
Abstract
Background
Nurses working in intensive care units (ICUs) experience high work demands that pose significant challenges to maintaining work–life balance.
Aim
This study aimed to explore barriers to, and coping strategies for, achieving work–life balance among ICU nurses.
Methods
A sequential exploratory mixed methods design was employed. In Phase I, a descriptive exploratory qualitative approach was used, and in Phase II, a descriptive cross-sectional design was adopted. Integration of qualitative and quantitative findings was conducted during the interpretation stage.
Results
Both qualitative and quantitative findings consistently indicate that caregiving responsibilities substantially increase work–life conflict. Achieving work–life balance among nurses was particularly challenging, with most reporting difficulties managing professional and family responsibilities. These challenges led to stress and reduced personal time, whereas strong support systems, including workplace flexibility and family support, were essential for improving work–life balance. Significant associations with medium effect sizes were identified for age (p = 0.01), gender (p = 0.02), and income (p = 0.04), indicating that personal characteristics influence how ICU nurses manage work and family demands. Unresolved emotional stress directly affected work engagement and motivation. Organizational constraints emerged as key structural barriers to work–life balance, with financial factors further intensifying stress and limiting nurses’ ability to manage competing demands. Social and organizational support systems acted as protective factors, mitigating stress and enhancing nurses’ ability to sustain demanding ICU roles.
Conclusion
ICU nurses face substantial barriers to achieving work–life balance. Organizational support is crucial for promoting nurses’ well-being and sustaining quality patient care. The generalizability of these findings is limited due to the use of non-probability sampling and data collection from a single tertiary care center; therefore, results should be interpreted with caution when applied to other settings or populations.
Introduction
Nursing, historically considered a vocation, has long been associated with an image of selflessness and caring, often exemplified by Florence Nightingale in the nineteenth century (Currie & Carr-Hill, 2013Currie & Carr‐Hill, 2013). Traditionally, nurses were viewed as trained caregivers and continue to constitute the largest segment of the workforce in healthcare systems (Currie & Carr-Hill, 2013Currie & Carr‐Hill, 2013). Over time, the profession has evolved significantly; however, nurses continue to face numerous challenges, including heavy workloads, long working hours, sleep disturbances, limited autonomy, staff shortages, and mental stress resulting from the continuous care of sick and dying patients (Saedpanah et al., 2022). These factors negatively impact physical and mental health, ultimately affecting nurses’ overall performance (Labrague, Nwafor, & Tsaras, 2020Labrague et al., 2020). Previous studies have reported that 30% to 70% of nurses experience work-related stress (Feleke et al., 2025).
Nurses working in intensive care units (ICUs) encounter a range of stressors that are patient-related, interpersonal, or organizational (Hao et al., 2020). ICU nurses experience higher levels of continuous stress than those in general wards due to frequent exposure to critically ill patients and complex procedures (Hao et al., 2020; Saravanan et al., 2023). Interactions with patients’ families and witnessing their suffering further contribute to the emotional burden (Kaushik et al., 2021; Şanlıtürk et al., 2021). In ICU settings, heavy workloads, long shifts, and high patient-to-nurse ratios are consistently associated with perceived stress (Şanlıtürk et al., 2021). Inadequate salaries and limited resources further contribute to strain and dissatisfaction (Kaushik et al., 2021; Şanlıtürk et al., 2021). These stressors can result in adverse outcomes, including physical health issues such as musculoskeletal, gastrointestinal, and cardiovascular disorders, as well as psychological distress and challenges in personal and family life (Saedpanah et al., 2022). Collectively, these factors negatively affect overall nursing performance (Khamisa et al., 2015).
