
Abstract
Introduction
Indiscriminate use of antibiotics has led to antibiotic resistance, a global health threat. In low- and middle-income countries like Bangladesh, the situation is particularly dire. Nursing students are a concerned population as they have their respective part to play in antibiotic resistance. There is a lack of understanding about their knowledge, attitude and practice regarding antibiotic usage and resistance among this demographic.
Methodology
A cross-sectional study design was employed and third- and fourth-year nursing students were recruited for the study from both government and non-government institutions in Bangladesh. Data were collected using a self-administered structured questionnaire. Descriptive statistics and multiple logistic regression analyses was performed using Stata version 16.
Results
Among 664 participants, 83.58% of the students demonstrated good attitudes (>80%) and practices (>80%) towards antibiotic resistance, while 57.9% exhibited good knowledge. Older students had higher odds of good knowledge (aOR = 1.29) and practice (aOR = 1.84). Female gender (aOR = 2.00), private-institution enrollment (knowledge aOR = 1.57; attitude aOR = 3.44; practice aOR = 2.25), and Bachelor of Science enrollment (knowledge aOR = 2.13; attitude aOR = 3.38; practice aOR = 2.44) were associated with higher odds of good KAP. In contrast, fourth-year students showed lower odds of good attitude (aOR = 0.09) and practice (aOR = 0.45). Knowledge was weakly but significantly correlated with both attitude (r = 0.18, p < 0.001) and practice (r = 0.09, p = 0.041).
Conclusion
Nursing students in Bangladesh show promising attitudes and practices towards antibiotic resistance. Efforts to enhance education on antibiotic resistance are necessary in guiding these future healthcare providers to combat this emerging threat effectively.
Introduction
Antibiotics have played an important therapeutic role in reducing morbidity and mortality resulting from multiple diseases, particularly bacterial infections (Nair et al., 2019). Antibiotic resistance (ABR) is increasing daily because of the use of antibiotics without appropriate indications and proper etiquette as seen during the COVID-19 pandemic (Jainlabdin et al., 2021). The World Health Organization (WHO) warns that the world is entering an age, in which antibiotics are used to treat even minor sickness and injuries (World Health Organization, 2023). If the infection cannot be treated with appropriate antibiotics, it poses an opportunity for mild illness to transition to something severe and life-threatening. This escalating threat is reflected in its global toll, as antimicrobial resistance is responsible for an estimated 1.27 million deaths annually and imposes a heavy economic burden on healthcare systems (Murray et al., 2022).
Antibiotics act on bacterial cell walls, protein synthesis, and nucleic acid synthesis (Kapoor et al., 2017). Resistance to antibiotics occurs when bacteria resist drugs that are meant to kill or restrict their growth due to overuse and misuse of antibiotics. Bacteria undergo genetic changes that alter antimicrobial targets or reduce drug access, enabling them to survive otherwise inhibitory antibiotics (Urban-Chmiel et al., 2022).
It is rapidly becoming a global issue due to multiple factors such as patients’ self-medication, the availability of antibiotics without requiring a physician’s prescription, not completing the designated course, and incorrect prescriptions (Ahmed et al., 2019; Haque et al., 2019; Hoque et al., 2020; Melles-Brewer et al., 2024). Physicians, nurses, nursing students, and paramedics, play active roles in this influence, as their knowledge, attitude, and professional practice contribute directly to ABR's development (Hoque et al., 2020). In China, evidence from outpatient prescription data indicates that 50.7% of antibiotic prescriptions were inappropriate in primary care settings (Zhao et al., 2022). In comparison, recent data indicate that at least 28% of outpatient antibiotic prescriptions in the United States are not needed, representing a considerable level of inappropriate use (Health Care Providers, 2025).
Bangladesh, like many LMICs, faces disproportionate challenges in controlling antibiotic misuse due to weak regulation, widespread retail sales, and limited surveillance. A high prevalence of cases of resistance to antibiotics remains, and many frequently used medicines have become ineffective, which increases the treatment cost and medication discontinuation rate. Which in turn increases ABR, creating a morbid, never-ending cycle (Ahmed et al., 2019). The lack of surveillance and accurate regional information regarding the current status of the ABR fuels this self-perpetuating cycle. Recent assessments show that although nearly two-thirds of drug-sellers had dispensing training, their knowledge of antibiotic use was only moderate (60.2%), over half (57.5%) were unaware of policies, and more than two-thirds of their recommendations deviated from guidelines (Al Masud et al., 2025). People who visit healthcare centers frequently purchase medicines from retail drug shops; therefore, the prescriber and drug supply chain play an important role (Lucas et al., 2019). Quantitative data show that about half of antibiotic sales (37–57%) are done without a registered physician's prescription (Al Masud et al., 2024, 2025; Islam et al., 2022). Qualitative research also highlights that improper dispensing and incomplete dosing are common practices (Lucas et al., 2019; Nahar et al., 2020).
