
Abstract
Introduction
The use of telemedicine in palliative care has become an effective tool. Telephone follow-up allows for the anticipation of complications, the resolution of doubts, and the provision of peace of mind. However, case resolution is conditioned by various factors.
Objective
The objective of this study was to analyze the factors influencing the resolution of nurse-led telephone follow-ups of palliative home care patients treated by nurses at the Salud Responde public telemedicine service in Andalusia (Spain).
Methods
A retrospective observational study was conducted that included 44,981 records of requests from palliative home care patients who were treated by nurses at the Salud Responde public telemedicine service during the period between 2012 and 2024. It is important to note the distinction between two profiles: proactive palliative patients, characterised by clinical stability and proactive management of complications through planned follow-up; and reactive palliative patients, who are more clinically complex and initiate contact with the service on an unscheduled basis.
The study variables are grouped into the following blocks: sociodemographic data, temporal data and clinical data on the patient, reflecting the type of resolution of each consultation. Machine learning techniques were applied, using the Random Forest model to predict the type of resolution of each call, which differentiated between health advice and referral to other levels of care.
Results
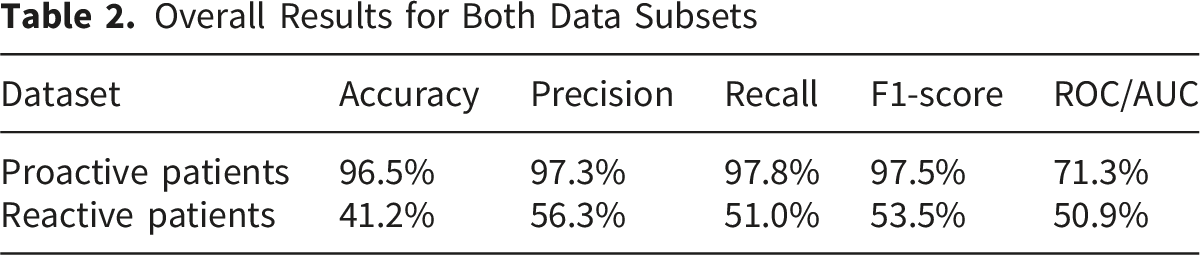
Of the records included, 74.44% corresponded to proactive patients and 25.56% to reactive patients. The model established a set of rules that achieved high accuracy in proactive patients (96.5%), but low accuracy in reactive ones (41.2%). In proactive patients, healthcare advice stands out as the resolution of cases, while the factors most associated with resolution were clinical status, age, respiratory distress and conspiracy of silence.
Conclusion
The resolution of demands raised by palliative home care patients through telephone follow-up is conditioned by various factors. This study describes the criteria that mainly affect the profile of the proactive patient. These findings are relevant for implementing improvements in decision-making and in the organisation of telemedicine, ensuring continuity and quality care.
Introduction/Background
Palliative care (PC) is a fundamental element of the healthcare system, focusing on improving the quality of life of people with advanced diseases and their caregivers through a comprehensive approach. The World Health Organization recognizes PC as a human right; however, there are inequalities between groups of countries in accessing these services based on their income. Each year, it is estimated that more than 56.8 million people need PC. Seventy-eight percent of these people live in low- and middle-income countries, where the availability of such services is limited and resources are more concentrated in high-income countries (World Health Organization, 2022).
To increase accessibility for the population that requires PC, strategies are needed to optimize resources, such as telemedicine. This resource falls within the concept of telehealth, which consists of incorporating information technologies into healthcare for the population (Gajarawala & Pelkowski, 2021).
Telemedicine has become increasingly important as an effective means of providing real-time healthcare through information and communication technologies (Fernández & Mérida Hernández, 2010). It complements face-to-face care, expanding coverage, improving monitoring and health education, while reducing patient anxiety and congestion in healthcare centers, increasing the satisfaction of both patients and their caregivers (Couderc et al., 2023).
Despite advances and the implementation of telemedicine in the field of palliative care, there are few studies on the factors that influence professionals’ decision-making regarding the resolution of cases treated. Identifying these factors provides evidence for optimising telecontinuity programmes for palliative home care patients and, thereby, continuity of care. As such, an exploratory Machine Learning model is presented so that professionals can gather further evidence with which they can further justify palliative care.
