
Abstract
Introduction
Palliative care nurse practitioners work in sustained proximity to death, grief, and end-of-life decision, yet relatively little is known about how this role relates to psychological well-being and depressive symptoms.
Objective(s)
To examine subjective happiness, mental well-being, and depressive symptoms among palliative care nurse practitioners in Israel, and to explore how clinicians interpret repeated exposure to death in relation to these experiences.
Methods
An explanatory sequential mixed-methods study was conducted among certified palliative care nurse practitioners in Israel. In the quantitative phase, participants completed the Subjective Happiness Scale, the Mental Health Continuum-Short Form, and the Center for Epidemiologic Studies Depression Scale. In the qualitative phase, a focus group was conducted with survey respondents to explore meaning, coping, and death-related experiences. Descriptive statistics, internal consistency estimates, and Pearson correlations were used for the quantitative analysis. Qualitative data were analyzed using reflexive thematic analysis.
Results
Thirty-six nurse practitioners completed the survey and ten participated in the focus group. Participants reported moderate subjective happiness and mental well-being, while 44.4% scored above the threshold for elevated depressive symptoms on the depression screening measure. Qualitative analysis generated four themes: temporal reflections on death, cultural and societal meaning, existential struggle, and professional-personal identity intersections.
Conclusion
Palliative care nurse practitioners may sustain professional meaning while also carrying substantial depressive symptom burden. Institutional responses should move beyond informal self-care and include structured reflective support, mental health monitoring, and workforce policies that acknowledge the emotional consequences of repeated exposure to dying.
Introduction
Caring for patients at the end of life is emotionally and existentially demanding. Clinicians who repeatedly accompany patients and families through dying trajectories are exposed not only to suffering and grief, but also to sustained relational, ethical, and existential strain. Within this context, palliative care nurse practitioners (NPs) play a central role in symptom management, care coordination, decision support, family guidance, and continuity of care across serious illness and dying, placing them in ongoing proximity to death and loss (Aaron & Andrews, 2016; Haron et al., 2019; Institute of Medicine, 2011; International Council of Nurses, 2020; Israel Ministry of Health, 2012; National Academies of Sciences, Engineering, and Medicine, 2021; Romem et al., 2023). Despite the growing clinical importance of this role, limited research has examined how repeated exposure to death is reflected in the psychological well-being of palliative care NPs.
Review of Literature
Existing literature has addressed distress, burnout, and professional quality of life among nurses and palliative care clinicians, yet less is known about how subjective happiness, mental well-being, and depressive symptoms are experienced specifically by palliative care nurse practitioners (Ablett & Jones, 2007; Kakemam et al., 2019; Li et al., 2021; Peters et al., 2012). This gap is important because psychological functioning in palliative care cannot be captured through a single indicator. Repeated exposure to suffering, grief, and close relationships with patients and families may affect multiple, partly overlapping dimensions of mental life, including positive appraisal, emotional and social functioning, and depressive symptom burden (Bożek et al., 2020; Gray et al., 2019; Marchand et al., 2015; Parent-Lamarche & Marchand, 2019; Ruggeri et al., 2020; World Health Organization, 2022). Subjective happiness reflects a global appraisal of one’s life and positive experience (Khosrojerdi et al., 2018; Lyubomirsky & Lepper, 1999; Yoon et al., 2022), whereas mental well-being encompasses broader emotional, psychological, and social functioning (Ruggeri et al., 2020; World Health Organization, 2022). Depressive symptoms, in turn, reflect distress-related affective burden that may coexist with preserved professional functioning rather than simply replace it (Braquehais et al., 2020; Klapwijk et al., 2020). Related constructs, including compassion satisfaction, compassion fatigue, and professional quality of life, similarly suggest that meaning, commitment, and strain may coexist rather than operate as mutually exclusive states (Geoffrion et al., 2019; Samson et al., 2016; Samson & Shvartzman, 2018; Stamm, 1995).