Studies in Bangladesh reveal existing knowledge gaps and inappropriate prescribing practices among healthcare providers, which exacerbate the situation (Ahmed & Islam, 2012; Nahar et al., 2020). Certain practices are ubiquitously reported in studies conducted in Bangladesh, such as prescribing antibiotics without testing the sensitivity through laboratory tests, prescribing for diseases that do not necessarily require antibiotics, two or more antibiotic prescriptions at the same time, and greater antibiotics prescribing frequency in hospital or clinical settings (Biswas et al., 2015; Haque, 2017; Hoque et al., 2020). Healthcare workers play a significant role in this regard due to their involvement with medication and prescribing drugs. The Knowledge, Attitude, and Practice (KAP) framework provides a useful behavioural lens to assess both cognitive understanding and practical behaviours regarding antibiotic use, and has been widely applied in healthcare research (Jahromi et al., 2025). The KAP model posits that knowledge is a necessary but not sufficient precondition for attitudinal change, and that attitudes in turn may — but do not always — translate into practice. This directionality has been widely assumed in health behaviour research, though empirical evidence suggests the relationships are often weak, mediated by contextual factors, and non-linear. In the present study, the KAP framework is applied descriptively to assess each domain independently and to examine their interrelationships, without assuming a causal pathway.
Nurses are at the heart of antibiotic stewardship owing to their responsibilities of administering medicines, monitoring patients, and counselling families. In Bangladesh, nursing students are prepared to do these roles by a curriculum consisting of clinical responsibilities before graduation and training on antibiotics and ABR (BNMC, 2019a, 2019b; Jayaweerasingham et al., 2019). Few previous studies have targeted nursing students, an integral part of the healthcare provision team in a hospital setting. By addressing this evidence gap, this study aims to inform curriculum reforms and national policy on antimicrobial stewardship training for nurses in Bangladesh. The general objective of the study was to assess knowledge, attitudes, and practices about the use and resistance of antibiotics among nursing students in Bangladesh. Specifically, it aimed to explore nursing students’ knowledge on the use and resistance of antibiotics, assess their attitude towards proper use and resistance to antibiotics, and evaluate practices to prevent antibiotic resistance. This study also sought to establish the relationship between knowledge, attitude, and practice, while additionally investigating factors associated with knowledge, attitude, and practice regarding antibiotic use and resistance. A better understanding of what the students know and think about the issues of antibiotic usage and resistance will be instrumental in creating an effective and customized educational intervention for them (Hoque et al., 2015).
Literature Review
Antibiotic resistance (ABR) is now one of the most important public health threats of the 21st century. According to the World Health Organization (WHO), that antibiotic resistance could lead to a future where common infections and injuries that are currently treatable with antibiotics may become fatal again. (World Health Organization, 2023). Inadequate healthcare infrastructure and poor regulatory systems cause more than 1.27 million deaths annually due to ABR in low- and middle-income countries (LMICs) (Ahmed et al., 2019).
In Bangladesh, ABR is a severe threat to public health systems evidenced by multiple studies reporting high resistance rates of antibiotics (Ahmed et al., 2019; Hoque et al., 2020). This is made worse by the fact that there is widespread over the counter access to antibiotics, diagnostic testing is not being done, and there is not much in place in terms of antimicrobial stewardship policies (Nahar et al., 2020). The COVID-19 pandemic further accelerated the misuse of inappropriate antibiotics, including the inappropriate use of antibiotics prophylactically or symptomatic despite the fact that COVID-19 is a viral infection (Jainlabdin et al., 2021).
Primarily, antibiotics work against bacterial cell wall synthesis, protein synthesis, or DNA replication. Bacteria develop resistance when they acquire the ability to defeat or circumvent these mechanisms through genetic mutation or horizontal gene transfer (Kapoor et al., 2017; Urban-Chmiel et al., 2022). The molecular basis of resistance is known, but human behavior is key to propagation.
ABR is also influenced by self-medication, incomplete courses, and demand driven prescribing. Up to 90 percent of all antibiotics sold in Bangladesh are sold without prescription and many are misused because of lack of public awareness and lax pharmacy regulation (Lucas et al., 2019). Prescribers often prescribe antibiotics empirically or in response to patient pressure, even when clinical indications are absent, contributing to the acceleration of antimicrobial resistance (Khan & Ahmed, 2025).
The prescribing practices, the antibiotic administration and patient counseling of healthcare providers are critical in either promoting or inhibiting ABR. Especially nurses are the critical links between physicians and patients, and central to patient care. In the context of LMICs such as Bangladesh where nurses are often responsible for extended responsibilities in the absence of physicians, nurses’ understanding of antibiotic stewardship becomes even more important (Ahmed & Islam, 2012).
Antibiotic administration and patient interactions are part of the training process of nursing students, who undergo clinical rotations as the part of their training. They are essential actors in antibiotic use practices since they are exposed to it very early. However, studies demonstrate that healthcare students do not receive enough training on antimicrobial resistance before entering the workforce (Kotwani et al., 2021; Nogueira-Uzal et al., 2020).
Several studies have been performed to determine the knowledge, attitude, and practices (KAP) of the ABR of healthcare students. Okedo-Alex et al. reported 64.7% of Nigerian medical students having good knowledge of antibiotic use and resistance (Okedo-Alex et al., 2019). A large gap among different populations was found, as only 47% of the general public in Kuwait had adequate knowledge (Awad & Aboud, 2015). In Sri Lanka, nursing students had varying degrees of understanding and their knowledge were surprisingly not related to practice (Jayaweerasingham et al., 2019).
