
Abstract
Introduction
Community-based palliative care has been widely studied worldwide, yet the developmental trajectory of this field remains unclear. In this study, we aimed to elucidate current research focuses, emerging hotspots, and trends in community-based palliative care through bibliometric and visual analyses.
Methods
This study involved bibliometric analysis, combined with visual knowledge mapping of the retrieved literature. Data were retrieved from the Web of Science Core Collection for publica1tions from 2015 to 2025. Bibliometric networks were visualized using CiteSpace and VOSviewer. The reporting framework for this study complies with the Preferred Reporting Items for Bibliometric Analysis guidelines.
Results
Overall, 1,180 publications on community-based palliative care were examined. Annual publication output showed a continuous upward trend, with the United States contributing the largest number of publications (330 articles). The institution with the highest research output was the University of Edinburgh. BMC Palliative Care was the most productive journal. Four core research topics were identified: (a) community-based palliative care services and practice; (b) palliative care and health outcomes among older adults with chronic diseases in the community; (c) advance care planning and decision-making; and (d) barriers to and training in palliative care among community health workers.
Conclusion
Publications on community-based palliative care have increased steadily since 2015, indicating growing academic interest in the field. The United States and Western Europe lead this domain, supported by strong presence of prominent researchers and leading research institutions. Several cohesive, high-output author groups have emerged, reflecting the development of well-connected research collaborations. Although existing research primarily centers on four core topics, “interviews,” “framework,” “family physicians,” “lung,” and “dementia” may represent emerging research frontiers.
Introduction
Palliative care (PC) is an approach that improves the quality of life of patients and their families facing challenges associated with life-threatening illness. It prevents and relieves suffering through early identification, accurate assessment, and treatment of pain and other problems, whether physical, psychosocial, or spiritual (Knaul et al., 2018; World Health Organization, 2020). Despite its well-established clinical benefits and status as a global public health priority, the World Health Organization (WHO) reported that only 14% of patients with terminal illness worldwide have access to PC services (World Health Organization, 2020). This gap is even more pronounced in rural settings: 45% of the global population lives in rural areas, yet PC resources and services in these regions remain severely limited (Marshall et al., 2023). The global burden of chronic non-communicable diseases continues to grow, alongside rapid population aging. Against this backdrop, expanding equitable access to PC has become an urgent global public health priority. In particular, community-based palliative care (CBPC) is widely recognized as a core strategy for addressing the global access gap (Kuebler et al., 2024).
Literature Review
The World Organization of Family Doctors recommends delivering PC as a priority through primary healthcare teams in community-based systems (World Organization of Family Doctors, 2014). CBPC supports patients at home or in community facilities through home visits, medical supplies, and telephone follow-up (Hui & Bruera, 2020). Multidisciplinary primary care teams enhance accessibility, feasibility, and cost-efficiency. Compared with institutional care, CBPC is more cost-effective, better aligned with patient preferences, and less burdensome to acute care systems (Hughes et al., 2023; Scott et al., 2024).
Over the past two decades, the evidence base for CBPC has expanded worldwide. Several high-income countries and regions have established relatively mature care models and standardized assessment frameworks (Dale et al., 2009; Hui & Bruera, 2020; Schenker et al., 2021). As an early leader in the modern hospice movement, the UK established a community-led PC model in the 1990s (Coyle et al., 1999), equipping GPs with standardized tools through the Gold Standards Framework (Munday et al., 2007) and integrating CBPC into the national primary care system. The US implemented tiered Medicare payment reforms to create sustainable financial incentives for scalable home-based PC models (Taylor et al., 2018).
China, a developing country, faces compounded challenges: rapid population aging, a growing number of chronic disease patients at the end-of-life, and limited access to PC services (Hu & Feng, 2016). Although policy attention and practical initiatives related to CBPC in China have increased in recent years (H. Lin et al., 2025; Y. Lin et al., 2024), several gaps remain between domestic research and international best practices. These include fragmented research directions, poorly defined core themes, and limited cross-institutional and international collaboration. Further, the lack of systematic reviews has hindered efforts to consolidate the existing knowledge base. These disparities require further validation through comprehensive comparative analyses.