Nurses with better work–life balance experience lower mental strain, reduced burnout, and greater job satisfaction (Widayana, Agustina, & Mediawati, 2025Widayana et al., 2025). Evidence shows that nurses who maintain a healthy balance between professional and personal roles report higher well-being, improved mental health, and greater overall job satisfaction (Zhang et al., 2024). A scoping review across 12 countries noted that 24-hour shift systems for nurses were associated with lower quality of life, reduced job satisfaction, and increased mental exhaustion (Widayana, Agustina, & Mediawati, 2025Widayana et al., 2025). Given that nurses comprise over half of the global healthcare workforce, improving work–life balance is a key strategy for protecting nurses’ well-being, stabilizing the workforce, and maintaining high-quality patient care (AbdELhay et al., 2025).
Review of Literature
Nurses face numerous challenges in maintaining work–life balance. Emphasizing self-care without addressing organizational issues such as staffing shortages, overtime work, and unsafe workloads limits nurses’ capacity to achieve sustainable work–life balance (Mullen, 2015). Conversely, factors such as adequate income, family support, supportive organizational policies, and manageable working hours play a crucial role in maintaining this balance (Widayana, Agustina, & Mediawati, 2025Widayana et al., 2025; Sarla and Sandhu, 2024). Married female nurses, especially in low- or middle-income settings, experience additional barriers, including difficulties in time management due to multitasking between household and clinical responsibilities, childcare, and persistent gendered expectations. These factors result in a “double burden” of paid and unpaid work (Sellahewa & Arachchi, 2023).
Work–life balance is also strongly associated with employee dissatisfaction and the reciprocal negative effects of work on family and family on work (Rony, Numan, & Alamgir, 2023). A strong culture of self-sacrifice and loyalty to patients and families often normalizes long working hours and missed family time as indicators of being a “good nurse” frequently at the expense of personal well-being (Ong et al., 2024). A cross-sectional study of nurses in Jordan found that demographic and occupational factors significantly influenced work–life balance, job satisfaction, and burnout. Higher education was associated with better work–life balance; however, many nurses reported that job demands negatively affected family life. Notably, nurses working more than 50 hours per week reported higher work–life balance, but job satisfaction remained moderate, and work-related burnout was prevalent, highlighting the need for strategies to improve nurses’ well-being and professional engagement (Abuhammad et al., 2025).
Additional research has examined the relationship between work environment factors and professional quality of life among ICU nurses, focusing on burnout, compassion satisfaction, and secondary traumatic stress. The study found that most nurses reported average levels of compassion satisfaction, burnout, and secondary traumatic stress. A moderately positive practice environment was significantly associated with lower burnout and higher compassion satisfaction. Overall, ICU nurses viewed their work environment positively; however, targeted interventions are needed to reduce burnout and enhance professional well-being (Ayed et al., 2024).
Similarly, a study of 233 NICU nurses in the West Bank found that most reported average compassion satisfaction, burnout, and secondary traumatic stress, with a moderately favorable practice environment. Positive work environments were strongly associated with higher compassion satisfaction and lower burnout and secondary traumatic stress. Enhancing staffing, resources, nurse–physician collaboration, and emotional support was deemed essential for improving professional quality of life (Batran et al., 2025). Maintaining nurses’ work–life balance is also essential for improving organizational productivity, quality of care, and positive clinical outcomes (Rony, Numan, & Alamgir, 2023).
Nurses employ a range of coping strategies to protect their well-being and maintain work–life balance. These strategies include setting clear boundaries between work and home, seeking support from colleagues, engaging in open communication, and participating in restorative activities (Poku et al., 2023). Evidence consistently identifies social support from family, friends, colleagues, and supervisors as a key factor in helping nurses cope with stress and maintain a better quality of life (Kowitlawkul et al., 2019). Cross-sectional studies and scoping reviews have also identified physical exercise, self-care practices, and mindfulness-based stress reduction techniques as effective strategies for sustaining resilience in high-stress nursing roles (Setiawan & Susanto, 2025; Widayana, Agustina, & Mediawati, 2025Widayana et al., 2025). Addressing stressors and regulating emotions constructively has been associated with lower burnout, whereas avoidant coping strategies are linked to poorer outcomes (Eysa et al., 2025).