This conceptual distinction is especially relevant in palliative care NP practice, where high clinical responsibility intersects with sustained exposure to mortality. In small national workforces, these clinicians may experience both strong professional visibility and considerable emotional burden. Moreover, death in palliative care is not only a clinical outcome but also a relational and existential event. Attitudes toward death are shaped by personal experience, training, culture, and organizational context, and these factors may influence both coping and the quality of end-of-life care (Cybulska et al., 2022; Fernández-Gutiérrez et al., 2024; Gama et al., 2012; He et al., 2023; Johansson & Lindahl, 2011; Klapwijk et al., 2020; Lange et al., 2008; Peters et al., 2013; Wong et al., 1994; İnci & Koraş Sözen, 2024). Repeated proximity to dying may therefore deepen existential reflection and professional meaning while also leaving clinicians emotionally vulnerable.
Terror Management Theory offers a useful interpretive view for this tension. The theory proposes that awareness of mortality can evoke existential anxiety that is managed through symbolic, relational, and meaning-based resources, including cultural worldviews, self-esteem, and close relationships (Arndt et al., 2002; Greenberg & Arndt, 2012; Greenberg et al., 1986). In the present study, this framework is not treated as a directly tested explanatory model, but as a heuristic for understanding how palliative care nurse practitioners may sustain commitment, and professional functioning while remaining susceptible to emotional burden (Bergman et al., 2018; Hart et al., 2005; Pyszczynski et al., 2021). Accordingly, the present mixed-methods study was designed not only to quantify levels of subjective happiness, mental well-being, and depressive symptoms among palliative care nurse practitioners in Israel, but also to examine how these clinicians themselves interpret repeated exposure to death and dying in relation to their psychological well-being and emotional burden. By integrating standardized psychological measures with qualitative accounts of lived professional experience, the study seeks to generate a more comprehensive understanding of how well-being and distress coexist in this workforce, and what may remain obscured when either quantitative or qualitative evidence is considered alone.
Methods
Design
An explanatory sequential mixed-methods design was used to clarify an observed quantitative pattern: moderate subjective happiness and mental well-being alongside elevated depressive symptoms in a substantial proportion of participants. In the first phase, survey data were collected to describe subjective happiness, mental well-being, and depressive symptoms. In the second phase, qualitative data were collected through a focus group with survey respondents to explore how repeated exposure to death, grief, and professional meaning might help contextualize this pattern. Integration occurred through connected sampling, whereby focus group participants were recruited from survey respondents, and through interpretive merging, whereby qualitative themes were used to explain and contextualize the quantitative findings.
Research Question(s)
This study addressed two research questions: (1) What are the levels of subjective happiness, mental well-being, and depressive symptoms among palliative care nurse practitioners in Israel? (2) How do palliative care nurse practitioners interpret repeated exposure to death and dying in relation to their psychological well-being and emotional burden?
Sample
The survey was distributed to all accessible certified palliative care nurse practitioners practicing in Israel between October 2021 and February 2022 through professional WhatsApp groups and nursing forum.
Inclusion criteria: Eligible participants were certified registered nurses with a master’s degree, formal nurse practitioner certification in palliative care, current employment in a palliative nurse practitioner role, Hebrew fluency, and provision of informed consent. Exclusion criteria: were absence of palliative care nurse practitioner certification, not currently practicing in a palliative nurse practitioner role, inability to complete the study materials in Hebrew, or failure to provide informed consent.
Thirty-six of 73 eligible palliative care nurse practitioners completed the survey, yielding a response rate of 49.3%. For the qualitative phase, only survey respondents who volunteered for the focus group were included. Participants represented health maintenance organizations, general hospitals, and geriatric medical centers. Data collection took place during the later phases of the COVID-19 pandemic, a context that may have influenced workload, staffing conditions, grief exposure, and psychological distress (Braquehais et al., 2020; Gebhard et al., 2022).
The study targeted the full accessible population of certified palliative care nurse practitioners practicing in Israel during the study period. Because this is a small national workforce, recruitment followed a census-based approach rather than sampling to a predetermined powered effect size. Accordingly, the quantitative findings should be interpreted as exploratory and descriptive rather than confirmatory.
