
This study employed an explanatory sequential design—a mixed-methods approach in which qualitative data explain and complement quantitative findings (Creswell & Plano Clark, 2007). The first phase involved a quantitative survey to capture the overall picture of moral distress and the ethical climate. In the second phase, a qualitative survey explored specific experiences and episodes, focusing particularly on significant associations or findings that required deeper interpretation. This provided a complementary and contextual understanding. This design combined the generalizability of quantitative research with in-depth qualitative insights, enabling a deeper understanding of complex ethical phenomena. It was well suited to the study’s objectives.
Definitions of Terms
Moral distress is defined, based on Jameton’s original conceptualization, as the psychological and emotional distress experienced by nurses when they recognize an ethically appropriate course of action but are unable to implement it because of institutional, organizational, or personal constraints (Jameton, 1984). Ethical climate is defined following Olson’s framework as employees’ shared perceptions of how ethical issues are recognized and addressed within an organization, as well as the attitudes and behaviors that are expected and supported regarding ethical conduct (Olson, 1998; Victor & Cullen, 1988).
Participants and Data Collection
Quantitative Phase
Nursing directors at 315 specialist training facilities registered with the Japanese Society of Intensive Care Medicine were contacted to request research cooperation, and consent was obtained from 54 facilities (17.1%). A minimum sample size of 120 was established based on prior research linking moral distress and organizational factors to ensure the detection of significant associations. A post-hoc power analysis was conducted using G*Power (version 3.1). For a multiple regression analysis with five predictors, assuming a medium effect size (f2 = 0.15), α = 0.05, and power = 0.80, the required sample size was 92. With 168 participants, the actual power exceeded 0.90, indicating sufficient power to detect medium effects.
A web-based survey was conducted from January to February 2022. Participants were recruited through facility-approved posters and responded anonymously using their personal devices. The final question assessed interest in follow-up interviews, identifying participants who had at least three years of ICU experience and self-reported moral distress.
Registered nurses currently working in ICUs who were employed at one of the participating facilities and able to understand and complete the Japanese-language questionnaire were eligible to participate. Nurses who were not currently working in an ICU setting (e.g., on leave or transferred) and those unwilling to provide informed consent were excluded. The facility participation rate was 17.1% (54/315). While this response rate is comparable to national-level nursing surveys in Japan, potential selection bias remains, as participating institutions may be more academically affiliated or ethically proactive than non-responding institutions. Generalizability should, therefore, be interpreted with caution.
Qualitative Phase
Eleven nurses were selected through purposive sampling based on the results of the quantitative survey. Variations in moral distress and ethical climate scores were considered to ensure a diversity of experiences and perspectives. Data collection continued until thematic saturation was achieved, with no new themes emerging in the final interviews.
Online semi-structured interviews, each lasting 40 to 60 minutes, were conducted from April to August 2022. The interview guide included questions about specific experiences related to key situations of moral distress (e.g., end-of-life care and difficulties in collaboration) and ethical climate issues (e.g., relationships with physicians and organizational support) identified in the quantitative survey (see Supplemental Material 1 for the complete interview guide). Participants reflected deeply on their experiences, thoughts, emotions, and the organizational factors they recognized at the time. Interviews were audio-recorded with consent and transcribed verbatim.
Interview participants were purposively selected from survey respondents who had consented to be contacted for follow-up interviews, thereby ensuring variation in the JMDS-R and J-HECS scores. Nurses who declined to participate in the interview phase or whose schedules did not permit participation during the data collection period were excluded.
Qualitative Data Analysis
Qualitative data were analyzed using qualitative content analysis, following the methodological framework proposed by Schreier (2012). This approach was selected to systematically describe and interpret patterns in participants’ experiences related to moral distress and ethical climate. Two researchers independently coded the transcripts, discussed discrepancies, and reached consensus through iterative team discussions, thereby enhancing analytical rigor and credibility.
The qualitative component of this study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (see Supplemental Material 2 for the completed COREQ checklist). Qualitative data analysis was conducted manually, without using specialized software.
