
Abstract
Introduction
Pneumonia is an inflammation of the air sacs in the lungs in response to an injury, such as infection. When the lungs are also involved, it could be referred to as bronchopneumonia. It can be one area of the lung or several areas. According to international data, pneumonia has been the main cause of lower respiratory tract infection (RTI)-related morbidity and mortality. With an anticipated 505,000 deaths worldwide in 2021 (range from 454,000 to 555,000), S. pneumonia was the cause of the greatest percentage of all age-lower RTI-related deaths.
Objective
To identify risk factors of pneumonia among under-five children who visit under-five OPD in Hadiya Zone public hospitals Central Ethiopia 2024.
Method
An institution-based unmatched case-control research design was used in Hadiya zone public hospitals, with 160 cases and 321 controls of children aged 2-59 months included in the sample. The cases were children with pneumonia, while the controls did not have pneumonia. Ethical clearance was obtained. Data was entered using Epi-Data version 4.6 and analyses using SPSS 27 statistical software. Bivariable and multivariable logistic regression analyses were performed to identify determinant factors. Statistical significance was declared at a p-value ≤ 0.05 with adjusted odds ratios (AORs) and 95% confidence intervals (CIs).
Result
Place of cooking (AOR: 2.75, 95%CI: 1.66, 4.58), History of Diarrhea in the past 2 weeks (AOR: 6.37, 95%CI: 3.63, 11.2), History of parental asthma in the family (AOR: 4.32, 95%CI: 2.31, 8.05), and a children received PCV vaccine during their infancy period (AOR: 2.09 95%CI: 1.24, 3.51), were found to be risk factors of under-five pneumonia.
Conclusion
In this study, the risk of pneumonia among under-five children was significantly associated with several factors, including whether the children came from households where people cooked indoors, whether the children had experienced diarrhea in the past two weeks, whether the children came from families where parents experienced asthma, and whether the children received the PCV vaccine in infancy. These factors are of critical importance in the management of pneumonia among under-five children and therefore warrant interventions aimed at reducing the risk of pneumonia in this group of people.
Introduction
Pneumonia is an inflammation of the air sacs in the lungs in response to an injury, such as infection. When the airways are also involved, it may be called bronchopneumonia (Ambroggio et al., 2023). According to international data, pneumonia has been the main cause of lower respiratory tract infection (RTI)-related morbidity and mortality. With an anticipated 505,000 deaths worldwide in 2021 (range from 454,000 to 555,000), S. pneumonia was the cause of the greatest percentage of all age-lower RTI-related deaths (1. GBD 2021 LRI Collaborators, 2024).
Yet over 5 million children are dying every year, and pneumonia accounts for nearly 20% of the deaths. The rate of progress in reducing pneumonia-related mortality has been slower than for other leading causes of child deaths (United Nations Inter-agency Group for Child Mortality Estimation, 2024c).
The World Health Organization data indicates that pneumonia resulted in the deaths of 147,180 children under-five years old, accounting for 22% of all fatalities among children aged 1 to 5 years. The incidence rate of under-five pneumonia is 0.29 episodes per child-year. The developing country accounts for 151.8 million cases per year; of these, 74% are accounted for by fifteen world countries, including Ethiopia (UNICEF, 2021). On the other hand, Southeast Asia and Africa are the two continents with the highest rates of under-five pneumonia, reporting an estimated 61 million and 35 million childhood pneumonia cases annually, respectively and also out of all the continents, Africa has the most significant incidence and severe cases of pneumonia (Abebaw et al., 2022).
Different reports show that from sub-Saharan Africa, Ethiopia has the highest rate of pneumonia, with an estimated 3.37milloin children affected by pneumonia annually, Ethiopia consistently ranks among the top nations in the world for under-five pneumonia mortality, usually ranking fifth or sixth among the top 15 countries with the highest burdens, according to current statistics and studies going up to 2023–2024. (18%-20% deaths (Girma et al., 2023).