Pharmacy and medical students have been seen to have greater knowledge scores compared to nursing students mostly due to the differences in their curriculum contents (Al-Qerem et al., 2022). In addition, in some contexts such as Lebanon and Iraq, knowledge was high but attitudes towards antibiotic use were inconsistent (Al-Salih et al., 2019; Sakr et al., 2020). This reinforces the fact that it is not just information, but also behavioral and curricular reinforcements.
Concerning practices including prescription of more than one antibiotic where there were no absolute indications and not issuing culture and sensitivity tests that assesses the sensitivity of an antibiotic for an individual before issuing the antibiotic, have been reported several times in Bangladesh (Biswas et al., 2015; Datta et al., 2016). There are no studies that assessed the knowledge, attitude and practice of nursing students in Bangladesh, while there are very few studies that involved general practitioners and medical students (Hoque et al., 2015).
In the second year, the curriculum for BSc and Diploma in Nursing includes topics on antibiotic resistance, however the depth and methods of delivery vary from institution to institution (BNMC, 2019a; 2019b). In addition, institutional quality differences of private and public nursing schools may influence student preparedness (Climer et al., 2025). These gaps leave a failing foundation for future nurses to have responsible antibiotic practices.
Repeatedly, educational exposure is shown to influence KAP levels. Structured training in antimicrobial stewardship is known to increase knowledge and encourage attitudes congruent with best practices (Mersha, 2018). Inclusion in the syllabus alone is not enough. In Bangladesh, nursing students report learning about ABR in the second year, and reinforcement across later years may be lacking, given evidence of declining practice and attitude in fourth year students (Rábano-Blanco et al., 2019).
Internationally, the curricula have been recommended to be reformed to include repeated and case based ABR education, supported by practical modules and clinical simulations (Reena & Ittyachen, 2022). Interventions targeted during clinical rotations could also counteract the influence of irrational prescription practices that are common in tertiary care hospitals.
Although nursing students are highly involved in antibiotic use pathways in Bangladesh, there is no such comprehensive national level study on their KAP regarding antibiotic use and resistance. There is no multivariable analysis, validated instruments or correlational assessment between the KAP domains within existing research. These gaps are addressed in this study by sampling representative institutional types and programs (Diploma and BSc), and not only prevalence but also the predictors of good knowledge, attitudes and practices. Therefore, the objectives of this study were: 1. To assess the level of knowledge, attitudes, and practices (KAP) of nursing students regarding antibiotic use and resistance. 2. To identify socio-demographic and academic factors associated with KAP levels. 3. To examine the correlation between knowledge, attitude, and practice regarding antibiotic use and resistance.
These findings can help to identify targeted curriculum reforms and policy measures to improve antibiotic stewardship practices of future nurses in Bangladesh by elucidating the interrelationships among KAP domains and the effects of educational and demographic factors.
Methods
Design
This study was conducted using a cross-sectional design from 16th April 2024 to 07th July 2024. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline for cross-sectional studies. The completed STROBE checklist is provided as supplementary material.
Research Question
This study assessed the levels of knowledge, attitude and practice (KAP) regarding antibiotic use and resistance and identified the factors that are associated with the KAP levels.
Sample
Data were collected from third- and fourth-year students of the Government and Non-government BSc and Diploma Nursing institutes across Bangladesh. Stratified random sampling was used, and the population was initially stratified into government (n=67) and non-government (n=330) institutes considering the total attending students in these institutions. Twenty institutes were randomly selected (8 government and 12 non-government), considering the total number of institutes in each stratum. The sample size was calculated to estimate a single proportion with predefined precision, separately for government and non-government nursing institutes. The initial sample size was estimated using the single-population proportion method at a 95% confidence level, with a 5% margin of error and a conservative assumed prevalence of 50% due to the absence of prior estimates. As individual-level enrolment data were not publicly available, finite population correction was applied using the officially sanctioned seat capacity for nursing programmes, published by the governmental authority, as a proxy for the population size within each stratum. The resulting stratum-specific sample sizes were rounded up to the nearest integer and allocated proportionally in accordance with the stratified random sampling design. A total of 666 nursing students participated in this study. 280 participants were from government institutes and 386 from non-government institutes (Supplementary Table 1).
Inclusion/Exclusion Criteria
As according to the curriculum or B.Sc. and Diploma Nursing Course in Bangladesh, the students are taught about Antibiotic usage and resistance in 2nd year. As such third- and fourth-year students from BSc or Diploma courses from government or non-governmental organizations in Bangladesh who were present on the day of data collection and provided written informed consent. First- and second-year students, and those that were unwilling to participate were excluded. (BNMC, 2019a; 2019b). Subjects fulfilling the inclusion criteria were invited to participate, and upon agreement, they were provided with the data collection tool and a written informed consent form.
Institutional Review Board Approval, Informed Consent, and Human Subjects’ Rights Required
Approval was received from an Institutional Review Board (IRB)/Ethical Review Committee (ERC) of the appropriate University for this survey. Only eligible students who met the inclusion criteria and provided the written informed consent were included. The study was conducted in accordance with the principles of the Declaration of Helsinki, and participant confidentiality was strictly maintained.