Institutional Review Board Approval and Informed Consent
Participants were recruited through purposive and snowball sampling among Israeli palliative care NPs. All participants provided informed consent. The study was approved by the Institutional Review Board of Jerusalem College of Technology Ethics Committee (approval no.: 21_014).
Data Collection
Quantitative Phase
Data collection consisted of an anonymous web-based survey distributed through professional WhatsApp groups and a palliative care nurse practitioner forum. The opening page described the study and included an informed consent form. Participation was voluntary, and the survey terminated automatically for respondents who declined consent, ensuring that no identifying information was recorded. Of the 73 questionnaires distributed, 36 were returned fully completed, yielding a response rate of 49.3%.
Qualitative Phase
From the nurses who completed the questionnaire, participants were invited to take part in a voluntary focus group; 10 nurses agreed to participate. The focus group was conducted online via Zoom in March 2022 and facilitated by a member of the research team using a semi-structured guide addressing meanings of death, coping strategies, and professional and personal boundaries. The session lasted approximately 90 minutes, was audio-recorded, transcribed verbatim, and de-identified. Data were analyzed using reflexive thematic analysis: two researchers independently coded the transcript, compared codes, and iteratively developed themes through discussion and consensus; discrepant interpretations were resolved through team review. Trustworthiness was supported through investigator triangulation and an audit trail documenting coding decisions and the rationale for selecting illustrative quotations. Given the emotional and identity-laden nature of end-of-life care, reflexivity was treated as a methodological requirement. Facilitators and coders documented their assumptions before analysis and revisited them throughout the analytic process to reduce premature interpretive closure and enhance confirmability.
Statistical and Qualitative Analysis
Descriptive statistics summarized participant characteristics and scale scores (means, standard deviations, ranges, frequencies, and percentages). Internal consistency reliability was examined using Cronbach’s alpha. Associations between continuous variables (SHS, MHC-SF total and subscales, and CES-D total and subscales) were evaluated using Pearson correlation coefficients (two-tailed), with statistical significance set at p < .05. Analyses were conducted using SPSS version 27. Qualitative data were analyzed using reflexive thematic analysis. An inductive coding process was used to identify patterns across the transcript, followed by iterative theme development through team discussion and refinement. Trustworthiness was supported through systematic documentation of analytic decisions, iterative memo-writing, and regular peer debriefing to challenge assumptions and refine theme boundaries.
Integration of Findings
Integration occurred at both the design and interpretation stages. At the design stage, survey respondents were invited to participate in the qualitative phase, creating a connected sample. At the interpretation stage, qualitative themes were used to contextualize the quantitative pattern of moderate subjective happiness and mental well-being alongside elevated depressive symptoms. Specifically, the qualitative data helped illuminate how existential reflection, repeated exposure to dying, and blurred professional-personal boundaries may coexist with preserved meaning and professional functioning.
Measures, Validity, Reliability, and Rigor
Three validated questionnaires and a sociodemographic questionnaire were used in the study: the Subjective Happiness Scale (SHS; Lyubomirsky & Lepper, 1999), the Mental Health Continuum-Short Form (MHC-SF; Lamers et al., 2011), and the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977). Hebrew translations were provided through the Professional Committee for Clinical Psychology in the Israeli Ministry of Health. All measures were scored according to published instructions, and score ranges and interpretation are reported to support transparency. Internal consistency for each instrument in the current sample was assessed using Cronbach’s alpha. The CES-D cut-off is presented as an indicator of elevated depressive symptoms on a screening measure rather than as a diagnostic threshold.
Subjective Happiness Scale (SHS)
SHS (Lyubomirsky & Lepper, 1999) consists of 4 items, where the respondent is asked to rate themselves on a 7-point Likert scale. For two of the items, the respondent is asked to describe the extent of their happiness (in absolute and relative terms), and in the other two, are asked to describe how similar they are to two short descriptions of people who are happy/unhappy. The average of the 4 items is calculated, with item 4 being a reversed item. The higher a person’s score, the higher the reported level of happiness and psychological well-being. Since the test assesses a person’s degree of happiness, there is no cut-off point that indicates a standard level of happiness. The scale exhibits high internal consistency, with Cronbach’s alpha values ranging from 0.79 to 0.94 across various populations and studies.