Measurement Scales
Scales Used in This Study

Ethical Climate
The ethical climate was measured using the Japanese Hospital Ethical Climate Survey (J-HECS), a culturally adapted version of Olson’s HECS for Japanese healthcare settings (Inagaki et al., 2020; Olson, 1998). The J-HECS comprises 18 items across five subscales and uses a five-point Likert response format, with higher total scores indicating a more positive ethical climate. Permission for its use was obtained from the developers.
Data Analysis
Quantitative Data Analysis
Descriptive statistics were calculated for participants’ basic attributes and scores based on the JMDS-R and J-HECS. Considering that the scale items were ordinal and group distributions were not assumed to be normal, Mann–Whitney U and Kruskal–Wallis tests were used for between-group comparisons.
Pearson’s product-moment correlation coefficients were calculated to examine the associations between moral distress (including the JMDS-R subscales) and ethical climate (including the J-HECS subscales). Pearson’s correlations were retained because they are considered sufficiently robust to modest deviations from normality at this sample size (n = 168). Statistical analyses were performed using JMP Pro 16.1 (JMP Statistical Discovery LLC, Cary, NC, USA), with a two-tailed significance level of p < .05.
Ethical Considerations
This study was approved by the relevant institutional ethics review committee. In addition, institutional permission was obtained from the participating nursing institutions prior to data collection. Electronic informed consent was obtained for the survey, and written consent was obtained for the interviews. All data were anonymized.
Participants were thoroughly informed both in writing and verbally (during interviews) about the research objectives and methods, voluntary participation, the right to withdraw consent at any time, assurance of anonymity, strict data management, the prohibition of non-research use, and the methods of publishing the findings. Informed consent was obtained after confirming that the participants fully understood the information. Consent for the web surveys was provided via an “agree” button, while written signatures were obtained for the interviews. Data were managed using anonymous IDs, with the master list stored separately in a secure, locked location.
Results
Quantitative Survey Findings
Of the 171 ICU nurses from 54 consenting facilities, three duplicate responses from the same IP address were excluded, yielding 168 valid responses (a 98.2% valid response rate).
Participant Attributes
Basic Attributes (N = 168)

Moral Distress
Mean Scores and Standard Deviations for Moral Distress (JMDS-R) and Ethical Climate (J-HECS) Subscales

Perceptions of Ethical Climate
The mean total J-HECS score was 56.74 (SD = 12.13). Among the subscales, “organizational support through a clear hospital philosophy” (M = 11.46, SD = 3.25) and “trust and collaboration from physicians” (M = 11.10, SD = 3.09) had relatively low mean scores.
Correlation Between Moral Distress and Ethical Climate Subscales
Correlations Between Moral Distress (JMDS-R Level Subscales) and Ethical Climate (J-HECS Subscales)

Each cell presents correlation coefficients (r values) with their corresponding p-values.