Work–life balance remains a widespread concern among nurses, contributing to high levels of stress, burnout, and reduced job satisfaction, ultimately affecting the quality of patient care (Feleke et al., 2025; Smith & Lee, 2022). Although previous studies have predominantly focused on work-related stress or burnout, few have examined organizational barriers and coping strategies among ICU nurses, particularly in low- and middle-income countries. Furthermore, most studies rely solely on quantitative or qualitative methods, limiting a comprehensive understanding of how organizational, personal, and social factors interact to influence work–life balance. To address this gap, the present sequential exploratory mixed methods study aims to comprehensively examine work–life balance among ICU staff nurses in a tertiary care center. By integrating qualitative insights with quantitative findings, this study seeks to provide a nuanced understanding of work–life balance among nurses and inform nursing administration, hospital management, and policymakers about specific strategies to improve nurses’ well-being, promote a sustainable work environment, and ultimately support high-quality patient care. The study adopts the Job Demands–Resources (JD–R) model (Bakker & Demerouti, 2007) to interpret barriers and coping strategies.
Methods
The reporting of this study followed the Good Reporting of a Mixed Methods Study (GRAMMS) checklist, which provides guidance for the transparent and rigorous reporting of mixed methods research, including the integration of qualitative and quantitative findings.
Research Approach and Design
A sequential exploratory mixed methods research design was used. In Phase I, a descriptive exploratory qualitative approach was employed to collect in-depth information about the barriers to, and coping strategies for, maintaining work–life balance among ICU nurses. In Phase II, a descriptive cross-sectional research design was used, with qualitative findings translated into a structured dichotomous questionnaire to assess work–life balance. Integration of qualitative and quantitative data occurred during the interpretation stage. The study was conducted from April 2025 to May 2025.
Study Setting
The study was conducted among staff nurses working in ICUs at a tertiary care center in Tamil Nadu, India. The hospital employs 725 nurses and provides advanced medical care for complex health conditions, including specialized surgeries, intensive care, and organ transplants. Equipped with expert specialists and advanced technology, the hospital offers a controlled environment suitable for conducting research due to its large nursing workforce, diverse departments, and adequate patient load.
Population
Sample Size and Sampling Technique
n = required sample size Z = 1.96 (standard normal deviate at 95% confidence level) p = 0.565 (estimated prevalence of work–life imbalance) q = 1 − p = 0.435 d = 0.10 (allowable error)

Substituting the values:



Thus, the minimum required sample size was 94 ICU staff nurses. To account for a possible 10% non-response or incomplete data, the sample size was adjusted as follows:
Adjusted sample size = 94 + 10% of 94
Adjusted sample size = 94 + 9.4 ≈ 104
The final sample size for the quantitative component was therefore 104 ICU nurses.
Inclusion and Exclusion Criteria
The study included both male and female staff nurses working in the ICUs. Staff nurses with a minimum of six months of ICU experience who were willing to participate, provide informed consent, and communicate effectively in Tamil or English were included in the study. Nurses on long-term leave, maternity leave, or unwilling/unable to participate in interviews were excluded from the study.