Mental Health Continuum-Short Form (MHC-SF)
The Mental Health Continuum-Short Form consists of 14 items rated on a 6-point Likert scale reflecting the frequency of emotional, social, and psychological well-being experiences during the previous month (Lamers et al., 2011). Items yield emotional, social, and psychological well-being subscale scores and an overall mean score. The questionnaire has high psychometric data, including a high internal consistency reliability in which Cronbach’s alpha coefficient of 0.89 for the entire questionnaire, and between 0.74-0.93 for each scale separately.
Center for Epidemiologic Studies Depression Scale (CES-D)
The Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) is a 20-item self-report screening questionnaire for depressive symptoms. Respondents indicate how often each item reflected their experience during the previous week on a 4-point Likert scale ranging from 0 (rarely or never) to 3 (most or all of the time). Items are commonly grouped into depressive affect, positive affect, somatic and retarded activity, and interpersonal difficulties (Shafer, 2006). The instrument has demonstrated good psychometric properties, including internal reliability of approximately 0.85 in general populations and 0.90 in clinical populations (Radloff, 1977). Higher total scores indicate greater depressive symptom burden. In this study, a score of 17 or higher was used as an indicator of elevated depressive symptoms on a screening measure rather than as a diagnostic threshold (Blumstein et al., 2012; Steinman et al., 2017).
Results
Sample Characteristics
Participant Demographics of Palliative Care Nurse Practitioners (N=36)
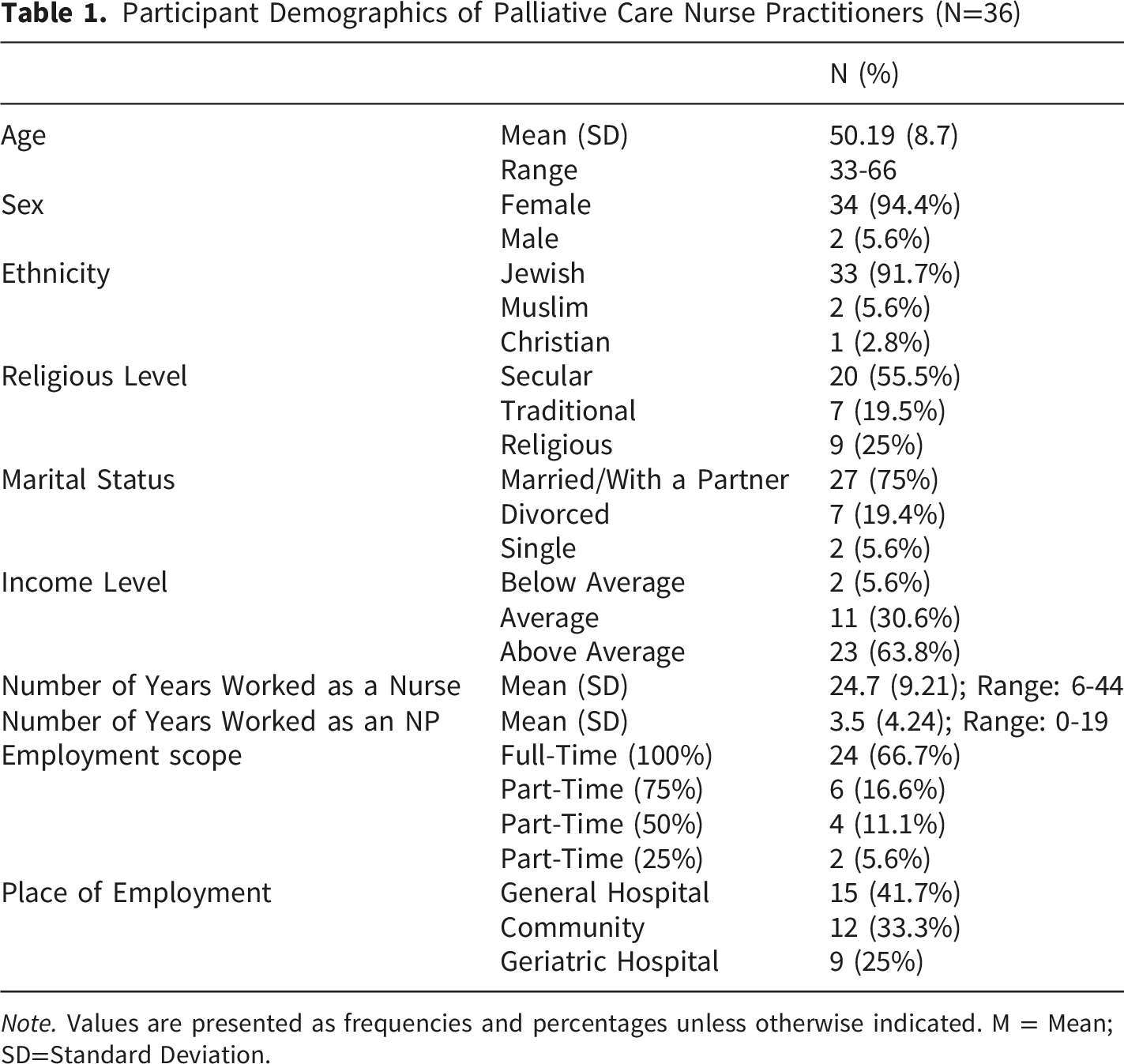
Note. Values are presented as frequencies and percentages unless otherwise indicated. M = Mean; SD=Standard Deviation.
Research Question Results
Scale Scores
Subjective Happiness Scale
The mean SHS score was 5.38 (SD = 0.96), indicating moderate subjective happiness in this cohort.
Mental Health Continuum-Short Form