Data Collection Instruments
A structured self-administered questionnaire was adapted after an extensive literature review from previously published KAP instruments on antibiotic resistance and was contextually modified for the Bangladeshi nursing education setting (Jainlabdin et al., 2021; Kanneppady et al., 2019; Sakr et al., 2020; Zulu et al., 2020). It was pretested on 21 participants, who were not included in the final analysis. The final version of the questionnaire was structured based on pretesting. A panel of experts and experienced members evaluated the questionnaire and tested the validity and reliability of the questionnaire, and after their approval the final version of the questionnaire was prepared. The original English questionnaire was translated into Bengali using a forward-translation process. The Bengali version was then back-translated into English and then reviewed by a public health expert for linguistic and conceptual equivalence. Following reconciliation of any discrepancies, the instrument was piloted on 21 participants, who were not included in the final analysis, and necessary adjustments were made based on pretesting feedback. Content validity was assessed by a panel of subject-matter experts, and the final version of the questionnaire was prepared after their approval. The instrument was not subjected to full psychometric validation including confirmatory factor analysis or test–retest reliability assessment, and is therefore best characterised as an exploratory adapted tool. Internal consistency was assessed using Cronbach's alpha: knowledge domain α = 0.601, attitude domain α = 0.595, and practice domain α = 0.632. These values indicate limited internal consistency, falling below the conventional threshold of 0.70, and suggest possible heterogeneity within the constructs. Composite scores derived from these scales should therefore be interpreted with caution, as measurement error may attenuate observed associations. Item-level dimensionality assessment was not performed and is recommended in future studies.
The questionnaire included five sections: sociodemographic information, general information, knowledge, attitude, and practice of students regarding antibiotic resistance. The sociodemographic section included age, sex, marital status, attending institution type, curriculum, and year of study questions. The general information contained questions regarding previous consumption history and source of antibiotics, educational experience, and years of educational exposure to antibiotic resistance. Sociodemographic factors such as age and sex have been consistently identified as determinants of KAP regarding antibiotic resistance in prior literature (Guo et al., 2021; Jairoun et al., 2019). Institutional and curricular characteristics were included based on evidence that structural differences in nursing education, including programme type and ownership status, are associated with variation in student outcomes (Climer et al., 2025; Higuita-Gutiérrez et al., 2020).
The knowledge section contained 10 items, and the practice section contained 5 items. The knowledge section explored students’ knowledge regarding what antibiotic resistance is and when, where, and how antibiotics should be used to ensure ABR does not develop. The practice section focused on self-reported practice for the prevention of antibiotic resistance. Questions from both the knowledge and practice sections had binary responses (Yes/No), and a correct and wrong response was assigned a value of ‘1’ and ‘0’, respectively. As such, the knowledge section had a total score range of 0 to 10, and the practice section had a score range of 0 to 5. The attitude part contained 10 items exploring students’ attitudes towards the proper way of antibiotic prescribing and use. Here, a 3-point Likert scale was employed for responses with ‘Agree’=3, ‘Neither agree nor disagree’=2, and ‘Disagree’=1. The total score of the ‘Attitude’ section ranged from 10 to 30. The data collection procedure was conducted and monitored by the authors. Data entry and cleaning procedures began alongside data collection by co-investigators. Thereafter, regular crosschecking of data entry was performed by the investigators. Item-wise distribution (percentage) of correct answers is provided in the supplementary files (Supplementary Table 2).
Statistical Analysis
Categorical and continuous variables are presented as frequency, percentage, and bar chart, wherever applicable. The cumulative scores of knowledge, attitude and practice sections were categorized into categories by using 80% of the total scores as a demarcation point for ‘Poor’ and ‘Good’ scores following existing literature (Harapan et al., 2020; Hasan et al., 2023). While this approach facilitates comparability across studies, it is acknowledged that dichotomisation of continuous scores introduces information loss and potential misclassification. The logistic regression findings are therefore dependent on these threshold definitions, and results should be interpreted accordingly. Sensitivity analyses using continuous KAP scores were not performed but are recommended in future work to assess the robustness of these findings.
Scores of 8 and above out of 10 in knowledge were categorized as ‘Good Knowledge’, and scores below 8 belonged to the ‘Poor Knowledge’ category. Similarly, a score of 24 (80% of 30) was the cutoff point for attitude (Poor Attitude > 24 ≥Good Attitude), and 4 (80% of 5) was the cutoff point for practice (Poor Practice > 4 ≥ Good Practice). Multiple logistic regression analyses were performed to identify factors associated with Knowledge, Attitude, and Practice (any degree), and covariates were selected from socio-demographic and general information. Variables included in the multivariable models were selected based on prior literature and conceptual considerations. Sociodemographic factors (age, sex, marital status), institutional characteristics (type of institution, curriculum, study year), and educational exposure (ABR training) were included as they represent theoretical constructs linked to knowledge acquisition and practice. During model building, collinearity was assessed and the variable ‘In which year antibiotic resistance was taught’ was excluded from multivariable models due to collinearity with other educational exposure variables, as noted in the Results. However, formal assessment of multicollinearity using variance inflation factors and model fit evaluation using the Hosmer–Lemeshow test were not reported in the current analysis; this represents a methodological limitation and is recommended in future studies using similar designs.