Based on UNICEF reports, pneumonia accounts for 16% of all under-five deaths in sub-Saharan Africa compared to 14% for malaria and 10% for acute diarrheal diseases (UNICEF, 2023). In Ethiopia, as well as Hadiya Zone, pneumonia is a significant public health issue. However, there is a lack of local knowledge on specific risk factors for the development of pneumonia. The purpose of this study is to generate knowledge on specific risk factors for pneumonia among children aged less than five years in Hadiya Zone public hospital.
Review of Literature
Pneumonia is the leading cause of mortality and morbidity in children; according to the World Health Organization, pneumonia accounts for around 14% of deaths in children under five years old. Half of these deaths occur in sub-Saharan Africa (World health organization [WHO] 2023).
Ethiopia is among the countries with a high burden of under-five mortality, where pneumonia is a significant contributor. According to the Ethiopian demographic health survey report, acute respiratory infections, especially pneumonia, are the most common childhood illnesses (Ethiopian Statistical Service. (2026)).
Sociodemographic Related Factors
Several studies have identified multiple determinants of pneumonia among under-five children. A case-control study conducted in the Bangladesh stated that maternal age and the academic status of the mother and preterm babies were significantly associated with pneumonia (Islam et al., 2024). Another case-control study done in northeast Ethiopia confirmed that children having older mothers and having mothers who are housewives by occupation significantly play a role in the development of pneumonia (Bazie et al., 2021).
Maternal and Child-Related Factors
Maternal and child-related factors also play a crucial role in developing pneumonia. An Indonesian case-control study found that non-exclusive breastfeeding, lack of vaccination, and malnutrition increased the risk of under-five pneumonia (Sutriana et al., 2021). A study conducted in the tertiary hospital of Mogadishu, Somalia, shows that unvaccinated children, allergic disease in the family, and children’s history of pneumonia for the past two weeks were factors that affected under-five pneumonia (Roble et al., 2025).
On the other hand a hospital-based study in South Africa reported that HIV-exposed and malnourished children had a higher risk of under-five pneumonia (Le Roux et al., 2021). A study in Eastern Ethiopia found that malnutrition, lack of vaccination, altered mental status, complicated pneumonia, and cigarette smoke exposure increased the risk of pneumonia in children (Adbela et al., 2024). Similarly, a case-control study in Jijiga found that incomplete vaccination, cooking smoke exposure, household respiratory infections, diarrhea, and female sex increased the risk of under-five pneumonia (Osman et al., 2025).
Household and Environmental
Environmental factors are among the most important determinants of childhood pneumonia.
A study conducted in Bangladesh by found that poor household environmental conditions, including overcrowding, indoor smoke exposure, and the use of unclean cooking fuels, were significantly associated with respiratory infections among under-five children (Islam et al., 2024). A study conducted in Gamo Zone, southern Ethiopia, reported that children from households where food was cooked inside the living room had a significantly higher risk of pneumonia (Solomon et al., 2022).
Methods and Materials
Study Area and Period
The study was conducted in Hadiya zone, which is the capital city of the Central Ethiopia region; also, it is one of the 7 zones in Central Ethiopia. It has 13 woredas and 4 town administrations with a total of 329 kebeles, of which 303 are rural and 26 are urban. It is located 230 Km away from the capital city of Ethiopia. It is situated at an altitude of 1800-2950 meters above sea level and has an average temperature ranging from 10 to 24 degrees centigrade. The zone has 1 specialized hospital and 3 first-level hospitals. This study was conducted in public hospitals of the Hadiya zone from February 1 to March 30, 2024.
Study Design
Institutional based un-matched case-control study design was conducted to asses’ Risk Factors of pneumonia.
Source Population
All under-Five Children who visit the Hadiya Zone Public Hospital’s Pediatrics OPD.
Study Population
All selected under-five children who visited the selected Hadiza zone Public Hospital’s pediatrics OPD during the study period.
Sample Population
All under-five children who fulfill the inclusion criteria at the selected public hospitals were included in the study.
Case Definition
All under-five children with a diagnosis of pneumonia who come for treatment service during the data collection period.