Review of Literature
The effectiveness of telemedicine services has been demonstrated in different areas, including urgent and emergency care (Sharifi Kia et al., 2023), mental health services (Hagi et al., 2023), intensive care (Spies et al., 2023), orthopedic and trauma surgery consultations (Zamora Navas et al., 2021), pediatric care (Shah & Badawy, 2021), and the management and control of chronic diseases (Xiao & Han, 2023). A systematic review of the effectiveness of telemedicine versus face-to-face care during the COVID pandemic suggests that both are comparable, highlighting that models for integrating telemedicine with face-to-face care will become increasingly relevant (Hatef et al., 2024). The field of PC has also been the subject of attention from telemedicine (Ghazal et al., 2024).
Multidisciplinary care via telemedicine reduces delays in treatment, improves coordination, and avoids unnecessary referrals, thereby enhancing quality of life, which is the main goal in this area (Daly & Riess, 2016). Similarly, decision-making must follow the values of patients and their families in relation to end-of-life care (Yamamoto et al., 2017). Barriers that may arise during this process can be mitigated by dedicating more time to communication (Roodbeen et al., 2020). Decision-making by professionals working in telemedicine is influenced by stress, potential risks, the time in which they must make the decision, and their knowledge of the cases (Jacobs, 2025).
A recent systematic review focuses on examining the benefits of telemedicine in PC and highlights the need to adopt thoughtful and prudent approaches that consider ethical issues (Krieckemans et al., 2025). In this regard, it is necessary to have an in-depth understanding of how this resource works, in addition to analyzing specific aspects such as the clinical, sociodemographic, or organizational factors that determine whether a follow-up is resolved satisfactorily or, on the contrary, requires referral to other levels of care, an issue to be addressed in this research.
Machine learning methods are a subset of artificial intelligence, focused on the development of algorithms or rules by trial and error from the database provided, useful for obtaining clinical predictions (Brnabic & Hess, 2021). The implementation of automated procedures in this decision-making context could have a positive effect on the early activation of resources; however, this same fact raises ethical questions that remain to be resolved (De Panfilis et al., 2023; Oliveira dos Santos et al., 2022).
The objective of this study was to determine the resolution of telephone follow-up performed by nurses in palliative home care patients served by a public telemedicine service in Andalusia (Spain), as well as to identify the predictive factors associated with this resolution, using a machine learning-based analysis method.
Methods
Design and Sample
A retrospective observational study was conducted based on the records of home-based PC patients treated by the public telemedicine service in the region of Andalusia (Spain), whose data were analyzed using machine learning techniques.
This service, called Salud Responde (Junta de Andalucía, 2025), is a consolidated telemedicine model with multi-channel access that offers remote healthcare to the population. It serves the eight provinces that make up Andalusia and has a population coverage of 8.6 million people (Instituto Nacional de Estadística, 2024). Since 2012, its wide range of services has included telephone follow-up of home-based PC patients, which is carried out by trained nurses who monitor the patients. Its objectives are to detect complications early and provide health advice and, when necessary, refer to those cases that require in-person care.
If the patient shows warning signs that require urgent attention, they are referred to the nearest Emergency Coordination Center. Otherwise, the case is resolved through health advice or referral to a Case Management Nurse at their primary care center.
Follow-up is carried out on two patient profiles. On the one hand, there are proactive palliative patients, characterised by clinical stability and the proactive management of complications through planned monitoring, who are those who receive comprehensive follow-up during the days specified by their primary care physician, through a telephone interview in which the patient and/or primary caregiver are asked about the highlights of the patient’s health, identifying their needs. On the other hand, there are reactive palliative patients, of greater clinical complexity, resulting in unscheduled contact with the service, who are those who contact the service themselves in order to resolve doubts or problems, with the call being transferred to the service’s healthcare staff as a priority.
This study covers the period from June 2012, when this follow-up programme began, to December 2024. All records indicating follow-up of palliative home care patients through the Salud Responde service were included as inclusion criteria. Incomplete records, duplicates, and those that did not correspond to follow-up episodes for this type of patient were excluded. The unit of analysis for this study was healthcare records corresponding to requests from palliative home care patients. Population sampling was used, including the entire target population that met the inclusion criteria during the period covered by this study.