The outcomes are presented as adjusted odds ratios (ORs) rounded to three decimal places with corresponding 95% confidence intervals (CIs). Pairwise correlation analysis was done to check the correlation among the outcome variable. Statistical significance was set at p < 0.05, and incomplete responses were not included in the final analyses. The statistical software Stata (version 16) was used for data analysis.
Results
A total of 666 participants were initially included in this study. Two participants were excluded due to incompleteness and then finally analyzed 664 data points. Among the 664 respondents, 280 were from government institutions, and 384 were from private institutions.
Overall, Practice and Attitude scores indicated that more than 80% of the participants, meaning that every four out of five nursing students had good practice and attitude towards Antibiotic Resistance. However, although the majority of students (57.9%) had good knowledge, it was lower than the overall practice and attitude scores, which is apparent in Figure 1. Percent distribution of respondents across knowledge, attitude and practice categories
Frequency Distribution of Sociodemographic Variables Across Knowledge, Attitude, and Practice Categories

The current investigation revealed that a significant proportion of participants, specifically those aged ≤20 years (94.92%), had a favorable attitude regarding antibiotic resistance. Similarly, female individuals (84.27%) showed a more favorable attitude toward antibiotic resistance than their counterparts (78.48%). Most participants from private institutions (90.63%), those with diplomas (87.32%), third-year students (89.12%), those who had used antibiotics within the previous month (94.55%), and those who were not educated about antibiotic resistance (87.95%) showed more favourable attitudes than their respective counterparts (Table 1).
The majority of the participants were 22 years (90.82%), male responders (87.34%), private candidates (85.90%), and B.Sc. Nursing students (84.52%) reported good practices regarding antibiotic resistance. Similarly, those who had taken antibiotics in the previous year (91.39%) and who had not been educated about antibiotic resistance (91.68%) also reported good practices (Table 1).
Pairwise Correlation of Total Knowledge, Attitude, and Practice Scores

aPearson correlation coefficients (r),
bp-values.
Association Between Sociodemographic Variables and Knowledge, Attitude, and Practice
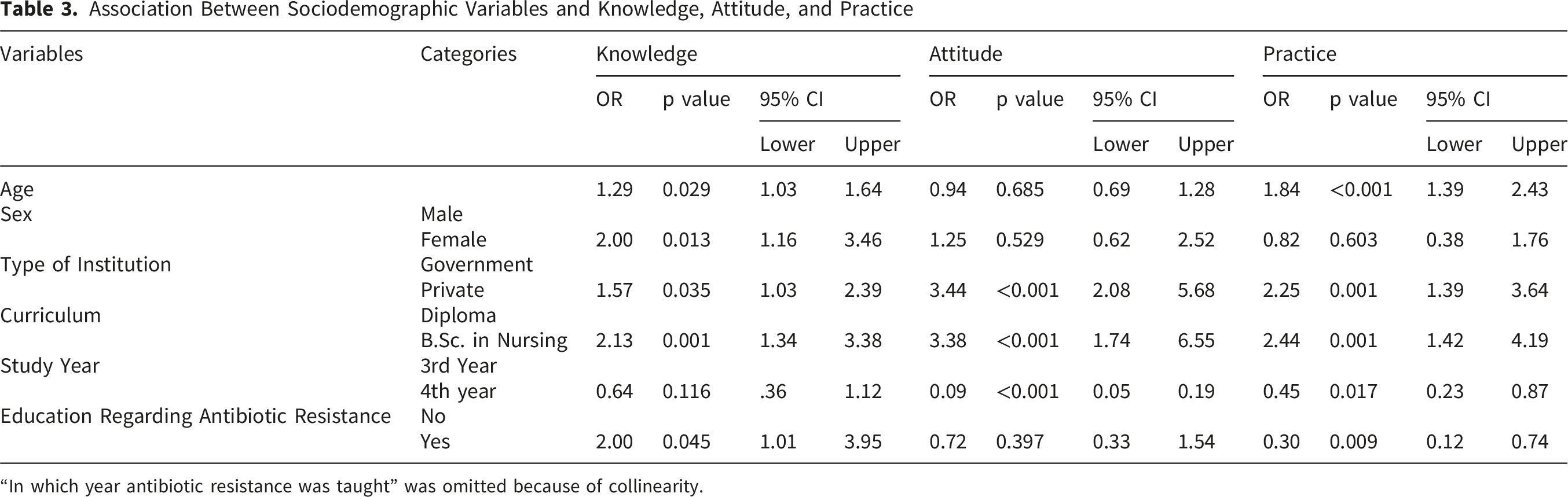
“In which year antibiotic resistance was taught” was omitted because of collinearity.
Discussion
Healthcare workers can play a significant role in the prevention of antibiotic resistance. This study examined nursing students’ knowledge, attitude, and practice related to antibiotic resistance. The findings indicated that the majority of nursing students demonstrated good attitudes and practices in relation to antibiotic use, with knowledge about antibiotic resistance slightly lagging behind. Older age, female gender, enrollment in private institutions, and pursuing a bachelor’s degree in nursing were associated with better knowledge, attitude, and practice. In this study of 664 nursing students, over four-fifths showed good attitudes and practices towards antibiotic resistance, while knowledge was lower at 57.9%. Female students, those in private institutions, and those enrolled in BSc programmes were associated with higher odds of good KAP, whereas fourth-year students showed lower odds of reporting good attitudes and practices compared with third-year students. Knowledge showed a weak but significant positive correlation with both attitude and practice.