Relationship Between Respondents’ Basic Attributes and Moral Distress Levels
Figure 1 illustrates the mean moral distress levels across age, years of nursing experience, years of ICU experience, and specialized certification status, with statistically significant group differences identified for each variable. Relationship between Participants’ Attributes and their Level of Moral Distress (Mean JMDS-R Score)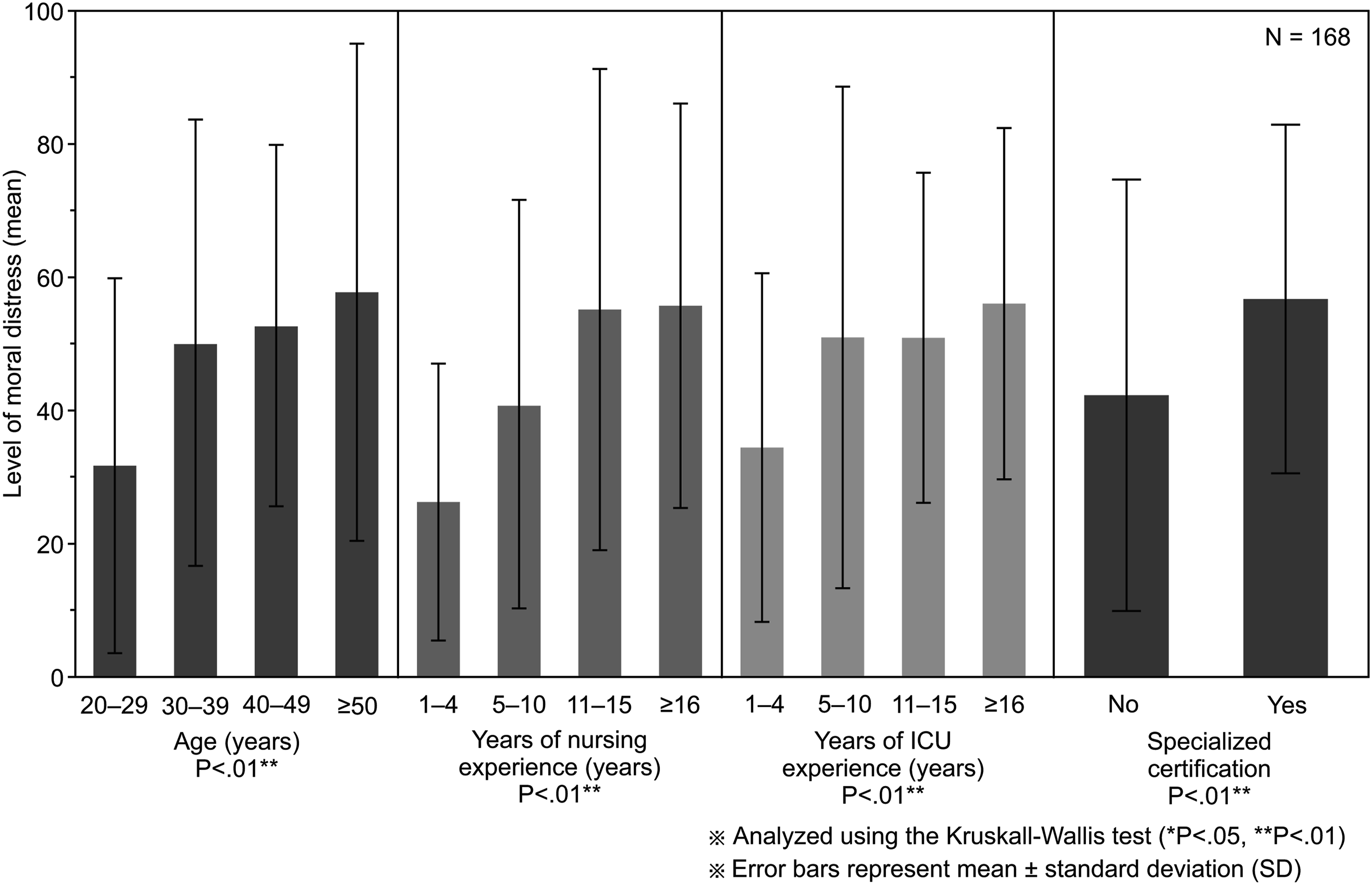
Qualitative Survey Findings: Complementing Quantitative Findings
Overview of Interview Participants (N = 11)

Key Themes Identified in the Qualitative Analysis, Description, and Representative Quotes

Key Themes
Theme 1: Ethical Dilemmas and a Sense of Powerlessness in End-of-Life Care
The quantitative survey showed that the JMDS-R subscale “lack of respect for patient dignity” had the highest mean score (Table 3). End-of-life care emerged as a salient context in the qualitative interviews, as illustrated by the following account: “Despite the evident end-of-life status, no one decides to discontinue treatment; we just continue interventions day after day. It is distressing for the patients, their family members, and us” (Participant G). Participants frequently expressed a sense of powerlessness regarding futile life-sustaining treatment and disagreements among family members (Participants I and F), confirming that these factors intensify moral distress.