Data Collection
The Salud Responde service provided the research team with an anonymized database in which each record was identified by a randomly assigned sequential code. This database was exported from the Andalusian Health Service’s version 1.2 of the “Palliative Care Management and Support System” application, which records the information collected by nursing staff through a computer system called Avaya. The study period covers from June 2012, when the follow-up began, to December 2024, compiling a total of 44,981 records.
The variables analyzed were age, sex, type of palliative patient (reactive and proactive), pathology or diagnosis (describing the patient’s pathology; if there is more than one pathology, clarifying which one or ones are oncological, as well as indicating the main pathology for which the patient is receiving telephone follow-up), whether the patient is aware of their illness (Aware/Not aware/Unknown), the prognosis (Aware/Not aware/Unknown), the presence of a conspiracy of silence (Absent/Unknown/Present) understood as the situation in which the patient has not been informed of their clinical diagnosis, usually due to a decision made by their family as a measure to protect them from emotional impact (Lemus-Riscanevo et al., 2019) and the severity or complexity of the illness (es). The degree of severity or complexity is determined by the professionals responsible for the patient through categorisation as minimum (need for specific hospital interventions), medium (poorly controlled symptoms) and maximum (severe symptoms); this information is relevant for carrying out appropriate telephone follow-up.
Data was also collected from assessments carried out during telephone follow-ups: patient status (unchanged/improved/worsened), clinical symptoms and problems identified (breathing difficulties, pain, swallowing problems, nausea and vomiting, doubts about the prescribed regimen, presence of new problems identified by the patient) and case resolution (health advice, referral to the Emergency Coordination Centre or a case management nurse). In this context, health advice includes interventions such as health guidance and education, resolving doubts about treatment, emotional support for both patients and family members, as well as recommendations aimed at preventing complications and managing mild symptoms. Additionally, it should be noted that the proactive or reactive profile of the patient conditioned the number of variables. While all variables were collected for proactive patients, for reactive patients, only age, gender, type of pathology, complexity, and the patient’s knowledge of their pathology were collected. The rest of the variables are not collected in the application for this patient profile (Servicio Andaluz de Salud, 2012).
Data Analysis
Data Set and Pre-processing
Initially, the data underwent various pre-processing techniques. The dataset prepared for analysis included 44,981 records. Given that a different amount of information and variables were available for each type of patient, the original dataset was separated into two (proactive and reactive). Subsequently, the data for each of the subsets was analysed individually. 3,613 cases in the proactive subset and 1,807 cases in the reactive subset had more than half of the variables blank. Such examples lacking essential information, such as the pathology that the patient was suffering or whether the patient had received health advice or some other treatment, as well as patients which lacked >50% of all attributes, were removed from both subsets, while the rest of the examples remained unchanged. Additionally, for those patients who had essential information but lacked some particular attributes, the missing data were imputed using the mode of the subset for categorical data and the mean of the subset for numerical data. Other pre-processing techniques were applied to each subset individually, including the selection of characteristics to eliminate all free text fields deemed irrelevant to the clinical context, including geolocation data and date of reviews, and the imputation of missing values according to the previously specified criteria. After applying the pre-processing, the datasets contained 29,447 records of proactive patients and 10,114 of reactive patients, respectively.
Since both datasets were unbalanced, with up to 98% of cases requiring only health advice in the proactive subset and 97% of cases requiring only health advice in the reactive subset, SMOTE (Chawla et al., 2002) was applied to both datasets. SMOTE is an oversampling technique that generates artificial examples by taking values from a given class and creating new cases at intermediate points between the original examples. SMOTE was used so that all classes had the same number of examples, for a total of 13,042 reactive examples and 57,712 proactive examples. Although SMOTE creates artificial examples, potentially introducing new biases and noise by over-generalizing minority classes and misrepresenting data distribution, it takes into account the values of real patients and generates synthetic examples that always remain within the values of real patients, also considering the class corresponding to them. Although it is inevitable that the generation of synthetic data introduces noise, SMOTE does so by minimising it. Additionally, the additional data generated by SMOTE is used only for model training, while the experimentation was carried out using only real data. In the experiment, better results were obtained by applying SMOTE than without it, demonstrating the usefulness of the technique and the absence of bias introduced by its use. To continue, in order to ensure that there was no overfitting to the data, 5-fold stratified cross-validation was used as a training and validation strategy. Consequently, the data were divided into 5 groups, maintaining an equal distribution of all classes. The model was then tested five times, so that in each run, 4 groups were used to train it and the remaining group was used to validate it (Figure 1). Behaviour of the k-fold validation strategy
Classification
In this research, the Random Forest model (Breiman, 2001) was used to extract relevant information from patient data in order to determine the most effective way to treat a given patient based on the information available about them. The Random Forest model is a model that groups together other tree-based algorithms, with each tree being constructed using only a portion of the attributes. After that, the results of each individual tree are combined using a weighted sum or majority vote, so that the most voted result is chosen for each example to be predicted.