Currently, although a substantial body of research on CBPC exists, bibliometric studies remain scarce. Bibliometrics is a scientific, quantitative method grounded in mathematics and statistics that analyzes specific knowledge carriers (Ninkov et al., 2022). Robust empirical data are essential to clarify the current research landscape, emerging trends, and key thematic areas in this field (Liu et al., 2021). Therefore, herein, we conducted a comprehensive bibliometric and visual analysis of CBPC literature.
We aimed to systematically explore the prevailing themes and evolving trends in CBPC to offer evidence-based insights for informing future research and clinical practice in this field. The analysis aimed to cover publications from 2015 to 2025, using data sourced from the Web of Science Core Collection (WoSCC), to characterize publication patterns and research productivity in this field.
Specifically, we aimed to: (a) provide a comprehensive overview of CBPC research over the past decade, including temporal, geographic, institutional, journal, author, keyword, and co-citation distributions; (b) examine cross-national author collaboration patterns; and (c) elucidate core research themes and their evolutionary trajectories.
Methods
Data Source
The WoSCC (Clarivate Analytics, Philadelphia, PA, USA) indexes over 21,000 peer-reviewed journals across disciplines. Known for its citation indexing, it is widely used in bibliometric research. The WoSCC was searched on October 29, 2025. The retrieved records included titles, authors, publication years, journals, countries/regions, keywords, abstracts, and cited references. CiteSpace (version 6.3. R1) and VOSviewer (version 1.6.20) were used to analyze the data and visualize research trends and intellectual structures.
Retrieval Strategy
Data were retrieved from the WoSCC using the following search strategy: (TS=(“Community” OR “Community Hospital” OR “Community Health Centers” OR “Neighborhood Health Centers” OR “Community Health Services” OR “Community Health Care” OR “Community Healthcare” OR “Community Health Nursing”)) AND TS=(“Hospice and Palliative Care Nursing” OR “Palliative Care” OR “Palliative Medicine” OR “Hospice Care” OR “Terminal Care” OR “Hospices” OR “end-of-life care” OR “supportive care”) AND Article (Document Type) AND English (Language).
The search was restricted to peer-reviewed journal articles published between January 1, 2015 and October 29, 2025. Two researchers independently screened the retrieved records by title and abstract. Disagreements were resolved through discussion with a third researcher until consensus was reached.
Data Analysis
Bibliographic characteristics of the selected publications, including year of publication, geographic origin, affiliated institutions, and source journals, were examined using the “Analyze Results” tool in the WoSCC. To illustrate temporal trends and distribution patterns, graphical outputs, including bar charts and line graphs, were generated using Microsoft Excel (version 2016, Microsoft Corporation, Redmond, Washington, United States).
CiteSpace (version 6.3. R1), a Java-based application developed by Chen (2006) for visualizing and analyzing bibliometric networks, was used to identify research fronts and collaboration patterns. Raw data retrieved from the WoSCC were exported in plain text format and saved as download_*.txt. These files were imported into CiteSpace for keyword burst detection and co-citation network analysis. The analysis parameters were set as follows: time span, 2015–2025; years per slice, 1; and selection criteria combining the g-index, k=25; and Top N=50. To evaluate the reliability of the cluster structures derived from co-citation analysis, CiteSpace provides two metrics: modularity (Q) and mean silhouette value (S). A Q value >0.3 suggests meaningful partition of the network into distinct clusters. The S value ranges from -1 to 1, with an average >0.5 indicating coherent and well-matched items within each cluster (Chen et al., 2015). The log-likelihood ratio was applied to interpret the thematic content of each cluster by identifying the associated characteristic and distinguishing terms.
VOSviewer (version 1.6.20), a bibliometric mapping software developed at Leiden University (Van Eck & Waltman, 2010), was used to visualize keyword co-occurrence networks and thematic clusters. Bibliographic data were imported in plain text format. The analysis was configured using the following parameters: fractional counting method and a minimum keyword occurrence threshold of 15. This threshold was applied to exclude low-frequency keywords, ensuring that only representative terms were retained for network construction. For other parameters, default settings were retained. This bibliometric analysis was conducted in accordance with the Preferred Reporting Items for Bibliometric Analysis guidelines.