More than half of the students in this study displayed good knowledge of antibiotic resistance. Similarly, in a study conducted in Nigeria on similar premises, 64.7% of participants demonstrated good knowledge of antibiotic use and resistance (Okedo-Alex et al., 2019). Another study conducted in Kuwait reported that less than half (47%) of the study participants had good knowledge of Antibiotic Resistance among the general public (Awad & Aboud, 2015). Students pursuing education related to medical science, are usually well-informed about antibiotic usage and resistance compared to other faculties, as reported in existing literature (Dopelt et al., 2023; Nogueira-Uzal et al., 2020; Prigitano et al., 2018; Sakr et al., 2020; Zulu et al., 2020).
In this study, significant associations were observed between age and levels of knowledge and practice regarding antibiotic resistance through multivariable regression analysis. Interestingly, while age was associated with knowledge and practice, no such correlation was found with attitudes. Similar findings in various countries support the age-knowledge link, while studies in Lebanon and Iraq did not report an age-knowledge association (Al-Salih et al., 2019; Guo et al., 2021; Jamhour et al., 2017). As an individual gets exposed to more sources of information with the passage of time, the knowledge level is expected to increase. Besides, senior nursing students are likely to get more exposure to antibiotic usage and information about resistance. Hence, a better knowledge level is likely among the higher age groups. Still, students before the academic introduction of antibiotic resistance might lack exposure to antibiotic-related education, impacting their performance in knowledge, attitude, and practice, and after the completion of education, may face the risk of knowledge attenuation due to a lack of revision or practice, potentially influencing their retention of antibiotic-related information.
Contrary to the association between age and practice found in the multivariable analysis, a Jordanian study conducted among pharmacy students did not find any association between age and practice level (Al-Qerem et al., 2022). Additionally, it highlighted a negative age-attitude connection, not observed among the nursing students in this study. These variations could be explained by the differences in study population, region, curriculum, and question sets used to assess attitude.
While study year showed a significant inverse association with attitude and practice in multivariable analysis, no significant association was observed between study year and knowledge of antibiotic resistance. Similarly, an Indian study showed satisfactory awareness of antibiotic resistance with advancing study years, but unsatisfactory attitudes and practices (Sobierajski et al., 2021). In contrast, a study among undergraduate medical students in Nepal reported opposing findings, emphasizing better practice among senior students, but no associations between study years with knowledge and attitude (Reena & Ittyachen, 2022). On the other hand, previous studies consistently highlighted higher knowledge levels regarding antibiotic resistance among senior students (Chaurasia et al., 2020; Jamhour et al., 2017; Kanneppady et al., 2019; Nogueira-Uzal et al., 2020; Prigitano et al., 2018). Therefore, the findings appear to vary across regions and participant groups. However, the diminishing attitude and practice during senior years among the participants of this study warrant an investigation into the underlying causes. As senior nursing students spend more time in hospital settings for hands-on learning, a better attitude and practice are expected. However, the prevailing practice regarding antibiotics in hospitals may be associated with less favourable attitudes and practices among these young learners. A pervasive and irrational pattern of antibiotic prescription in tertiary care hospitals suggests the practice to be poor in relation to antibiotic resistance (Datta et al., 2016). Recognizing the need for continual educational interventions, some authors advocated mandatory educational interventions across all phases of the undergraduate medical curriculum (Reena & Ittyachen, 2022).
Interestingly, female nursing students displayed higher commendable knowledge than their male counterparts (59.54% vs. 50.00%), consistent with a study conducted in UAE (Jairoun et al., 2019). After adjustment for other factors, female nursing students had twice the odds of possessing good knowledge regarding antibiotic resistance. However, no discernible associations were found between gender and attitudes or practices. This finding is also consistent with a Swedish study, where compared to female respondents, male respondents were more likely to be “Uncommitted” rather than to exhibit a “suitable restrictive attitude” about the use of antibiotics and their side effects (Vallin et al., 2016). However, studies have reported varied associations between sex and Knowledge, Attitude, and Practice (KAP) regarding antibiotic resistance (Jairoun et al., 2019). However, there are a few studies that did not find any associations (Jainlabdin et al., 2021).
Institutional categorization (government or private) and curriculum structure emerged as significantly associated factors across all three domains concerning Antibiotic Resistance (ABR). A study across different universities revealed varying levels of Knowledge, Attitude, and Practice (KAP) concerning AMR, indicating differences among institutions (Higuita-Gutiérrez et al., 2020). In principle, exposure to a variety of content regarding antibiotic resistance should positively enhance KAP among healthcare students. The BSc nursing curriculum is more intensive (4 years) than diploma nursing (3 years), enabling extended training on medical knowledge and practice among the former students. This structural difference may partly account for the observed KAP differences between BSc and diploma students in this study. Along this line of thought, some authors have recommended curriculum modifications to enhance knowledge, attitudes, and practices related to antibiotic resistance (Rábano-Blanco et al., 2019). On the other hand, private institutions are more likely to maintain quality education and training to keep their reputation in check compared to government institutions explaining the good KAP regarding antibiotic resistance among their nursing students (Climer et al., 2025). These differences may also be influenced by variations in faculty qualifications, the intensity of curricula, and the extent of structured clinical exposure, which are often more systematically emphasised in private institutions compared to government ones.