Description and Interpretation of the Study Instrument
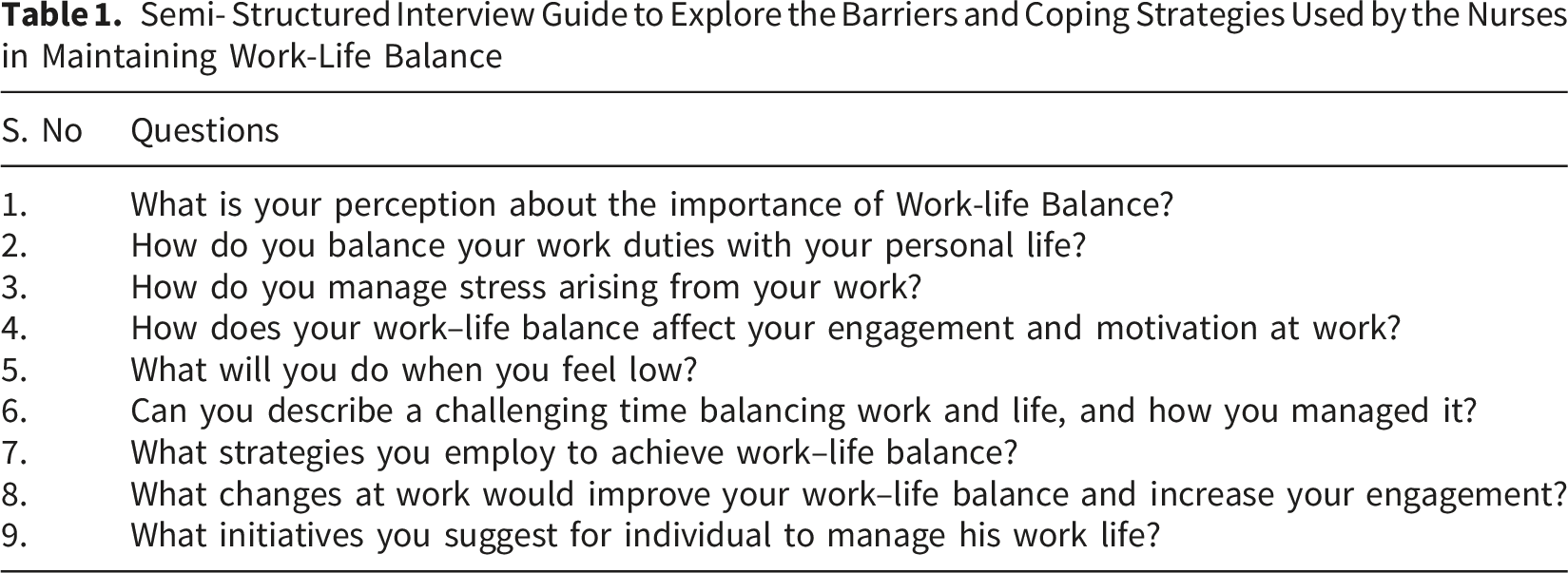
Semi- Structured Interview Guide to Explore the Barriers and Coping Strategies Used by the Nurses in Maintaining Work-Life Balance
Reliability and Validity of the Tool
Content validity was established through review by eight nursing education experts. A pilot study, conducted with 11 ICU nurses (10% of the sample), assessed reliability. Cronbach’s alpha was 0.89, indicating strong internal consistency.
Data Collection Procedure
Ethical Considerations
The study adhered to the Declaration of Helsinki. Written permission was obtained from the Nursing Directorate. Participants were fully informed about study procedures, provided written consent, and could withdraw at any time without penalty. No identifying information was collected. Audio recording of the interviews was conducted with consent. Professional boundaries and culturally appropriate communication were maintained throughout the study. Reflexive journals were used to enhance transparency and credibility. The collected data were stored in a password-protected file under the custody of the principal investigator.
Data Analysis Procedure
Data Integrity and Trustworthiness
The study findings accurately represent the nurses’ experiences and are reported honestly. All data were entered, analyzed, and presented transparently, without manipulation to support desired outcomes.
Results
Table 1 outlines the semi-structured interview guide used to explore nurses’ barriers to, and coping strategies related to, work–life balance.
Demographic Characteristics of the Participants
Frequency and Percentage Distribution of Demographic Variables of Nurses

Participants primarily belonged to nuclear families, especially in Phase II, suggesting limited access to extended family support. Most nurses held a Bachelor of Science in Nursing degree, indicating a well-qualified sample. The Qualitative Phase included nurses with both minimal and extensive experience, whereas the Quantitative Phase largely consisted of nurses with less than one year of experience. Long working hours were commonly reported, particularly among qualitative participants, highlighting the demanding nature of ICU work.