Ethics Statement
Ethical approval was deemed unnecessary as this study did not involve any human or animal subjects.
Results
Literature Distribution Characteristics
The initial search identified 1,659 publications. After duplicates were removed and titles and abstracts were screened against the inclusion criteria, 1,180 articles were included in the final analysis (Figure 1). They originated from 93 countries/regions. Flowchart of literature screening
As shown in Figure 2a, annual publication output increased steadily from 2015 to 2025. Figure 2b presents the geographic distribution of research output and the top 20 contributing countries/regions. (A) Annual publication volume in community-based palliative care research (2015–2025); (B) Top 20 productive countries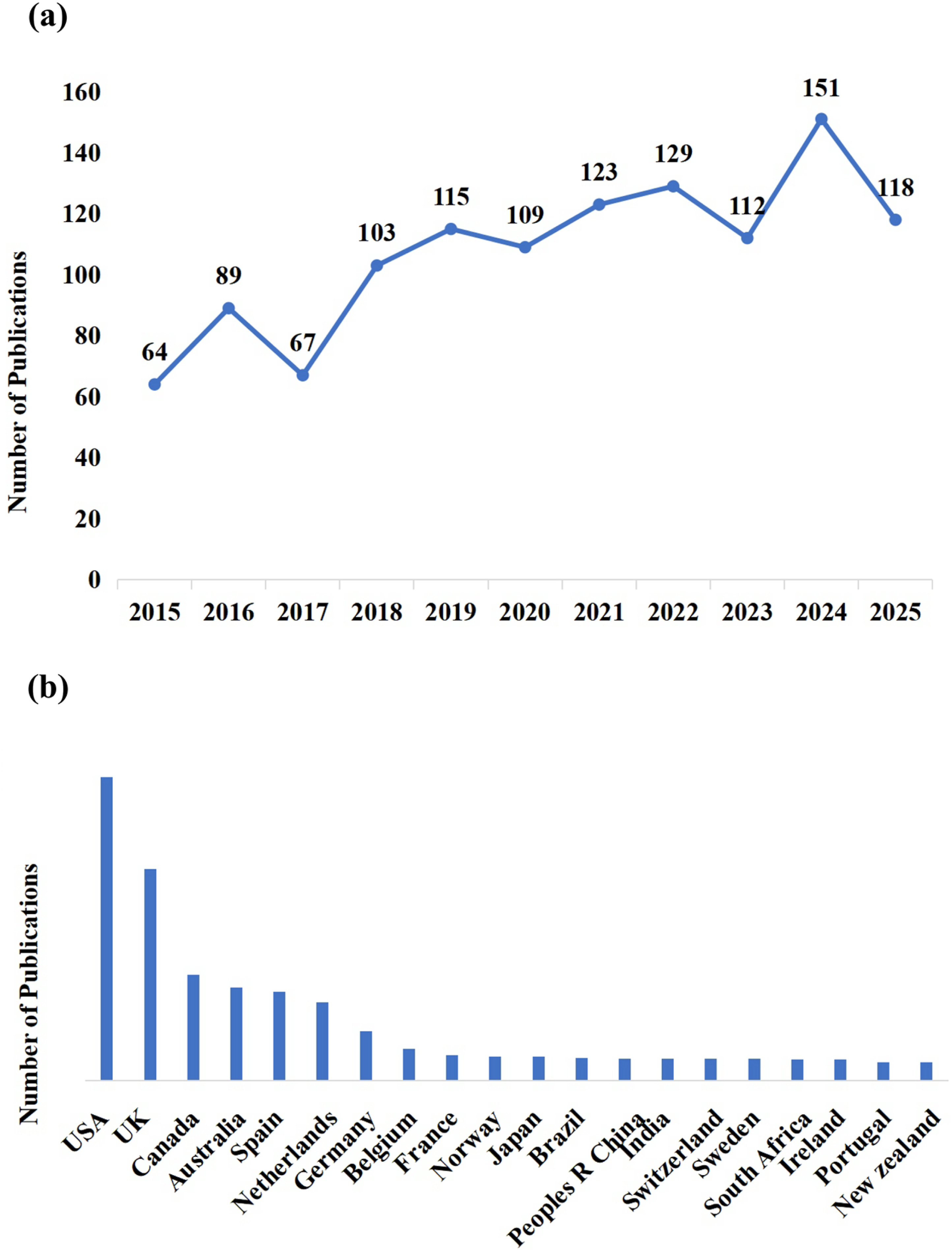
Top 20 Prolific Institutions (n=1,180)


Visualization of the institutional collaboration network
The most productive journal was BMC Palliative Care (Table S1). The most co-cited journal was Palliative Medicine (Impact Factor: 3.9) (Table S2).