Theme 2: Collaborative Challenges and Concerns About Quality of Care
Regarding the JMDS-R subscale “Collaboration with Difficulty in Quality Assurance,” nurses reported concerns about working with inexperienced staff: “Currently, about half of the ICU staff are transfers…with no emergency or ICU experience” (Participant E), and communication issues: “When a complication occurs that a physician anticipated but we did not, they ask, ‘Why didn’t you catch that?’ This leaves us with the feeling that our nursing care is not valued.” (Participant G).
Theme 3: Perceived Challenges in Organizational Culture and Ethical Climate
In relation to “organizational support through a clear hospital philosophy” and “trust and collaboration from physicians,” which scored low on the J-HECS scale, the narratives highlighted “harmful effects of a physician-centered decision-making process.” For example, according to Participants C, H, and E, “nurses’ opinions are often overruled by a single word from physicians, and adequate communication with physicians is impossible.” Further, concerning “dissatisfaction with unclear hospital philosophy and policies,” specific challenges with organizational support systems were expressed, with Participants I and F noting that hospital policies were ambiguous, leaving frontline staff struggling to adapt to constantly changing directives.
Theme 4: Risk of Care Routinization and Diminished Ethical Sensitivity
Regarding the “decline of nursing quality due to routinization of nursing duties,” participants noted that “morning care is provided uniformly without adequate consideration of individual patient circumstances” (Participants H and J) and “there are many tasks beyond core nursing duties, leaving us overwhelmed with clerical work” (Participant C). This was considered a contributing factor to the low ethical climate ratings observed in the quantitative data.
Discussion
This study employed a mixed-methods design to comprehensively examine moral distress among ICU nurses in Japan and its relationship with the ethical climate. The main findings were: (1) moral distress among Japanese ICU nurses is particularly pronounced in end-of-life care and tends to intensify with accumulated years of experience; and (2) a positive ethical climate—particularly “organizational support through a clear hospital philosophy”—was negatively associated with distress arising from “collaboration with difficulty in quality assurance.” These findings should be interpreted in the context of the unique Japanese healthcare culture. In the Japanese context, the cultural value of “wa” (harmony) can discourage open disagreement and the expression of ethically justified concerns, particularly within hierarchical physician–nurse relationships. Repeated suppression of such concerns may prevent ethical issues from being resolved and thereby contribute to the accumulation of moral residue over time. Together, the qualitative themes help explain the quantitative patterns: Theme 1 clarified why end-of-life care emerged as the most salient source of moral distress; Theme 2 illuminated distress related to collaboration with difficulty in quality assurance; Theme 3 explained why limited organizational support and physician-centered decision-making contributed to a poorer ethical climate; and Theme 4 further suggested that routinized practice may suppress ethical sensitivity and reinforce these difficulties. The qualitative themes related to end-of-life care—including “sense of powerlessness due to continuation of futile treatment,” “disagreements with patients’ family members,” and “dissatisfaction with physician-centered decision-making”—elaborated the contexts in which moral distress was most acutely experienced. The present study suggests that some features of the Japanese cultural context—such as reluctance to make explicit end-of-life decisions, social pressure to prioritize family wishes, and organizational cultures marked by deference to physician authority—may further exacerbate moral distress (Freidson, 2017; Ruhnke et al., 2000). This finding aligns with that of Ruhnke et al., who revealed in their Japan–US comparison that, in Japan, the wishes of patients’ family members are prioritized over the patients’ own wishes in treatment-related decisions, and physician authority tends to be relatively strong (Ruhnke et al., 2000). The situations described in the qualitative data—such as “no one makes the decision to discontinue treatment; interventions simply continue”—likely reflect a complex interplay of cultural norms that prioritize contextual factors and interpersonal relationships over individual patient autonomy. This indicates that, although moral distress is a cross-cultural phenomenon, its manifestations and intensity are shaped by each society’s unique sociocultural landscape. Izumi et al. emphasized the importance of delivering high-quality nursing care to patients with advanced diseases (Izumi et al., 2010). In this study, ICU nurses’ end-of-life distress stemmed from their ethical aspirations to provide dignified care—an aspiration impeded by cultural and organizational constraints.