Phase I: Qualitative Phase
Emergent Themes
Themes and subthemes related to barriers and coping strategies adopted by the nurses are presented below.
Theme 1: Challenges With Balancing Work and Life
Theme 2: Coping Strategies
Theme 3: Barriers in Institutions
Theme 4: Effects of Work Engagement and Motivation
Theme 5: Proposed Solutions
Phase II: Quantitative Phase
Outcome Measures
Work-Life Balance Among Nurses N=104

Association Between Work–Life Balance Among Nurses and Demographic Variables N = 104

Integrated Mixed Methods Results
Joint Displays of Mixed Methods Results

Themes of emotional spillover and motivation drain further illustrated how ICU-related stress extends into personal life, reducing emotional energy, work engagement, and intrinsic motivation. Correspondingly, 59.6% of participants reported experiencing stress at work due to family responsibilities, and an equal proportion indicated that work interfered with personal and family relationships. These findings clarify the quantitative trends, suggesting that unresolved emotional stress negatively affects work engagement and motivation, often resulting in emotional exhaustion rather than professional fulfillment.
Institutional barriers, including staffing shortages and rigid scheduling, emerged as significant challenges. These constraints contribute to overtime work, reduced autonomy, and limited recovery time. Consistent with these findings, 69.2% of participants reported insufficient time for family or household responsibilities due to work demands. Income was significantly associated with multiple work–life balance challenges (p < .05), including stress, time constraints, and prioritization of household responsibilities over professional duties. These results highlight organizational constraints as key structural barriers, with financial factors further exacerbating stress and limiting nurses’ ability to manage competing demands.
Key coping strategies identified in the Qualitative Phase, such as self-care practices (such as yoga and exercise) and social support from family and colleagues, were reinforced by quantitative findings. A total of 79.8% of participants reported receiving family support, and 78.8% indicated that flexible work hours and workplace childcare would improve work–life balance. Together, these findings suggest that social and organizational support systems function as protective factors that mitigate stress and enhance nurses’ capacity to sustain demanding ICU roles.
Finally, nurses demonstrated a strong orientation toward family responsibilities, often prioritizing household needs during periods of emotional or physical exhaustion. A total of 42.3 % reported prioritizing family over work during conflicts. Income significantly influenced this prioritization (p = .045), reflecting a value-based coping approach in which nurses consciously prioritize family well-being when faced with competing professional and personal demands.
Discussion
This sequential exploratory mixed methods study provides a comprehensive understanding of the barriers, coping strategies, and work engagement outcomes related to work–life balance among ICU nurses in a tertiary care setting. By integrating qualitative and quantitative findings, the study highlights how individual, organizational, and sociocultural factors collectively influence nurses’ ability to balance professional and personal responsibilities in high-intensity clinical environments.
The findings consistently indicate that caregiving responsibilities substantially increase work–life conflict, particularly among nurses in specific age groups. Qualitative insights further explain these quantitative trends, demonstrating that unresolved emotional stress negatively affects work engagement and motivation, often leaving nurses in a state of emotional exhaustion rather than professional fulfillment. Organizational constraints emerged as key structural barriers to work–life balance, with financial factors further intensifying stress and limiting nurses’ ability to manage competing demands. In contrast, social and organizational support systems were identified as protective factors that mitigate stress and enhance nurses’ capacity to sustain demanding ICU roles.
Previous studies support these findings, indicating that nurses with dependent children and greater family responsibilities report poorer work–life balance (Gribben & Semple, 2021). Similarly, studies among Spanish nurses have shown that having children increases work–family conflict, particularly when combined with rotating shifts (Jover et al., 2025). Limited access to childcare further exacerbates this burden (Alazzam et al., 2017). Additionally, rotating shifts have been associated with higher emotional exhaustion, poor sleep quality, and increased burnout compared with fixed schedules (Al-Hammouri et al., 2025; Dhaini et al., 2018). Consistent with these findings, the present study demonstrates that caregiving responsibilities and rotating shifts contribute significantly to emotional exhaustion and work–life imbalance. These findings can be interpreted with JD–R model, where caregiving responsibilities and rotating shifts act as job demands that increase strain and emotional exhaustion. In contrast, limited resources such as childcare support and stable scheduling reduce coping capacity, thereby intensifying work-life imbalance and burnout.