Since each tree considers only some attributes and the information is subsequently combined, the algorithm becomes more robust, particularly when compared to the individual trees that give rise to the model. This also allows for partial mitigation of overfitting, as well as other problems that may arise as a result of a large number of attributes.
The model was generated using C4.5 trees (Salzberg, 1994) with a confidence factor of 0.25 and a minimum of 2 objects per leaf node. It was also configured not to use the exact value of the nodes when dividing them, but rather the value that provides the greatest accuracy. The partitioning criterion was the information gain ratio. Finally, during the pruning phase, vertical displacement of subtrees was activated to avoid removing them completely from the model. The model was tested with different numbers of trees, and the best results were obtained using 100 trees. The most relevant rules extracted from the trees are shown in the results section. The hyperparameters provided allow the model used to be fully replicated and were obtained through a series of sequential experiments in which each possible combination of hyperparameters was tested using 50, 70, 90, or 100 trees. The hyperparameters reflected in the text are those that provided the best results.
A C4.5 tree consists of a set of nodes that can advance to other nodes based on the values of certain data attributes. The lowest-level nodes, known as leaf nodes, instead return a label as output. When a new example needs to be predicted, simply follow the node paths based on the attribute values of this new example until a leaf node is reached, which will provide the corresponding label.
The tree is constructed through several iterations of the same algorithm, which takes place in three phases: ● Phase 1: If all or almost all of the elements in a node have the same class or label, the node is considered a leaf node, and the algorithm stops at that node. ● Phase 2: Instead, for each element of the node, all attributes are considered. The attribute with the highest information gain is chosen, and the node is divided into several child nodes. Each child node is defined by threshold values of the chosen attribute, such that the elements of the parent node are distributed among its children. ● Phase 3: Once the complete tree has been constructed by repeating phases 1 and 2, it can be pruned (Venkatesan & Velmurugan, 2015) by removing some nodes, avoiding overfitting and sometimes improving the accuracy of the model.
Metrics
Since accuracy alone may not be sufficient to determine the quality of a model that works with patient diagnoses, multiple metrics will be considered when evaluating the results. Below are a series of basic definitions on which the metrics used were based: ● True Positive (TP): Patients in a target class who are classified correctly. In this case, patients for whom health advice is sufficient, correctly classified. ● True Negative (TN): Patients in any other class who are classified correctly. ● False Positive (FP): Patients in any other class who are incorrectly classified as belonging to the target class. In this case, patients who need transfer or assignment to a nurse but are classified as needing health advice. ● False Negative (FN): Patients in the target class who are classified as any other class. In this case, patients for whom health advice was sufficient and for whom a transfer or assignment to a nurse is predicted.
With these definitions, we can define the following metrics that were used to evaluate the model’s results: ● Accuracy: (TP + TN)/(TP + FP + TN + FN). Accuracy is defined as the proportion of correct predictions. When working with unbalanced datasets, accuracy is not enough, as a high accuracy can be obtained by always predicting the majority class while neglecting the minority class. ● Precision: TP/(TP + FP). Precision can be defined as the fraction of all patients who needed health advice who are correctly classified as such. Class-specific precision implies a low false-positive rate for the class, and as such is key when minimizing false positives. ● Recall: TP/(TP + FN). Recall can be defined as the fraction of patients who have been predicted to need health advice and who actually need it. Class-specific recall implies a low false-negative rate for the class, and as such is key when minimizing false negatives. ● F1 Score: 2 * (Precision * Recall)/(Precision + Recall). The F1 score is defined as the harmonic meaning between precision and recall. Class-specific F1 score represents the balance between class-specific precision and recall.