Definition of Pneumonia Diagnosis
Clinical and radiographic criteria were used in this investigation to diagnose pneumonia. Clinically, the diagnosis was made in accordance with the criteria of the Integrated Management of Neonatal and Childhood Illness (IMNCI), which was defined as the presence of cough and/or breathing difficulties along with age-specific fast breathing and/or chest indrawing. Chest X-ray results consistent with pneumonia, such as the presence of lung infiltrates, consolidation, or other suggestive abnormalities, as reported in patient records, served as the basis for radiological confirmation.
Control Definition
All under-five children who visited a ‘sick-baby clinic’ and were registered and classified for a condition other than pneumonia within a similar study period.
Control Selection
Controls were under-five children attending the same OPD during the same period as cases but without pneumonia based on IMNCI assessment. Cases and controls were selected from the same health facilities and catchment population, improving comparability, reducing selection bias, and enhancing internal validity.
Inclusion Criteria
All under-five children who visited the selected public hospital during the study period were eligible for inclusion.
Exclusion Criteria
• Caregivers who did not have information about the child at the time of data collection were excluded. • Children with cough due to a recent history of liquid or foreign body aspiration were excluded. • Infants aged less than two months were excluded. • Severe pneumonia cases were excluded.
To establish a fairly homogeneous study sample and to concentrate on pneumonia Risk Factors among outpatient and early emergency presentations, children with severe pneumonia necessitating hospitalization were excluded. In addition to producing findings relevant to basic healthcare and community-level initiatives, this strategy reduces confounding from illness severity and concomitant diseases, which are more prevalent among hospitalized patients.
Sample Size Determination and Sampling Procedure
Sample Size Determination for Risk Factors of Pneumonia Among Children Under-five Years in a Hospital-Based Case-Control Study in Public Hospitals in Hadiya Zone, Central Ethiopia, 2024
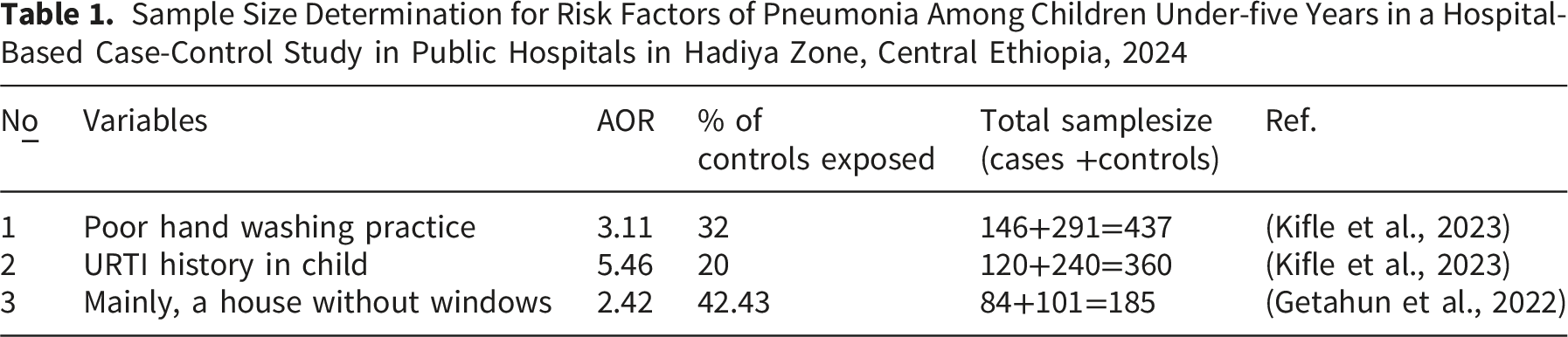
Finally, the maximum sample size is 437 (146 cases and 291 controls) after adding a 10% non-respondent rate. 44+437=
Sampling Procedure
Among the four public hospitals found in the Hadiya zone, two were selected using simply random sampling. The estimated number of outpatient visits to the under-five children outpatient department of each hospital for two months was counted from registrations and used as a baseline. Then the sample size for each hospital was proportionally allocated. The total sample size was then proportionally allocated to each selected hospital. Systematic random sampling was used to select both cases and controls. The estimated two-month study populations were 240 cases and 710 controls from Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital (NEMMCSH), and 86 cases and 264 controls from Shone Hospital.