The overall MHC-SF mean was 4.59 (SD = 0.60), with emotional well-being scoring highest (M = 4.82). Social well-being was somewhat lower (M = 4.20), suggesting relatively weaker perceptions of community connectedness compared with other well-being domains.
Center for Epidemiologic Studies Depression Scale
Scores on the SHS, MHC-SF, and CES-D Scales Among Palliative Care Nurse Practitioners (N=36)

Note. SHS = Subjective Happiness Scale; MHC-SF = Mental Health Continuum–Short Form; CES-D = Center for Epidemiologic Studies Depression Scale; M = Mean; SD=Standard Deviation.
Distribution of CES-D Levels Among Palliative Care Nurse Practitioners (N=36)

Note. CES-D = Center for Epidemiologic Studies Depression Scale. Higher scores indicate more severe depressive symptoms.
Association Matrix of Well-Being, Happiness, and Depression Among Palliative Care Nurse Practitioners (N=36)

Note. Values are Pearson correlation coefficients (r). N = 36. p < .05*, p < .01**, p < .001***. Dashes indicate correlations not reported in the present analysis.
Findings From the Thematic Synthesis
Thematic analysis generated four interrelated themes: temporal reflections on death, cultural and societal meaning frameworks, existential struggle and anticipatory self-reflection, and professional-personal identity intersections.
Temporal Reflections on Death
Participants described how time shapes the experience of dying, including the unsettling ways deaths seem to cluster around meaningful dates and the contrast between abrupt and peaceful endings. “Death near holidays…” “The inevitability and unpredictability of death… from peaceful cradling to an abrupt ’poof.”
Cultural and Societal Meaning
Death was frequently interpreted through collective memory and cultural framing. Some participants experienced discomfort when discussing personal death on nationally significant days, while others emphasized the role of tradition in shaping how death is understood and accepted. “I am feeling a little disturbed talking about my death on Holocaust Memorial Day.” “In the end, with all the desires and plans, usually everything is predetermined for everyone as in tradition.”