The finding that nurses with more years of ICU experience reported higher moral distress can be theoretically explained through Epstein and Hamric’s concepts of moral residue and the crescendo effect—the idea that unresolved ethical conflicts accumulate internally and intensify over time, as similar situations recur (Epstein & Hamric, 2009). This aligns with Dodek et al.’s international research findings linking years of professional ICU experience with higher moral distress (Dodek et al., 2016). However, our qualitative data also suggest that Japanese organizational culture, with its emphasis on seniority and group harmony (“wa”), may inhibit less experienced nurses from voicing their ethical concerns. If they do voice these concerns, they are unlikely to receive organizational support (e.g., “nurses’ opinions are overruled by a single word from a physician”). In such an environment, unresolved ethical conflicts may accumulate more severely, suggesting that veteran nurses not only encounter more distressing situations but also bear a heavier burden of unresolved issues. A systematic review by Lamoureux et al. on psychiatric nurses highlighted that chronic moral distress exacerbates burnout, depersonalization, cynicism, and decreased job satisfaction (Lamoureux et al., 2024). These findings underscore the possibility that accumulated experience might not necessarily translate into reduced distress or improved coping skills; instead, it may amplify feelings of helplessness and resignation.
These findings reflect broader international concerns that task overload, routinization, hierarchical communication, and pandemic-related pressures can impair ethical sensitivity and intensify ICU nurses’ moral distress (Donkers et al., 2021; Silverman et al., 2022).
Together, these studies support our interpretation that routinized care practices and a lack of ethical dialogue reflect not merely individual issues but broader systemic and cultural factors, highlighting the need for organizational and structural responses (Donkers et al., 2021; Silverman et al., 2022). Prior work has noted how hierarchical decision-making and ambiguous institutional policies can undermine nurses’ moral agency; our findings align with these observations and extend them to ICU contexts in Japan.
One of the key findings of the present study was the significant negative correlation between “organizational support through clear hospital philosophy” (an aspect of the ethical climate) and moral distress related to “collaboration with difficulty in quality assurance.” Studies have demonstrated a strong association between perceived organizational support and reduced moral distress among nurses (Robaee et al., 2018), reinforcing the importance of clear organizational philosophy and support structures. This suggests that when hospital philosophy and ethical guidelines are clearly and tangibly reflected in multidisciplinary decision-making, resource allocation, and staff education, nurses’ recognition of this as organizational support may reduce the distress arising from team conflicts and competency differences that affect care quality. This emphasis on clear organizational direction and robust support systems is central to fostering a culture of patient safety. Fujii et al. (2021) found that Japanese hospitals scored poorly on the continuous improvement mindset dimension of their patient safety culture. The low ratings for “organizational support through a clear hospital philosophy” may reflect that nurses perceive a lack of sustained, organization-wide commitment to ethical practice and care quality improvement (Fujii et al., 2021). A positive ethical climate may enhance psychological safety and promote constructive communication, contributing to the improvement of patient safety culture. Therefore, fostering such a climate is crucial not only for reducing moral distress but also for broader organizational improvement.