The sampling interval (k) was calculated for each hospital separately. For NEMMCSH, k was approximately 3 for controls (710/234 ≈ 3) and 2 for cases (240/117 ≈ 2), meaning every 3rd control and every 2nd case was selected. Similarly, for Shone Hospital, k was approximately 3 for controls (264/87 ≈ 3) and 2 for cases (86/43 ≈ 2), meaning every 3rd control and every 2nd case was selected (Figure 1). Schematic presentation of the sampling procedures used to select study participants in public hospitals in Hadiya zone, Central Ethiopia, 2024
The sampling frame included all children less than five years of age who attended the outpatient department of the health facilities involved in the study during that period. All eligible participants were identified from outpatient registration records, which were considered comprehensive.
Data Collection Instrument and Procedures
Parents of children aged two months to five years who were present during data collection were eligible to participate in the study. Face-to-face interviews and document reviews were conducted to collect data on socio-demographic and other independent variables. Before data collection, the questionnaire was pretested to ensure clarity, consistency, and contextual relevance. Findings from the pretest were used to make necessary modifications to improve comprehension and relevance.
The final questionnaire demonstrated acceptable internal consistency (Cronbach’s alpha = 0.82). It was adapted from previously validated tools and relevant literature (Bazie et al., 2021; Getahun et al., 2022; Kifle et al., 2023,). Participants were classified as cases and controls by physicians based on clinical examination and chest X-ray findings. Data collection was conducted individually in a convenient setting for respondents, and all information was recorded using a structured data collection sheet developed for the study.
Data Quality Control
The questionnaire was evaluated by experts in related fields. Intensive training that lasts two days was offered by the principal investigator to the data collectors and supervisors on the technique of timely data collection, the purpose of data collection, and the contents of the questionnaires. The data collection instrument was pretested on 5% of the total sample size. The principal investigator and field supervisor closely monitored trained data collectors to ensure that the study protocol was followed and the responses were completed. The completed questionnaires were checked daily for consistency and completeness. In data entry, double verification was used, and any differences were resolved by cross-checking the data. All data were further reviewed by the supervisor and principal investigator for completeness and consistency.