Ethical Considerations
Favorable opinion obtained from the Andalusian Coordinating Committee for Biomedical Research Ethics (study code: 2103 and communication/application code: SICEIA-2024-002454, approval date: February 5, 2025) as well as the Research and Innovation Coordinating Committee of the 061 Health Emergency Center (approval date: February 20, 2025). Both committees approved the exemption from informed consent for patients, as the data had already been recorded in the information systems of the organisation where this research was conducted. All procedures were carried out in accordance with the principles of the Declaration of Helsinki and current European data protection regulations.
Results
Sample Characteristics
Sample Characteristics

n.a: Not available.
Research Question Results
Overall Results for Both Data Subsets
Detailed Results for Each Data Subset

Proactive Patients
Confusion Matrix for the Subset of Proactive Patients

Relevant Rules for Proactive Patients

Reactive Patients
Confusion Matrix on the Reactive Patient Dataset

As can be seen, the outcomes for reactive patients are considerably worse than for proactive patients. Due to the low results provided by the model, no rules were extracted as they lacked the necessary accuracy, precision and recall to offer relevant knowledge to experts.
Discussion
The objective of this study was to analyse the factors associated with the resolution of telephone follow-ups in palliative home care patients treated by a public telemedicine service. The machine learning model showed promising results in proactive patients, finding that the most influential factors in case resolution were clinical status, age, presence of respiratory distress, pain, and the existence of a conspiracy of silence.
The results obtained show a notable difference in the model’s performance depending on the type of palliative patient. The analysis performed using the machine learning model applied to this research achieved high accuracy values in proactive palliative patients, with a decline in performance observed in reactive palliative patients. This result is justified by the difference in the availability, quantity, and comprehensiveness of the information collected in both groups, with the group of proactive palliative patients achieving greater accuracy in predictions. On the other hand, the lower accuracy in reactive palliative patients may be due to a lack of critical information, given that reactive patients have considerably few variables available due to the nature of their concerns, since they call to receive instructions rather than having detailed follow-ups on their conditions. This may cause the model to lack the information it would obtain from these missing variables, which allows it to correctly determine what action should be taken.
This finding is consistent with the intervention dynamics of the telemedicine service, as it provides differentiated care based on the patient’s profile, which is key to the correct approach to their situation. As for the proactive patient group, the telephone follow-up is planned and routine, and its purpose is to establish continuous monitoring that provides support and accompaniment (Steindal et al., 2020) to both the patient and their family members. This involves more extensive and multidimensional data collection, allowing for the early identification of problems or complications, the detection of emerging needs, and the guidance of clinical decision-making, in line with existing literature (Tieman et al., 2016). With regard to the reactive patient group, contact is made at the initiative of the patient or their family members, generally with the aim of resolving a specific issue. In this situation, the priority is to provide an immediate and specific response to the problem at hand, so postponing the resolution in order to collect more data that is not of interest at that moment makes no clinical sense and adds no value to either the patient experience or the efficiency of care.
In view of the results obtained, it can be seen that health advice is the preferred referral for proactive palliative patients treated by Salud Responde, which is consistent in terms of the effectiveness and efficiency of a telemedicine service. An early PC nursing phone-follow-up service for advanced cancer patients reported 87.6% effectiveness in telephone management, meaning most issues were handled by the nurse without further immediate intervention (Valenti et al., 2023). Similar results were found by Martins & Pinto (2023), who demonstrated that a PC for home patients during COVID-19 solved 92.9% of problems by phone. Teleconsultation could be considered a useful tool for overcoming both geographical and logistical barriers to accessing PC (Mathews et al., 2023).
Based on the results shown in the predictive rules derived from the model, it is evident that there are determining factors that influence the resolution of proactive patient cases, notably the patient’s current condition, respiratory distress, pain, conspiracy of silence, and age. Age is a modulating factor in decision-making, along with severity and respiratory distress, a fact already confirmed in previous research (Santus et al., 2023; Tang et al., 2012).
When the patient reports improvement or no clinically relevant changes but exhibits respiratory symptoms such as dyspnea, the call is forwarded to the Emergency Coordination Center for early diagnostic evaluation by medical personnel, who will determine whether it is necessary to dispatch medical resources to the patient’s home or whether pharmacological treatment is enough.