The study also revealed that ICU nurses experience substantial emotional spillover from work into their personal lives. Previous studies have similarly reported that ICU and NICU nurses often feel emotionally drained, with limited energy for family and personal activities after work (Hagen et al., 2025; Wudarczyk et al., 2025). Compassion fatigue has been shown to affect both personal and professional domains, leaving nurses functioning in a state of exhaustion rather than fulfillment (Hagen et al., 2025). In line with this evidence, participants in the current study described emotional exhaustion, reduced motivation, and difficulty in engaging in family life, all of which contribute to poor work–life balance. Additionally, work–life conflict has been associated with lower job satisfaction, increased stress, and higher turnover intentions (Rhéaume, 2022; Labrague et al., 2020). These findings align with the JD–R model, where high emotional demands in ICU settings deplete nurses’ energy, leading to exhaustion and impaired work-life balance. The lack of sufficient resources, such as psychological support and recovery time, further intensifies strain, contributing to reduced job satisfaction and increased turnover intentions.
Organizational constraints, such as understaffing, rigid scheduling, overtime, limited autonomy, insufficient recovery time, and low income, were identified as major barriers to nurses’ work–life balance. Notably, 69.2% of participants reported insufficient time for household responsibilities. These findings are consistent with existing literature, which highlights staffing shortages, irregular shifts, and heavy workloads as key contributors to burnout and poor work–life balance (Akter et al., 2019; Hujová et al., 2025; Mathebula et al., 2025; Widayana, Agustina, & Mediawati, 2025Widayana et al., 2025). Additionally, income and work schedules have been shown to significantly influence work–life balance in a Turkish study by Aslan et al. (2023), while financial stress among nurses is linked to reduced well-being and poorer mental health (Smith et al., 2026). The need for adequate rest and recovery has also been emphasized, as compressed schedules and insufficient time between shifts can exacerbate fatigue and negatively affect life outside work (Barker et al., 2025). These findings align with the JD–R model, where organizational constraints such as understaffing, heavy workload, and rigid scheduling function as high job demands that drive fatigue and work-life imbalance. Simultaneously, inadequate resources-such as fair income, autonomy, and sufficient recovery time –limit coping capacity, thereby intensifying burnout and negatively affecting well-being.
Nurses in the current study reported using various coping strategies, primarily self-care practices (such as exercise and yoga) and social support from friends, family, and colleagues. A substantial proportion (79.8%) reported receiving family support in managing work and personal responsibilities. These findings align with prior research identifying social support as a key coping mechanism (Badu et al., 2020; Cooper et al., 2020). Likewise, integrative reviews conducted among Australian nurses have identified strategies such as exercise, meditation, mindfulness, relaxation, and maintaining work–life balance as effective approaches to reducing stress and enhancing resilience (Badu et al., 2020; Li et al., 2024; Wei et al., 2025). Organizational interventions, such as flexible scheduling, adequate staffing, and family-supportive policies, have also been identified as critical for enhancing work–life balance (Widayana, Agustina, & Mediawati, 2025Widayana et al., 2025), consistent with the present study’s finding that 78.8% of nurses perceived flexible work arrangements and workplace childcare as beneficial in enhancing work–life balance. These findings are supported by JD–R model, where personal resources and job resources help buffer the impact of job demands. Such resources enhance resilience, reduce stress, and promote better work-life balance among nurses.