Existential Struggles
Alongside professional familiarity with dying, participants expressed personal vulnerability as fears, anticipatory reflection, and the emotional weight of imagining one’s own death. Some participants also expressed acceptance and curiosity about dying as part of this existential processing, rather than as a separate theme. These accounts suggested that clinical exposure does not eliminate existential anxiety; rather, it can intensify introspection. “Looking deeply into myself about the process of death and my desires.” “It’s melancholic to ponder what comes after my demise.” “Indeed, death is scary, and one needs to confront it and elevate the discourse.” “Death is present and exists; it’s part of the cycle of life.” “Death isn’t terrible; it can even be special and interesting.”
Professional-Personal Identity Intersections
Participants described blurred boundaries between professional role and private life, especially when emotional bonds with patients deepened and grief “followed them home.” “Thoughts about death and how I want it make me appreciate life…” “There is a wide variety of fears… death encompasses many aspects and reflects a person’s personality, his values, and his way of life.”
Discussion
This study examined subjective happiness, mental well-being, and depressive symptoms among palliative care nurse practitioners in Israel in the context of repeated exposure to death and dying. Overall, the findings suggest a psychologically complex profile. Participants reported moderate levels of subjective happiness and mental well-being, yet a substantial proportion also reported elevated depressive symptoms on a screening measure. This pattern warrants careful interpretation. It does not indicate a contradiction in a strict theoretical sense, nor does it establish a distinct psychological model. Rather, it may reflect the fact that the constructs measured in this study are related but not identical. In other words, palliative care nurse practitioners may preserve meaning, professional purpose, and aspects of positive psychological functioning while simultaneously carrying emotional burden associated with repeated grief exposure, relational attachment, and cumulative occupational strain.
A central contribution of the present study lies in the way the qualitative findings help explain and contextualize the quantitative pattern. The mixed-methods approach added interpretive value because the quantitative findings alone could describe the coexistence of moderate subjective happiness and mental well-being alongside elevated depressive symptoms, but could not explain how participants made sense of this pattern in the context of repeated exposure to death. Conversely, the qualitative findings alone could illuminate existential reflection, culturally mediated meaning, and blurred professional-personal boundaries, but could not show how common this broader pattern was across the sample. Themes of existential reflection, culturally mediated meaning, and blurred professional-personal boundaries suggest that palliative care nurse practitioners do not encounter death merely as an isolated clinical event. Instead, they repeatedly integrate exposure to dying into their moral, emotional, and professional worlds. Emotional adaptation to end-of-life care should therefore not be mistaken for emotional immunity. The present findings align with broader literature describing end-of-life care as emotionally demanding and relationally complex work. Palliative care clinicians routinely witness decline, accompany patients and families through dying trajectories, and continue to process grief after death. Brown’s (2022) concept of the “Caregiver’s Conflict” captures this burden, emphasizing that the emotional toll lies not only in the fact of death itself, but also in the experience of proximity, attachment, and aftermath. Similar dynamics have been documented in studies linking death work to emotional strain, meaning, and professional quality of life among helping professionals (Chan et al., 2016, 2022; Chiew et al., 2025; Crape et al., 2025; Czernecki et al., 2025; Lind et al., 2022; Tan et al., 2025). The current findings extend this literature by suggesting that moderate subjective happiness and mental well-being do not preclude the presence of elevated depressive symptoms, and that the emotional realities of palliative practice may be layered rather than uniform.
The relationship between nurses and death is inherently multifaceted. As Johansson and Lindahl (2011) describe, nurses often move “between life and death,” adapting continuously to shifting clinical and emotional realities. In this context, attitudes toward death are not static personal positions but evolving responses shaped by prior experience, education, organizational culture, and the nature of clinical encounters. Previous literature suggests that such attitudes may either mitigate or intensify distress, depending on how death is understood, discussed, and integrated into professional life (Cybulska et al., 2022; Fernández-Gutiérrez et al., 2024; Gama et al., 2012; Lange et al., 2008; Peters et al., 2013; Wong et al., 1994; İnci & Koraş Sözen, 2024). The present study supports this view. Participants’ narratives suggested that death was not experienced solely as a clinical endpoint, but also as an existential, relational, cultural, and symbolic reality. This broader framing may partly explain why palliative care nurse practitioners can experience both meaning and burden in parallel.