However, patients with mild symptoms receive health advice because, according to this study, mild symptoms can be resolved through recommendations, with younger patients being prioritized for receiving this advice. A systematic review and meta-analysis of randomized trials (Chair et al., 2024) found that telephone consultation resolved problems related to mild symptoms by only recommendations, and reduced face-to-face doctor visits, without increasing emergency visits, hospitalizations, or mortality. In a multivariable analysis of German on-call service (Hansen et al., 2025), telephone advice was associated with lower age and lower subjective urgency.
In predictive rule number 2, it is observed that if the patient is feeling better or there are no changes in their condition, but there are doubts regarding treatment, the indication would be referral to the Emergency Coordination Center or the Case Management Nurse. In this context nurses of Salud Responde can resolve doubts regarding pharmacological treatments, but they cannot remove or prescribe a new drug. Medication clarifications, dose titration, and prescription issues are a typical cause for non-presentially managed calls (Steindal et al., 2020.) Valenti et al., (2023) found out that medication management (18.9%) was a frequent cause of consultation. For this reason, some teleconsultation programs include different professionals such as pharmacists or physicians for complex medication issues. Valenti et al., (2023) stated that the majority of phone calls were handled by the nurse case manager, 28.1% were handled by a physician and 6.8% by the case manager and physician together. A cross-sectional study that added a pharmacist to a PC telehealth service showed high rates of polypharmacy and inappropriate medications, and telehealth reviews generated many recommendations on deprescribing, symptom control, and medication administration (Chess-Williams et al., 2024).
According to the results of this study, if the patient reports no significant changes that would prevent the continuation of home care, teleconsultation system offers the possibility of providing health advice. However, when a medium or high degree of complexity is detected in a PC context, the call is systematically referred to the CCU, to handle this situation as a priority. A blend approach that combines teleconsultations with face-to-face consultation is the more appropriate approach in PC context. PC face-to-face consultation is crucial for physical examination or new/complex diagnosis, and aid communication with patients and relatives (Morris et al., 2024). Acute life-threatening physiological instability and time-critical complications should be appropriately triggered through PC teleconsultation and referred to CCU.
Strengths and Limitations
One of the main strengths of this study is that, to date, no published evidence has been found, or the existing evidence is limited in terms of follow-up data on palliative home care patients from a public telemedicine service. A large volume of data has been processed thanks to the implementation of machine learning models. In this regard, the technique used in this research has already been successfully tested in other previous studies with large amounts of health case data, demonstrating advantages over traditional statistical analyses (Habehh & Gohel, 2021; Kourou et al., 2021; Rajkomar et al., 2019; Shehab et al., 2022). Due to the way the Random Forest model operates, it can capture both linear and non-linear relationships simultaneously, as well as automatically identifying correlations among multiple variables and attributes. In addition, the Random Forest model does not require homoscedasticity or normality in the analysed data.
This study is not without limitations. The analysis performed using the machine learning model shows that the quantity and quality of the available data are essential for predictive capacity, a fact that could not be controlled in this study as it was based on already available records. Particularly noteworthy are the limitations in reactive patients, which reinforce the need to structure data collection in this type of palliative care patient in a more appropriate and accurate manner in order to obtain results similar to those of the other group. Furthermore, the clear imbalance between types of outcomes required the use of oversampling techniques, although these were mainly applied during model training, and therefore their influence is considered to be minimal. The human factor, given the variability in clinical assessments carried out by nursing staff and the organisational changes that occurred during the study period, may also have influenced the results. Likewise, the telemedicine used by Salud Responde to monitor patients in palliative care is the telephone call, a fast and accessible means of communication for the majority of the population. However, according to a previous study, this method has sensory, cognitive, and functional limitations, which are key points for the use of telemedicine. In addition, according to this same study, older people did not consider telephone consultation to be a medical act, promoting a hybrid approach to consultation, which could be implemented as an improvement to this service (Khanassov et al., 2024).
Furthermore, it should be noted that the study period includes the year’s corresponding to the COVID-19 pandemic, which created a scenario that changed access to face-to-face care, healthcare organisation and service use. Therefore, this situation may have influenced case resolution by increasing the selection of health advice and giving rise to possible bias in the results obtained.
From an ethical perspective, the use of artificial intelligence models raises considerations given the vulnerability of the population under study. Their capacity for systematic analysis, together with the handling of large volumes of data, makes it possible to reduce interpretative variability, which justifies their use in this study. It should be clarified that, in this work, these techniques have been employed for research purposes, using an anonymised database and through an observational approach that guarantees the principles of patient autonomy, beneficence, and non-maleficence.