Financial factors also played a significant role in shaping work–life balance. Lower income was associated with higher mental workload and stress, indicating that financial difficulties influence how nurses prioritize work and family roles under pressure (Jin et al., 2024). This finding is consistent with the present study, which found that income significantly influenced the prioritization of work versus family responsibilities. Furthermore, previous research suggests that work–life balance among professionals is not uniform but is shaped by key demographic factors such as age, experience, and marital status (Ali et al., 2025). This aligns with the current study population, in which the majority of participants were novice nurses aged 21–30 years, unmarried, and with less than one year of ICU experience. These findings suggest that nurses at different life and career stages face distinct challenges. For example, early-career nurses may struggle primarily with job demands, whereas married or more experienced nurses may experience increased family responsibilities, affecting their work–life balance differently (Ali et al., 2025). Additionally, resilience has been shown to vary by gender, highlighting the need for targeted strategies to manage stress and support nurses’ well-being and quality of patient care (Aqtam et al., 2023). These findings can be interpreted through JD-R model, where financial strain and life-stage responsibilities act as contextual job demands that elevate stress and influence work-family prioritization. At the same time, individual factors such as experience and resilience function as personal resources, shaping how effectively nurses cope with demands and maintain work-life balance across different career stages.
A study of 500 Jordanian nurses found that higher education levels were associated with better work–life balance, although work demands continued to negatively affect family life (Abuhammad et al., 2025). Evidence from diverse global contexts, including Indonesia, Japan, Uganda, Bangladesh, Turkey, Malaysia, Jordan, South Korea, and Australia, shows that cultural and healthcare system differences significantly influence nurses’ work–life balance (Widayana, Agustina, & Mediawati, 2025Widayana et al., 2025). For example, a Japanese cohort study found that nurses may prioritize career advancement over family responsibilities to secure future stability (Tan et al., 2025). In contrast, the present study found that 42.3% of nurses prioritized family responsibilities over work during conflicts. These findings suggest that prioritization choices, whether career-focused or family-focused, are influenced by financial pressure and cultural expectations, which vary across different settings. These cross-cultural differences can be explained using JD-R model, where varying cultural expectations, financial pressures, and work demands act as context-specific job demands shaping prioritization between work and family roles. At the same time, resources such as education, career opportunities, and social support differ across settings, influencing how nurses balance demands and maintain work-life equilibrium.
Research conducted in Tamil Nadu, India, further supports these findings, indicating that nurses (particularly women) experience considerable challenges due to demanding work conditions, shift duties, and family responsibilities. Studies in this region have shown that age, income, and the nature of work significantly influence nurses’ ability to maintain work–life balance, with irregular shifts and heavy workloads contributing to imbalance (Jayarani & Mahalakshmi, 2020). Broader hospital-based studies in Tamil Nadu also emphasize that poor working conditions, long working hours, and inadequate staffing negatively affect work–life balance and well-being, particularly among married women (Sushil Shankar et al., 2020).
In Phase II, the sample predominantly comprised young, single, and novice nurses, which may limit the generalizability of the findings to ICU nurses with established family responsibilities. Consequently, the findings primarily reflect the experiences of nurses in the early stages of their careers rather than the broader ICU nursing workforce. Some interpretations of work–family conflict may therefore reflect adjustment-related stress associated with early professional roles rather than long-term work–life imbalance.
Strengths and Limitations
The sequential exploratory mixed methods design is a major strength of this study, as it facilitated a comprehensive understanding through the integration of qualitative and quantitative results. The development of the quantitative tool based on qualitative data increased the contextual relevance. The trustworthiness of the qualitative findings was strengthened through rigorous methods, such as data saturation, thematic analysis, and member checking. Additionally, the study considered both individual and organizational factors within the framework of the Job Demands–Resources model, providing a strong theoretical foundation. The use of joint displays further improved interpretive depth, and the study contributes valuable context-specific evidence from a tertiary care setting in India, where mixed-methods research remains limited.