Data Processing and Analysis
Data was entered using Epi-Data version 4.6 and analyzed using SPSS 27 statistical software. Model adequacy was assessed using the Hosmer–Lemeshow goodness-of-fit test. A bivariate logistic regression analysis was performed for each independent variable. Accordingly, those variables having a p-value less than or equal to 0.05 in the bivariate analysis were fitted to the multivariable logistic regression model. In multivariable regression, a P-value less than or equal to 0.05 was considered statistically significant. Multi-collinearity among independent variables was checked by the variance inflation factor (VIF).
Results
Sociodemographic Characteristics of the Respondents
Sociodemographic Characteristics of the Participants in Public Hospitals in Hadiya Zone, Central Ethiopia, 2024

Household and Environmental Characteristics of the Participants
Household and Environmental Characteristics of the Respondents in Public Hospitals in Hadiya Zone, Central Ethiopia, 2024

Parental and Child-Related Characteristics
Parental and Children-Related Characteristics of Respondents in Public Hospitals in Hadiya Zone, Central Ethiopia

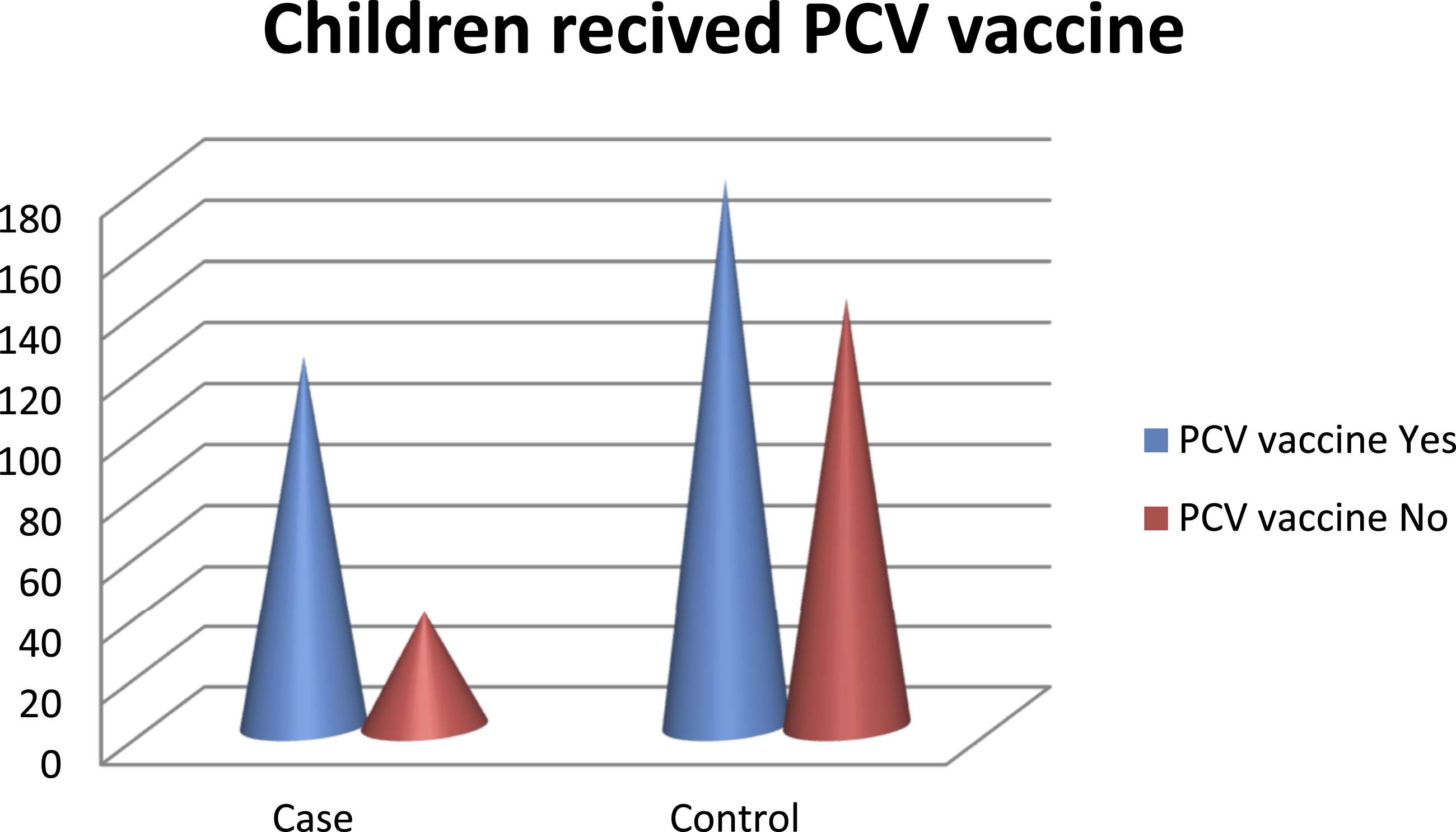
Distribution of PCV vaccination status among children under five years in public hospitals in Hadiya Zone, Central Ethiopia
Diagnostic Frequency Distribution of Control Group
Several conditions other than pneumonia were found in the controls. The most frequent diagnoses were feverish illnesses, severe diarrheal disorders, upper respiratory tract infections, and other minor ailments. IMNCI clinical evaluation and, when available, chest X-ray results were used to determine the control group (Supplementary table-1).
Risk Factors of Under-five Pneumonia
Binary logistic regression analysis was utilized to uncover independent factors of pneumonia in children under the age of five. First, the respondents’ socio-demographic variables, housing, and environmental variables, as well as parent- and child-related characteristics, were compared to the outcome variable, which was a risk factor, using a bivariate analysis. Variables with a p-value ≤ 0.05 were entered into the final multivariable logistic regression model.
Bivariable and Multivariable Logistic Regression Analysis of Factors Associated With Pneumonia Among Children Under-five-Years in Public Hospitals of the Hadiya Zone, Central Ethiopia, 2024 (N = 481)

Note. COR = crude odds ratio; AOR = adjusted odds ratio; CI = confidence interval; PCV = pneumococcal conjugate vaccine; URTI = upper respiratory tract infection.