Analysis of Authors and Co-Authors
VOSviewer was used to analyze author productivity and collaboration patterns in the field of CBPC (Figure S1). Co-authorship analysis was performed to identify key contributors and their collaborative networks. Four authors were the most productive in the field: Nils Schneider (n=17), Murray SA (n=15), Onwuteaka-Philipsen BD (n=15), and Luc Deliens (n=14).
The author with highest co-citations in this network was Murray SA (175 citations; link strength, 1224), followed by Gomes B (160 citations; link strength, 959). Their strong link strength confirms frequent co-citation, reflecting closely aligned intellectual foundations in CBPC research. Their prominent nodes and robust interconnections establish them as central figures in the co-citation landscape.
Keyword Co-Occurrence and Research Hotspots
A keyword co-occurrence network was constructed using VOSviewer. From an initial pool of 3,452 keywords, 117 terms with >15 occurrences were selected. After a detailed review, no duplicate keywords were identified. Consequently, 117 high-frequency keywords were retained, forming a network with 4,097 links (Table S3). The top five were “palliative care” (n=701), “primary care” (n=251), “cancer” (n=186), “end-stage” (n=165), and “primary health care” (n=152).
Four distinct clusters were identified based on high-frequency keywords, each representing a core research theme (Figure 4). The cluster solution generated by CiteSpace yielded a Q value of 0.415 and a mean S value of 0.742, indicating a statistically acceptable modular structure with good cluster coherence. Cluster 1 (green): CBPC service and practice; Cluster 2 (red): PC and health outcomes among older adults with chronic diseases in the community; Cluster 3 (blue): advance care planning (ACP) and decision-making; Cluster 4 (yellow): barriers and Training of PC in community health workers (CHWs). Network map of high-frequency keywords for community-based palliative care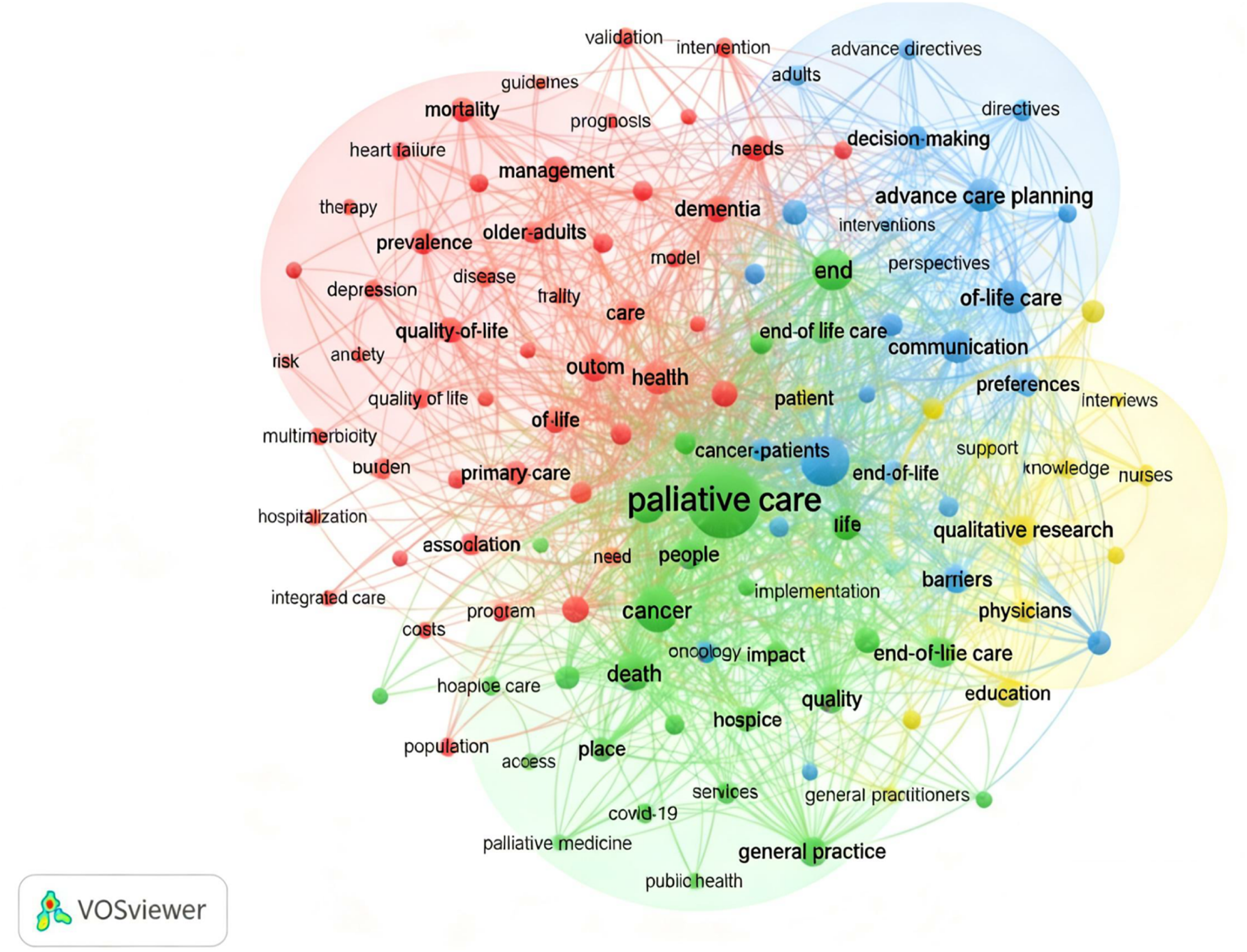
Burst Detection
Keyword burst detection was performed on 1,180 articles to identify emerging research trends. Figure 5 presents the 30 keywords with the strongest burst strength, arranged by the beginning year for each burst. The timeline is represented by a blue bar, and red segments indicate periods of heightened activity, reflecting duration of each burst. For each keyword, the figure displays the time interval and corresponding burst intensity. Keyword bursts in articles on community-based palliative care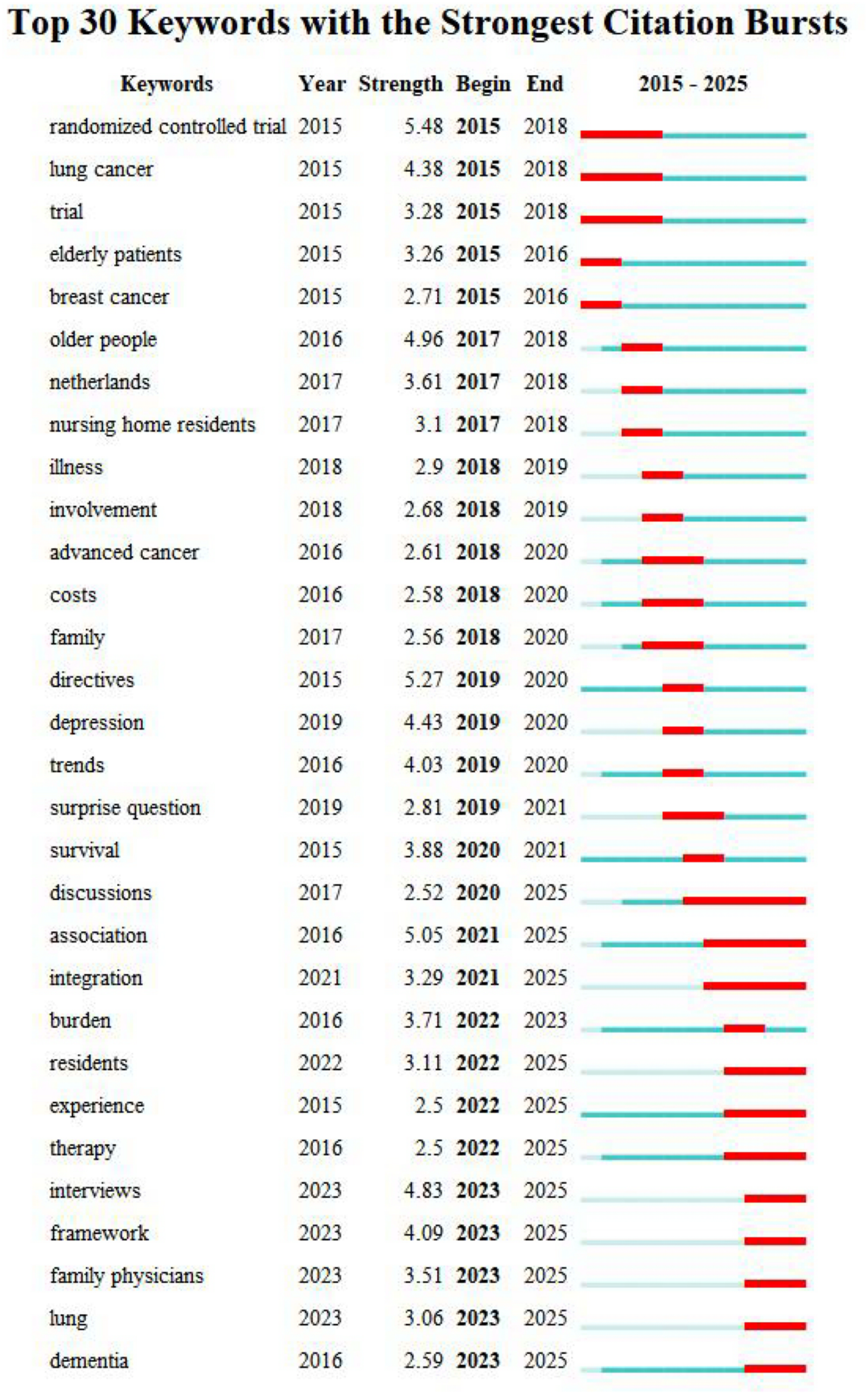
Within the analysis period (2015–2025), the earliest keyword to exhibit a burst was “randomized controlled trial,” whereas “discussion” had the longest duration, remaining active for 5 years. In terms of burst strength, the five highest values were observed for “randomized controlled trial,” “directives,” “association,” “older people,” and “interviews,” with strengths of 5.48, 5.27, 5.05, 4.96, and 4.83, respectively. Since 2023, keywords such as “interviews,” “framework,” “family physicians,” “lung,” and “dementia” have emerged as new bursts, suggesting potential future directions in CBPC research.
In addition to the findings presented in Figure 5, CBPC research can be divided into three distinct stages. The initial stage (2015–2018) focused on evaluating the clinical effectiveness and feasibility of CBPC for specific critically ill populations, particularly patients with cancer. During the second stage (2019–2022), research expanded beyond disease-centered interventions to encompass broader aspects, including decision-making in diagnosis and treatment, patients’ psychological and social needs, and support for family systems. The third and most recent stage (2023–2025) emphasizes the systematic integration of PC into the broader healthcare system, with the aim of serving a more diverse patient population while advancing the scientific framework for implementation.