A notable association between antibiotic resistance education on the knowledge and practice level of nursing students was also found in this study. Previous experience in research or education and repeated training might improve KAP regarding antibiotic use and resistance emphasizing the need of continual education in this matter (Higuita-Gutiérrez et al., 2020; Mersha, 2018).
While correlation analyses revealed weak but significant positive relationships between knowledge and both attitude and practice, these were interpreted only as descriptive associations and not as causal effects, given the limitations of correlation methods. It is important to note that although the correlations between knowledge and attitude (r = 0.18) and between knowledge and practice (r = 0.09) were statistically significant, both are weak by conventional standards. In large samples such as this (n = 664), even trivially small correlations can achieve statistical significance. The practical magnitude of these associations is therefore limited, and they should not be interpreted as evidence that knowledge meaningfully drives attitude or practice change. This finding is consistent with broader evidence that the KAP relationship in antibiotic stewardship is attenuated by contextual, institutional, and behavioural factors beyond individual knowledge (Jahromi et al., 2025). These results reinforce the need for multi-component educational interventions that target behaviour change directly, rather than assuming that knowledge acquisition alone will translate into improved practice. Prior literature suggests that higher knowledge levels are associated with more favourable attitudes and practices, though the direction and strength of these relationships vary considerably across settings. (Holbrook et al., 2005; Waseem et al., 2019).
The study provides novel insights into the complex dynamics of antibiotic resistance awareness. This study's focus on a specific demographic, such as nursing students, brings to light knowledge gaps pertinent to this unique population, making it a novel approach, as similar studies have never been conducted on nursing students in Bangladesh. Moreover, nursing students are future nurses, future stewards of the accurate use of antibiotics, and preventers of misuse and AMR. This study can also serve as a baseline to highlight the multifactorial interplay between socio-demographic factors, academy-related factors, and knowledge, attitude, and practice regarding antibiotic resistance. Further studies are required to investigate extensively the current state of knowledge, attitudes, and practices of antibiotic resistance among Bangladesh nursing students in different contexts. These studies should recruit participants from all administrative divisions to maximize generalizability, longitudinal study designs to better characterize temporal associations, and attempt to identify reasons for attenuation of attitude and practice observed among the senior students. Practical measures such as case-based discussion, simulation-based education, and interdisciplinary One Health teaching can better prepare nursing students, while future research should include longitudinal follow-up and intervention trials to test educational interventions, assess post-graduation knowledge retention and clinical behaviour, and use objective measures to validate self-reported practices. Second, comparative analyses at government and non-government institutions and between bachelor and diploma programmes within both countries would provide valuable inputs to inform curriculum development and policy interventions. Lastly, although interaction effects (e.g., gender modifying practice) and predicted probabilities (margins analysis) could provide additional insights, these were beyond the scope of the cross-sectional descriptive design and are recommended for future research.
Strength and Limitations
A notable strength of this study is its large sample size which bolsters the statistical reliability of the findings. However, the study has some limitations despite its novelty. Primarily, its cross-sectional design restricts the establishment of causal relationships between age, knowledge, attitude, and practices regarding antibiotic resistance. As the questionnaire relied on self-reported data, particularly in the practice section, there may have been socially desirable responses. The absence of confirmatory factor analysis, and test–retest reliability assessment means the instrument should be regarded as exploratory. The relatively higher levels of reported attitudes and practices, despite only moderate knowledge, may partly reflect social desirability bias in self-reporting, institutional norms that reinforce expected behaviours, or reliance on rote learning that encourages favourable responses without ensuring deep conceptual understanding. Furthermore, the lack of data from all administrative divisions may question the generalizability of the results. However, the robust methodology of this study can mitigate these concerns to a certain extent.
Additional limitations include the limited internal consistency of the adapted instrument, which suggests possible construct heterogeneity and may attenuate regression-based associations. The use of an 80% dichotomisation threshold, while consistent with prior literature, introduces information loss and renders logistic regression findings sensitive to threshold definition. Furthermore, the weak KAP inter-correlations observed are likely partly attributable to statistical artefact at large sample sizes and should not be interpreted as evidence of meaningful construct relationships. Multicollinearity assessment and Hosmer–Lemeshow model fit statistics were not formally reported, and causal inferences cannot be drawn from this cross-sectional design.
Implications for Practice
Our results are indicative of the need for ongoing educational reinforcement regarding antibiotic resistance throughout nursing education, particularly in subsequent years when clinical experience can be vulnerable to inappropriate prescribing behavior. Curricula strengthening with appropriately designed antimicrobial stewardship elements, coupled with targeted interventions in governmental and private institution facilities, might help sustain favorable attitudes and behaviors. Practical measures such as integrating case-based discussion and simulation-based education into clinical curriculums, and interdisciplinary teaching to introduce the One Health philosophy towards antibiotic prescribing, can even more effectively prepare nursing students. Continuous professional development and repeated training opportunities are also essential to ensure that nursing students transition into practice as effective stewards in the fight against antibiotic resistance.