The qualitative findings reinforce this interpretation. Temporal reflections on death, existential self-reflection, and the blurring of professional and personal boundaries indicate that repeated exposure to dying may become internalized over time. Participants did not describe death merely as something that occurs to patients. Rather, they described a repeated and cumulative engagement with death that shaped how they understood themselves, their work, and their own mortality. In this sense, palliative care practice appears to require not only clinical skill but also ongoing emotional and existential processing. The emotional impact of such work may therefore be cumulative, even among highly skilled and committed clinicians.
Coping responses in this setting appear to involve both individual and organizational processes. Existing literature remains divided regarding the relative contribution of personal self-awareness and self-care compared with institutional support and structured workplace responses (Ablett & Jones, 2007; Galiana et al., 2022; Koen et al., 2011; Sansó et al., 2015). On one hand, clinicians may rely on personal coping strategies, meaning, spirituality, or professional identity to sustain themselves in demanding settings. On the other hand, these personal resources may be insufficient in the absence of formal organizational recognition of the emotional burden associated with repeated exposure to death. The present findings support the view that both levels matter. Results from the Subjective Happiness Scale, the Mental Health Continuum-Short Form, and the Center for Epidemiologic Studies Depression Scale jointly suggest a meaningful burden of elevated depressive symptoms. These findings reinforce the need for systematic monitoring and tailored support for palliative care nurse practitioners rather than reliance on informal resilience alone.
Terror Management Theory may provide a useful interpretive view for understanding some of these findings, particularly those related to mortality awareness, meaning, cultural framing, and professional identity. According to Terror Management Theory, awareness of mortality may generate existential threat, which individuals manage through symbolic systems of meaning, close relationships, and affirming roles or identities that provide stability and value (Arndt et al., 2002; Greenberg & Arndt, 2012). However, the theory was not directly tested in this study, as the design did not include measures of mortality salience, worldview defense, or self-esteem buffering. Accordingly, Terror Management Theory should be viewed here as a heuristic and interpretive framework rather than as an empirically verified explanatory model.
Even with that caution, the theory helps illuminate important features of the findings. Cultural worldviews were reflected in participants’ references to tradition, collective memory, and social rituals surrounding death, all of which appeared to provide structure and continuity in the face of mortality. Relational buffers were evident in participants’ descriptions of deep bonds with patients and families and in their emphasis on connection, presence, and the hope for a good death grounded in love and meaning. Professional identity may also have served as a buffer when participants portrayed their role as one of skilled accompaniment, moral responsibility, and presence at the end of life. At the same time, the recurrence of intrusive reflections, including imagining one’s own death or questioning life’s meaning, suggests that mortality-related awareness may remain active in this role despite these buffering processes. This may help explain why depressive symptoms can persist even when meaning and professional commitment remain intact.
The cultural setting of the study further strengthens this interpretation. In the Israeli context, tradition and collective memory, including references to Holocaust Memorial Day, appeared to provide especially salient frameworks through which death was interpreted and emotionally processed. Yet these frameworks did not eliminate vulnerability. Rather, they appeared to coexist with broader existential concerns, including questions about the afterlife, the value of life, and the meaning of mortality more generally. This suggests that cultural and symbolic systems may help structure and contain mortality awareness without fully resolving its psychological impact. For palliative care nurse practitioners, the experience of repeated exposure to dying may therefore be shaped not only by professional demands but also by the wider cultural narratives available for understanding death.
The findings should also be interpreted in light of the historical moment in which the data were collected. Because data collection occurred during the later phases of the COVID-19 pandemic, participants were practicing within a context of heightened workload, staffing instability, cumulative loss, and prolonged uncertainty (Braquehais et al., 2020; Coppola, 2021; Gebhard et al., 2022; Parent-Lamarche et al., 2024). These conditions may have intensified distress and should not be treated as incidental background factors. Pandemic-era healthcare work likely amplified both the emotional demands of end-of-life care and the difficulty of recovery from repeated exposure to dying. As such, the depressive symptom burden observed in this study may reflect not only the enduring realities of palliative care practice but also the added strain of a historically exceptional period.