Top Co-Cited Reference Analysis
Analysis of the co-citation network allows examination of development and evolution of specific research domains (Liu et al., 2023). Using CiteSpace, we constructed and analyzed a co-cited network for CBPC. The five most frequently co-cited references are authored by Terry G, Sleeman KE, Kim GM, Sleeman KE, and Clark D. A report predicted that by 2,040 more people in England and Wales will need PC, mainly due to rising deaths from dementia and cancer; this report has the highest centrality (Etkind et al., 2017). References were clustered by title, and the top five clusters identified were “primary care,” “advance directives,” “dementia,” “primary healthcare,” and “quality of care” (Figure S2).
Discussion
Although annual publication volumes fluctuated slightly, research on CBPC maintained a steady upward trajectory over the past decade. Notably, the number of related studies increased from 2015 (n=64) to October 29, 2025 (n=118), and this trend is likely to continue in the coming years. This growth reflects increasing academic attention to PC delivered in primary health settings, driven by the escalating chronic diseases burden and rapid population aging (Naghavi et al., 2024).
In terms of publication output, the US and the UK lead globally. This leadership appears to be supported by early policy commitment, sustained funding, concentrated institutional expertise, and systematic workforce development.
The UK pioneered the modern hospice movement by founding St Christopher’s Hospice in 1967 (Redwine & Ganti, 2024), thereby embedding PC into the National Health Service. The US introduced the Medicare Hospice Benefit in 1982 (Mor & Teno, 2016), creating a federal reimbursement mechanism.
Strong academic infrastructure underpins the substantial research output of both countries. Over half of the world’s top 10 high-impact institutions are located in the US, while the UK hosts leading contributors such as University of Edinburgh. This concentration of expertise reinforces their global leadership in CBPC. Both countries have established formal training systems to cultivate interdisciplinary professionals.
Within CBPC research, several stable and highly productive core author clusters have emerged. Notably, the collaborative network linking the University of Edinburgh and University of Cambridge has demonstrated high publication productivity. This team has focused primarily on optimizing CBPC service delivery (Mitchell et al., 2022; Turner et al., 2023) and examining end-of-life care practices and patient experiences in community settings (Boyd et al., 2010; Mason et al., 2016). Such inter-institutional collaboration facilitates the sharing of research resources, exchange of specialized expertise, and integration of innovative perspectives, which are critical to advancing CBPC research.
Overall, contemporary research on CBPC remains concentrated in high-income regions, particularly the US and Western Europe. Research output from developing countries remains limited, a gap that may reflect structural disparities. High-income countries established PC systems earlier, have greater research funding availability, maintain larger groups of specialized researchers, and receive stronger governmental support and policy prioritization (Clark et al., 2020).
Digital Health Integration: An Emerging Frontier (2023–2025)
Beyond the thematic clusters identified in our analysis, the 2023–2025 period has seen a notable acceleration in digital health integration within CBPC research. Telehealth, remote monitoring, and artificial intelligence (AI) are increasingly shaping the service models and frameworks highlighted herein.
Early empirical studies laid the foundation for this transformation. Udelsman et al. (2019) demonstrated that combining natural language processing with administrative codes enables rapid identification of seriously ill patients who might otherwise be difficult to identify, eliminating the need for labor-intensive manual chart review.
Building on these foundational efforts, recent evidence has broadened the scope of digital health applications. A 2025 systematic review demonstrated that telehealth interventions improve functional status, reduce hospitalizations, alleviate psychological distress, and lessen caregiver burden (Haroen et al., 2025). However, the evidence base remains concentrated in high-income countries, limiting its generalizability. Despite these promising advances, the application of AI in PC remains at an early stage. Although AI has shown considerable potential in areas such as prognostic assessment and medical record support, important challenges remain, including limited validation, a lack of cross-institutional testing, and insufficient transparency (Bozkurt et al., 2025). These issues hinder clinical implementation. Future research should prioritize rigorous external validation, use large patient datasets, and adopt open science approaches to ensure the reliability, safety, and credibility of AI-based tools.