On the other hand, it should be considered that the model predicts clinical decisions made by nursing professionals in a telephone follow-up scenario, and not objective clinical outcomes such as hospital admissions. Therefore, it may reflect patterns of current clinical practice and decision-making processes specific to the care context, rather than strictly identifying independent clinical risks.
Furthermore, the possibility of selection bias due to the exclusion of 12% of records because they were incomplete should be acknowledged. This may be because documentation can be compromised in situations of high care workload and/or urgent intervention contexts.
Finally, the findings should be interpreted with caution. The database used faithfully reflects real clinical practice within a single public telemedicine service with its own specific characteristics, which limits the generalisability of the results to other contexts; therefore, it will be necessary to validate the model in other populations and settings in order to confirm its applicability. As such, the model should be used in an exploratory manner to further assist medical professionals when making decisions but should never fully replace such a professional in a confirmatory manner.
Implications for Practice and Research
The results of this study confirm the importance of health advice in telemedicine practice. From a nursing perspective, these findings demonstrate the role of nurses as a central pillar in managing the follow-up of palliative patients. Nursing professionals are responsible for both the initial clinical assessment and for identifying and anticipating warning signs, and they hold the principal decision-making role in this model of care. The identification of a majority pattern of health advice in the analysed data lays the foundations for promoting its standardisation in the field of telemedicine, which implies training staff in this intervention. Additionally, the predictive rules derived from the Artificial Intelligence model used in this research represent potential in the design of clinical practice guidelines, action protocols, and support algorithms for decision-making in this healthcare context. The clinical rules derived from the model may serve as guidance and/or support for professionals in decision-making during the follow-up of these patients and could be implemented in real clinical practice through telephone triage, telecare systems, or even within the same follow-up recording application in order to introduce improvements. Furthermore, these results highlight the need to strengthen the training of nursing professionals in competences related to telemedicine, such as therapeutic communication and/or remote patient assessment, facilitating both consistency and standardisation in care. In this way, the identification of cases that can be resolved through health advice and those requiring referrals is streamlined, the quality of initial advice can be automated or improved, care pathways can be optimised, and uniformity of criteria can be ensured, thereby reducing variability and improving efficiency in the management of large volumes of consultations.
In relation to the above, it should be noted that telemedicine also influences the subjective experience of both the patient and their family members, with a positive increase in the perception of healthcare accessibility and emotional support (Haydon et al., 2025). This service should be offered as a complement and not as the only care option, especially in palliative patients (López Arias et al., 2021), thus contributing to the assessment of the different needs of patients and facilitating the possibility of care from home, which results in a reduction in long-term hospital admissions (Ayala-Salinas et al., 2023).
The implementation of predictive models in healthcare practice contributes to strengthening models of care led by nursing professionals, while also reinforcing the role of these professionals as essential to the continuity and quality of care for palliative patients.
With regard to future lines of research, the findings of this study show various possibilities for development. It would be necessary to improve the quality and completeness of the data collected, especially in the reactive palliative profile, in order to optimise the predictive capacity of the models. In addition, future research could incorporate new clinical and organisational variables, together with the use of evaluation metrics, with the aim of refining decision-support tools in telemedicine settings. Finally, it would be relevant to analyse the impact of incorporating these models into real clinical practice, thereby evaluating system efficiency and patient health outcomes.
Conclusion
This study has demonstrated promising results when applying machine learning models to predict call resolution in the context of telemedicine applied to PC, especially in the group of proactive patients. The results confirm that health advice is the preferred intervention in resolving cases, in addition to identifying the main predictive factors that influence referral, specifically clinical status, age, respiratory distress and conspiracy of silence.
Footnotes
Acknowledgments
The authors gratefully acknowledge the “Centro de Emergencias Sanitarias” and, in particular, the “Salud Responde” service for their collaboration in data collection, and Maylene Cotto – Andino for the official translation work of this article into English.
Ethical Considerations
This study adhered to the guidelines on research as per the Declaration of Helsinki regarding research on human subjects. Ethical clearance certificates were obtained from the “Comité Coordinador de Ética de la Investigación Biomédica de Andalucía” n° “SICEIA-2024-002454”. Permission was obtained from the “Comité de Investigación del Centro de Emergencias Sanitarias de Andalucía (CES-061)”.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.