Despite these strengths, several limitations warrant consideration. First, voluntary participation and informed consent may have introduced selection bias, as nurses with a particular interest in or experience of work–life balance issues may have been more likely to participate. Second, the study was conducted in a single tertiary care center, limiting the generalizability of the findings to other healthcare settings, such as primary care facilities, private hospitals, or different cultural and organizational contexts. The use of non-probability convenience sampling further restricts generalizability; therefore, the results should be interpreted with caution when applied to other settings or populations
In Phase II, 91.3% of participants had less than one year of ICU experience. This disproportionate representation limits the inclusion of more experienced ICU nurses. Therefore, the findings are likely to primarily reflect the perspectives and challenges of novice nurses in their early transition period rather than those of the wider ICU nursing workforce. The cross-sectional design of the study also precludes causal inferences, as the observed associations between demographic factors, work–life balance, and related outcomes do not establish directionality or temporality.
In addition, the study may be subject to social desirability bias, as participants might have provided responses they perceived as favorable or acceptable, particularly when discussing sensitive topics such as work–family conflict, organizational support, and coping strategies. The dichotomous questionnaire, developed from themes identified in the Qualitative Phase, has not undergone formal psychometric validation. Although items were reviewed for clarity and content relevance by subject-matter experts, the dichotomous format may have limited sensitivity in capturing nuanced experiences of work–life balance. Furthermore, reliance on self-reported data introduces the potential for recall and response biases. The use of a sample size calculation based on probability sampling assumptions, in conjunction with convenience sampling, may also limit the statistical representativeness of the findings.
Implications for Practice
The results highlight the importance of strengthening organizational support to help ICU nurses achieve work–life balance. Offering childcare facilities alone may be insufficient; these services should be made accessible, flexible, and responsive to nurses’ needs.
Hospitals should ensure adequate staffing levels and offer flexible work schedules to lighten the workloads of nurses and support the effective management of professional and family responsibilities. Nurse managers play a critical role in fostering a positive work environment by encouraging teamwork, promoting open communication, and providing emotional support to reduce stress and burnout.
Additionally, integrating wellness programs, stress management interventions, and self-care initiatives can enhance nurses’ coping capacity and resilience. Overall, optimizing organizational resources and support systems is essential for improving nurses’ well-being and maintaining high-quality patient care.
Future research should include multi-center studies with larger and more diverse samples, as well as longitudinal designs to examine the long-term effects of organizational interventions on nurses’ work–life balance, retention, and patient care outcomes.
Conclusion
This sequential exploratory mixed methods study provides a comprehensive understanding of the barriers, coping strategies, and work engagement outcomes related to work–life balance among ICU nurses in a tertiary care setting. Key barriers identified include staff shortages, rigid scheduling, overtime work, limited autonomy, low income, and insufficient recovery time. These factors contribute to emotional spillover, reduced motivation, stress, and exhaustion.
At the same time, nurses adopt coping strategies such as engaging in physical activities (e.g., exercise and yoga) and relying on social support from family, peers, and colleagues to manage work-related stress. The integrated findings indicate that flexible work arrangements and strong family support are essential for maintaining work–life balance, while financial strain further increases mental workload and stress.
Overall, these findings underscore the need for policies that prioritize adequate staffing, flexible scheduling, and fair compensation to promote nurses’ well-being, sustain work engagement, and ensure high-quality patient care in ICU settings. Furthermore, strengthening nursing education and research through collaborative efforts among policymakers, educators, and nursing leaders is essential to enhance workforce capacity and professional development (Nashwan et al., 2024).
Footnotes
Acknowledgement
The authors acknowledge the study participants.
Ethical Consideration
Ethical clearance was given by the Institutional Ethics Committee- (Approval Number: 8954/IEC/2024).Written informed consent was obtained from all participants prior to data collection. Ethical approval for the study was obtained from the Institutional Review Board (IRB) of SRM to Medical College Hospital and Research Centre (ECR/8869/INST/TN/2013/RR-19, dated 23/07/2024).
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study are not publicly available due to confidentiality restrictions and cannot be shared.
Roles and responsibilities
The funders had no role in the study design; data collection, management, analysis, or interpretation; or in the writing or publication of the report.