In recent years, there has been increasing recognition of the importance of measuring and researching moral distress among Japanese healthcare professionals. In addition to the JMDS-R used in this study, new instruments are being developed and adopted to more comprehensively capture contemporary aspects of moral distress—such as excessive documentation tasks and administrative directives that undermine care quality (Ishihara et al., 2018). The Japanese version of the Measure of Moral Distress for Healthcare Professionals (MMD-HP), originally developed by Epstein et al. (2019), was validated by Fujii et al. (2021). These advancements will deepen our understanding of the multifaceted dimensions of moral distress in Japanese clinical settings and pave the way for developing targeted interventions. The findings of this study are consistent with domestic research trends. Pandemic-specific conditions likely amplified several mechanisms identified in our data. Visitor restrictions complicated end-of-life communication and may have increased perceptions of futility, while staffing shortages and the redeployment of inexperienced staff strained collaboration, thereby intensifying moral distress in high-acuity settings. These pandemic-related dynamics may have particularly influenced three key findings of the present study. First, the high moral distress scores in end-of-life care situations may reflect not only longstanding cultural constraints, but also pandemic-specific barriers to family-centered communication, such as restricted visitation policies that prevented nurses from facilitating meaningful conversations between patients and families. Second, the relatively low scores for “organizational support through a clear hospital philosophy” may have been further depressed by the institutional ambiguity and rapid policy changes that were characteristic of the early pandemic period, when institutional guidance was frequently inconsistent or absent. Third, the positive association between ICU experience and moral distress may have been amplified under pandemic conditions, as experienced nurses—bearing greater clinical responsibility and a heavier accumulated moral residue—faced unprecedented ethical demands with inadequate systemic support. Therefore, while the patterns observed in this study likely reflect the underlying structural and cultural features of Japanese ICU nursing, the absolute levels of moral distress as well as ethical climate scores should be interpreted with consideration of the extraordinary circumstances during the pandemic period. As such, replication under non-pandemic conditions is warranted.
Drawing on the present study’s quantitative survey findings—specifically the correlation between ethical climate and moral distress—as well as qualitative insights from nurses’ lived experiences and organizational requests, we propose the following concrete measures to mitigate moral distress among ICU nurses.
Medical facilities should implement clear ethical guidelines for end-of-life care and establish regular multidisciplinary ethics conferences to review individual cases and support decision-making, thereby reducing nurses’ sense of powerlessness. These conferences should be institutionalized to empower nurses to participate as colleagues whose opinions are respected, with training focused on facilitative skills and psychological safety. Ethical leadership development programs should be offered to leaders across medical disciplines to foster heightened ethical sensitivity throughout the organization. Finally, institutions should expand nurses’ discretionary authority in care provision and promote more active nurse participation in treatment decision-making to prevent the routinization of care.
The implementation of these recommendations may face barriers such as the existing organizational culture, hierarchy, and constraints on time and human resources. Key factors for successful implementation include commitment from leadership, continuous interdisciplinary dialogue, mutual understanding, and sharing specific success stories.
Strengths and Limitations
Strengths
This study has several strengths. First, it employed an explanatory sequential mixed-methods design that integrated quantitative survey data with in-depth qualitative interviews. This design allowed us to capture both the prevalence and the contextual meaning of moral distress and the ethical climate among ICU nurses in Japan. Second, we used validated Japanese versions of the Moral Distress Scale-Revised (JMDS-R) and the Hospital Ethical Climate Survey (J-HECS), which ensured good psychometric properties and cultural appropriateness. Third, the analysis was explicitly contextualized within Japanese healthcare culture, including hierarchical physician–nurse relationships and the value of wa (harmony), thereby enhancing the interpretability and relevance of the findings for domestic practice. Fourth, the study was theoretically grounded in concepts such as moral residue and ethical climate, which strengthened the coherence among our research questions, methods, and interpretation of results. Finally, the study followed rigorous procedures for qualitative data collection and analysis, adhered to COREQ guidelines, and employed investigator triangulation to enhance the credibility and trustworthiness of the findings.
Limitations
This study also has some limitations. First, participants were self-selected volunteers from facilities that agreed to participate, which may limit the generalizability of the findings; participating institutions might have been more academically affiliated or ethically proactive than non-responding facilities. Second, the web-based survey and interviews were conducted during the COVID-19 pandemic (January to August 2022), a particularly challenging period for healthcare workers. Heightened stress, altered protocols, restricted visitation, and staffing constraints may have influenced both the level and domains of moral distress, as well as perceptions of the ethical climate. Third, as a cross-sectional study, this research cannot establish causal relationships between moral distress and the ethical climate. Fourth, the measures relied on self-reporting, which may be subject to recall bias and social desirability bias. Fifth, nurses who had already left the profession because of severe moral distress were not included in the sample; therefore, the actual level of moral distress among ICU nurses may have been underestimated. These limitations should be considered when interpreting and generalizing the findings, highlighting the need for longitudinal and intervention studies in the future.