Odds ratios are from binary logistic regression. The reference category for each variable is indicated as
Discussion
Pneumonia in children under the age of five is a prominent cause of illness and death globally, with particularly high rates in impoverished countries such as Ethiopia. Understanding the determining variables is critical for developing an effective care and preventive approach for pediatric pneumonia. These studies identify easy-to-prevent determining variables. The findings of this study showed that place of cooking, history of diarrhea in the preceding two weeks, parental history of asthma, and pneumococcal conjugate vaccine (PCV) status during infancy were significantly associated with pneumonia among under-five children.
Findings should be interpreted as associations rather than causal relationships due to the observational nature of the study. In addition, the results should be interpreted with caution because of potential selection and information biases inherent in the hospital-based case–control design.
The place of cooking was the key variable that indicated association with under-five pneumonia. Children from households where cooking was conducted inside the living house had significantly higher odds of developing pneumonia compared to those with a separate kitchen (AOR = 2.75, 95% CI: 1.66–4.58).
Similar studies in Indonesia; Gamo Zone southern,Ethiopia; and a study conducted in Worabe, Ethiopia, respectively, support this result (Abate et al., 2021; Seramo et al., 2022; Solomon et al., 2022; Sutriana et al., 2021).
This could be due to indoor pollution from unsafe energy sources such as charcoal, wood, and biomass. Indoor air pollution, notably from the use of solid fuels for cooking and heating, is a major risk factor for childhood pneumonia, particularly in nations with low and moderate income levels like Ethiopia. Exposure to these pollutants weakens a child’s respiratory system, leaving them more susceptible to diseases like pneumonia. Reducing indoor air pollution through initiatives like encouraging clean fuel usage and better cooking stoves is critical for pneumonia prevention.
Children with a history of diarrhea in the last two weeks had markedly higher odds of pneumonia compared to those without such history (AOR = 6.37, 95% CI: 3.63–11.2). This study was consistent with other previous studies in Spain, Uganda, Gambela, Ethiopia and Gonder, Ethiopia, respectively (Bazie et al., 2021; Prat, C et al., 2021; Getahun et al., 2022; Wanyana et al., 2024).
The possible reason may be due to the fact that the history of diarrhea is strongly associated with the development of pneumonia in children under five, and diarrhea is one of the main causes of mortality in this age range. This elevated risk is probably brought on by a compromised immune system as well as other elements associated with inadequate sanitation and hygiene. Consequently, in order to lessen the burden of these infectious diseases, important preventative strategies include the rotavirus vaccine, hand washing with soap, access to safe drinking water, better sanitation, and exclusive breastfeeding for the first six months.
Similarly, children with a family history of parental asthma had increased odds of pneumonia compared to those without such history (AOR = 4.32, 95% CI: 2.31–8.05). This finding agreed with studies conducted in different parts of the world: Malaysia, the Netherlands, and Worabe, Ethiopia, respectively (Ramzi, N., et al., 2024; Seramo et al., 2022).
The possible explanation might be that an important risk factor for pediatric pneumonia is a history of parental asthma; evidence suggests that children who have asthmatic parents are at a higher risk of contracting pneumonia themselves. Common genetic predispositions and environmental variables that promote vulnerability to both illnesses are probably the cause of this connection. Genetic factors can impact both pneumonia and asthma. A child who has an asthmatic parent may inherit genes that increase their vulnerability to respiratory conditions like pneumonia. Children who suffer from asthma or pneumonia are more susceptible to respiratory infections since these conditions can impact immune system development and function.
The PCV vaccine was also another factor identified to affect the occurrence of pneumonia in children under five years old. Children who did not receive the pneumococcal conjugate vaccine (PCV) had higher odds of developing pneumonia compared to vaccinated children (AOR = 2.09, 95% CI: 1.24–3.51). Those similar studies done in different countries, like the Public Health Foundation of India, state systematic reviews in East Africa and at Jimma University Medical Center in Ethiopia, respectively (Abate et al., 2021; Singh et al., 2022; Tegenu et al., 2022) support the finding.