Strengths and Limitations
This study has important strengths and limitations. A major strength is its mixed-methods design, which combined standardized measures with qualitative insights to provide a broader understanding of palliative care nurse practitioners’ psychological well-being and their experiences of repeated exposure to death and dying. Another strength is the focus on a small and understudied national workforce. Rigor was supported through validated quantitative measures and qualitative strategies including reflexive thematic analysis, audit trail documentation, and investigator triangulation.
Several limitations should be noted. The quantitative component was based on a small sample, lacked a comparison group, and used a cross-sectional design, limiting causal inference. Findings should therefore be viewed as preliminary and hypothesis-generating. The study also relied on self-report measures, which may be influenced by reporting bias or social desirability, and the depression measure was a screening rather than a diagnostic tool. In addition, the qualitative component was based on a single focus group, limiting the breadth of perspectives and transferability. Finally, data were collected during the COVID-19 period, and pandemic-related stressors may have influenced emotional burden and interpretation of experiences. Without pre-pandemic comparison data, these effects cannot be fully separated from role-related features of palliative nurse practitioner work.
Implications for Practice
The findings have practical implications for the organization of palliative care work and for the support of advanced practice nurses who repeatedly accompany patients and families through dying (National Academies of Sciences, Engineering, and Medicine, 2021; Parent-Lamarche et al., 2024). First, emotional burden should be addressed as an expected occupational exposure rather than as an individual weakness or a private coping problem. Routine workforce support for palliative care NPs should include structured opportunities for reflective debriefing, peer consultation, and facilitated discussion of difficult deaths, especially after emotionally intense patient trajectories or cumulative loss.
Second, the proportion of participants with elevated depressive symptoms supports the need for proactive monitoring and referral pathways. Screening should not be used punitively or as a measure of professional suitability, but as part of a confidential occupational health approach that normalizes help-seeking and enables early support. Managers should be trained to recognize signs of cumulative distress, moral strain, and grief spillover, particularly when clinicians continue to function at a high professional level while carrying substantial emotional burden.
Third, practice environments should protect time for recovery, supervision, and interdisciplinary meaning. Palliative care teams often rely on personal resilience and informal collegial support, but the present findings suggest that informal support is not sufficient (Crape et al., 2025; Czernecki et al., 2025; Tan et al., 2025). Institutional policies should embed reflective practice, access to mental health resources, bereavement-sensitive team routines, and leadership attention to workload and staffing. For nurse practitioner education and continuing professional development, curricula should include death-related self-reflection, boundary work, cultural meanings of death, and strategies for sustaining professional meaning without romanticizing resilience.
Finally, organizations should treat palliative care NP well-being as a quality-of-care issue. Clinicians who are supported emotionally and structurally are better positioned to provide sustained presence, complex communication, symptom management, and family guidance at the end of life.
Conclusions
This mixed-methods study suggests that palliative care nurse practitioners may sustain professional meaning and elements of positive mental well-being while also experiencing substantial depressive symptom burden. The findings should be interpreted cautiously given the small sample, cross-sectional design, single-focus-group qualitative component, and the COVID-19 context of data collection. Even so, the study provides an important signal that repeated exposure to death in advanced palliative nursing practice carries emotional consequences that deserve institutional recognition, structured support, and further longitudinal investigation.
Footnotes
Ethical Considerations
The study was approved by the Institutional Review Board from the Jerusalem College of Technology Ethics Committee (approval no.: 21_014).
Consent to Participate
All participants provided informed consent.
Author Contributions
Conceptualization: A.R. and G. P.; investigation: A.R.; Formal analysis: A.R. and G. P.; writing - original draft: A.R.; Writing - review and editing: A. R. and G. P.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available.