Implications for Practice
The findings of this study have several important implications for practice. Clarifying ethical guidelines for end-of-life care and institutionalizing regular interprofessional ethics conferences may help reduce nurses’ sense of powerlessness and support ethically consistent decision-making. Strengthening multidisciplinary collaboration and ensuring that nurses’ voices are heard can mitigate distress arising from communication barriers and physician-centered decision-making. Furthermore, cultivating ethical leadership across professions may enhance the organizational ethical climate by reducing ambiguity in hospital philosophy and promoting shared ethical values. Finally, expanding nurses’ autonomy and participation in clinical decision-making may prevent the routinization of care and support ethically grounded nursing practice in Japanese ICUs.
Conclusion
Japanese ICU nurses experience moderate levels of moral distress, particularly in end-of-life care, and a positive ethical climate correlates with lower levels of moral distress. These findings underscore the necessity of improving the ethical climate in medical facilities, with careful consideration of organizational and cultural contexts. Establishing an organization-wide support system is crucial. This includes promoting multidisciplinary collaboration, supporting ethical decision-making, ensuring psychological safety, strengthening leadership among managers, and providing continuous ethics education.
This study reaffirms that moral distress in Japanese ICUs is an organizational rather than an individual issue. It provides foundational data for future research on nursing ethics and clinical practice.
Future research should explore the development and evaluation of interventions tailored to improving the ethical climate in the ICU, such as structured ethical decision-making systems, ethics consultation services, and simulation-based ethics training. Additionally, longitudinal studies are needed to examine how changes in organizational policies and leadership practices influence moral distress over time. Cross-cultural comparative studies can reveal both universal and culture-specific factors that shape ICU nurses’ moral distress across diverse healthcare systems.
Supplemental Material
Supplemental Material - Moral Distress and Ethical Climate Among Japanese Intensive Care Unit Nurses
Supplemental Material for Moral Distress and Ethical Climate Among Japanese Intensive Care Unit Nurses by Hideki Yamauchi and Kyoko Ueno in Sage Open Nursing.
Supplemental Material
Supplemental Material - Moral Distress and Ethical Climate Among Japanese Intensive Care Unit Nurses
Supplemental Material for Moral Distress and Ethical Climate Among Japanese Intensive Care Unit Nurses by Hideki Yamauchi and Kyoko Ueno in Sage Open Nursing.
Footnotes
Acknowledgments
The authors express their sincere appreciation to all participating ICU nurses and facility administrators for their cooperation and valuable contributions to this study.
Ethical Considerations
This study was approved by the Research Ethics Committee, Graduate School of Health Care and Nursing, Juntendo University (No. Junkanrin 2021-71). Participants were informed in writing and, for interview participants, also verbally about the research purpose and procedures, voluntary participation, the right to withdraw consent at any time, confidentiality protections, secure data management, and the use of the findings for research purposes only.
Consent to Participate
Survey participants provided electronic informed consent by selecting an “agree” button prior to completing the questionnaire. Interview participants provided written informed consent before the interview.
Author Contributions
Hideki Yamauchi: Conceptualization, methodology, investigation, formal analysis, writing – original draft, writing – review & editing. Kyoko Ueno: Supervision. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Japan Society for the Promotion of Science (JSPS) KAKENHI (JP22K10857).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified quantitative data and a variable codebook are available from the corresponding author upon reasonable request. Full qualitative interview transcripts are not publicly available because participant consent and ethical restrictions do not permit public sharing of potentially identifiable narrative data. Anonymized illustrative quotations are included in the manuscript, and additional de-identified qualitative materials may be shared upon reasonable request, and subject to institutional approval.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.