This association might be immunization mitigates childhood pneumonia through two mechanisms. Firstly, vaccinations avert infections that directly induce pneumonia, such as Haemophilus influenza type B, and infections like measles and pertussis that can indicate pneumonia as a complication can also be avoided by vaccination. On the other hand, PCV functions via boosting the immunological system to generate antibodies against the Streptococcus pneumonia bacterium, a prevalent cause of pneumonia.
PCV has demonstrated considerable efficacy in decreasing the occurrence of pneumococcal pneumonia in children, with research indicating substantial decreases. The vaccination further safeguards against other serious pneumococcal infections such as meningitis and sepsis, which can be life-threatening in hospitalized patients and in situations of radiologically, confirmed pneumonia. PCV has significantly reduced pneumonia-related fatalities in children by preventing pneumococcal pneumonia.
Lastly, the results of this study have significant ramifications for public health management, especially in environments with limited resources where pneumonia remains a major cause of illness and mortality in children under five years. By identifying significant factors, this study presents practical evidence for focused intervention. Increasing community-based child health programs includes increasing immunization coverage, lowering exposure to indoor air pollution, preventing exposure to diarrheal disease, and early identification of family history of asthma. Cold reduced the burden of under-five pneumonia.
Strengths and Limitations of the Study
Data were collected from multiple public hospitals in Hadiya Zone, improving the variability of participants and enhancing internal validity. A relatively large sample size with an adequate case-to-control ratio was used, increasing the statistical power of the study. Pneumonia cases were ascertained using standard clinical criteria.
This study has several limitations. First, selection bias in the control group cannot be fully ruled out, which may affect the comparability between cases and controls. In addition, recall bias may have influenced some exposure variables, including indoor cooking practices and parental history of asthma. Although data were collected prospectively, the case–control design inherently limits the ability to establish causal relationships.
Implications for Practice
The results of this study suggest targeted interventions to control and prevent pneumonia in young children in such settings. Strengthening routine immunizations, improving indoor air quality, and promoting early health-seeking behaviors among caregivers are important. It is important for healthcare workers to emphasize early screening of high-risk young children and community-based health education for caregivers to avoid preventable risk factors.
Conclusion and Recommendations
In this study, the risk of pneumonia among under-five children was significantly associated with several factors, including whether the children came from households where people cooked indoors, whether the children had experienced diarrhea in the past two weeks, whether the children came from families where parents experienced asthma, and whether the children received the PCV vaccine in infancy.
These factors are of critical importance in the management of pneumonia among under-five children and therefore warrant interventions aimed at reducing the risk of pneumonia in this group of people. So to decrease the risk of pneumonia, caregivers need to enhance ventilation, address diarrhea, and vaccinate at the appropriate time against PCV, while health workers need to educate families and identify at-risk children, and policymakers need to advocate for clean cooking, strengthen immunization, and raise awareness about the risk of pneumonia in families.
Supplemental Material
Supplemental Material - Risk Factors of Pneumonia Among Under-five Children Attending the Public Hospital of Hadiya Central Ethiopia 2024
Supplemental Material for Risk Factors of Pneumonia Among Under-five Children Attending the Public Hospital of Hadiya Central Ethiopia 2024 by Seifu Awgchew Mamo, Sisay Foga, Rediet Gebreselassie Kelelew, Eliase Ezo, and Asnakech Zekiwos Heliso in Sage Open Nursing.
Footnotes
Acknowledgment
We would like to thank the study participants for the scarification of their valuable time spent filling out questionnaires, selected Hadiya Zone Public Hospitals, and Wachemo university.
Ethical Considerations
Ethical clearance was obtained from Wachemo University College of medicine and health science, institutional review board (WCU/IRB/0039/24) and a formal letter of cooperation to conduct this research was written to select Hadiya Zone Public Hospitals.
Consent to Participate
Each participant provided written informed consent, and the data collected from them would not have been shared. To maintain secrecy, privacy, and anonymity, names and other personally identifiable information about respondents were removed using coding. The participants were made fully aware that they might revoke their permission at any moment without incurring any fees or losing any advantages.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.