Conclusion
This study serves as a baseline for understanding knowledge, attitudes, and practices (KAP) levels among Bangladeshi nursing students regarding Antibiotic resistance. Factors like age, gender, institution type, curriculum, and year showed significant associations with KAP of nursing students regarding antibiotic resistance. Correlation between knowledge, attitudes, and practices was also observed in this study which can hint toward the need for continued educational efforts to address antibiotic resistance.
Supplemental Material
Supplemental material - Knowledge, Attitude and Practice of Nursing Students on Antibiotic Use and Resistance in Bangladesh
Supplemental material for Knowledge, Attitude and Practice of Nursing Students on Antibiotic Use and Resistance in Bangladesh by Mehedi Hasan, Md Abdullah Saeed Khan, Mosharop Hossian, Sabrina Yesmin Barsha, Miah Md. Akiful Haque, Jannatul Mawa Joya, Lamisa Rahman, Mohammad Nurunnabi, Tahmina Zerin Mishu, Sabrina Afroz, KM Tanvir, Mohammad Ali Hossain, Md Utba Rashid, Mohammad Lutfor Rahman, Mohammad Hayatun Nabi, and Mohammad Delwer Hossain Hawlader in Sage Open Nursing.
Supplemental Material
Supplemental material - Knowledge, Attitude and Practice of Nursing Students on Antibiotic Use and Resistance in Bangladesh
Supplemental material for Knowledge, Attitude and Practice of Nursing Students on Antibiotic Use and Resistance in Bangladesh by Mehedi Hasan, Md Abdullah Saeed Khan, Mosharop Hossian, Sabrina Yesmin Barsha, Miah Md. Akiful Haque, Jannatul Mawa Joya, Lamisa Rahman, Mohammad Nurunnabi, Tahmina Zerin Mishu, Sabrina Afroz, KM Tanvir, Mohammad Ali Hossain, Md Utba Rashid, Mohammad Lutfor Rahman, Mohammad Hayatun Nabi, and Mohammad Delwer Hossain Hawlader in Sage Open Nursing.
Supplemental Material
Supplemental material - Knowledge, Attitude and Practice of Nursing Students on Antibiotic Use and Resistance in Bangladesh
Supplemental material for Knowledge, Attitude and Practice of Nursing Students on Antibiotic Use and Resistance in Bangladesh by Mehedi Hasan, Md Abdullah Saeed Khan, Mosharop Hossian, Sabrina Yesmin Barsha, Miah Md. Akiful Haque, Jannatul Mawa Joya, Lamisa Rahman, Mohammad Nurunnabi, Tahmina Zerin Mishu, Sabrina Afroz, KM Tanvir, Mohammad Ali Hossain, Md Utba Rashid, Mohammad Lutfor Rahman, Mohammad Hayatun Nabi, and Mohammad Delwer Hossain Hawlader in Sage Open Nursing.
Footnotes
Acknowledgement
We extend our heartfelt appreciation to all the nursing students who generously contributed their time and insights to this study. We are grateful for the cooperation and support received from the healthcare facilities that allowed us to conduct our research on their premises. Additionally, we would like to thank the nursing institutes for their assistance in facilitating the data collection process.
ORCID iDs
Ethical Considerations
Approval was received from the Institutional Review Board (IRB)/Ethical Review Committee (ERC) at North South University for this survey (2024/OR-NSU/IRB/0309). The ethical norms of the 1964 Declaration of Helsinki and its later revisions or comparable ethical criteria were observed, wherever appropriate. Participants’ privacy and data safety were strictly preserved, and access was restricted to personnel involved in data collection and analysis.
Consent to Participate
The objectives of the study and their role in it were explained in detail to the respondents before obtaining their informed written consent. Those who provided consent participated in the study.
Author Contributions
Conceptualization: Khan, M A S; Hossian, M; Hawlader, M D H; Data Curation: Hasan, M; Khan, M A S; Formal Analysis: Hasan, M; Khan, M A S; Investigation: Hasan, M; Joya, J M; Nurunnabi, M; Barsha, S Y; Rahman, L; Mishu, T Z; Afroz, S; Hossain, M A; Rashid, M U; Methodology: Khan, M A S; Nabi, M H; Hawlader, M D H; Project Administration: Rashid, M U; Hossain, M A; Haque, M M A; Hossian, M; Supervision: Rahman, M L; Nabi, M H; Hawlader, M D H; Validation: Khan, M A S; Hossain, M A; Rahman, M L; Nabi, M H; Hawlader, M D H; Visualization: Tanvir, K M; Khan, M A S; Rahman, M L; Writing – Original Draft: Hasan, M; Barsha, S Y; Khan, M A S; Joya, J M; Haque, M M A; Writing – Review & Editing: Khan, M A S; Hossian, M; Rahman, M L; Nabi, M H; Hawlader, M D H; Hasan, M.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data collected and analyzed for this study are not publicly available due to participant confidentiality and institutional restrictions. However, the data are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.