In response to these challenges, digital technologies are reshaping CBPC service models. The EMBED-Care Framework for palliative dementia care digitally combines holistic assessment with clinical decision support, advancing from proof-of-concept to clinical deployment (Davies et al., 2025). Digital advance care planning (DACP) has also progressed, with the Optimal Care recommendations emphasizing interoperability and integration of DACP into routine organizational structures (Allsop et al., 2025).
Collectively, these advances indicate that digital health is reshaping CBPC service delivery. The field has progressed from early predictive models to integrated frameworks that embed clinical decision support into platform-based models. Future research should prioritize evaluating these interventions across diverse settings. A focus on human-centered design is essential to ensure that digital transformation promotes health equity rather than exacerbating disparities.
Main Theme Distribution and Research Frontiers
Analysis of high-frequency keywords helps identify the core research focus areas within the field of CBPC (Gainollina et al., 2025). Burst detection analysis identified several emerging terms, including “dementia,” “lung,” “family physicians,” “framework,” and “interviews,” highlighting potential future directions in CBPC research. Based on analyses of the keyword co-occurrence network and cited references, we identified four core research topics in CBPC research.
Cluster 1: CBPC Service and Practice
The first keyword cluster in this study centers on PC, cancer, hospice care, palliative medicine, medical services, and general practice. Keyword frequency and topic association analyses indicate that current research hotspots include PC models for patients with chronic diseases, the central role of general practitioners (GPs) in service delivery, and development of multidisciplinary collaboration mechanisms.
Evidence indicates that most patients with terminal illness prefer home-based hospice care (Higginson & Sen-Gupta, 2000), a preference that has driven global development of CBPC service models. Despite this growth in practice, PC research has lagged behind and seldom included CBPC populations. PC for patients with advanced dementia has largely been confined to institutional settings. Recent findings, however, show that an embedded community care model led by Advanced Practice Registered Nurses (APRNs) reduced combined emergency department visits and hospitalizations among patients with dementia by 55% (risk ratio=0.45, 95% confidence interval: 0.31–0.65) (Fasolino et al., 2024). This finding supports the core value of APRN-led models in community-based dementia PC while also highlighting competency gaps within primary care teams. Nursing administrators should therefore strengthen community-integrated care capacity at the systems level, expand APRN practice scope through regulatory reform, and establish corresponding payment mechanisms. Beyond dementia care, precision care models for advanced non-cancer chronic diseases continue to evolve (Sánchez-Cárdenas et al., 2023). In keyword frequency analysis, “GPs” appeared 42 times, underscoring their navigator role and critical linkage among patients, specialists, and community systems.
Based on the identified hotspots and gaps, future efforts should focus on two directions. First, research should develop and validate CBPC models tailored to underserved populations, including patients with non-cancer chronic diseases, rural residents, and ethnic minority groups, to reduce disparities in PC access. Second, studies should use rigorous scientific methods to examine the policy, funding, and training systems needed to strengthen the competencies of primary care providers, such as GPs and APRNs, supporting large-scale implementation of CBPC.
Cluster 2: PC and Health Outcomes in Older Adults With Chronic Diseases in the Community
The cluster, defined by the core keywords “older adults,” “mortality,” “heart failure,” “frailty,” “quality of life,” “depression,” and “primary care,” focuses on CBPC for community-dwelling older adults with chronic life-limiting illnesses. It reflects two global shifts: the epidemiologic transition toward chronic non-malignant diseases as the leading cause of death in elders and limitations of traditional cancer-centric PC models in addressing the fluctuating and long-term care needs of this population.
Existing evidence reveals marked inequities in access to care. Compared with patients with cancer, older adults with non-cancer life-limiting illnesses are much less likely to receive specialized PC across all settings, and they often experience substantial delays in care initiation (Quinn et al., 2021; Qureshi et al., 2018; Rosenwax et al., 2016). These disparities are not attributable to lower clinical need. Advanced heart failure and similar chronic conditions involve progressive functional decline and increasing needs for symptom management, psychological support, and social care (Gelfman et al., 2024). These barriers arise from modifiable systemic factors, including workforce shortages, inadequate training in non-malignant PC, limited community healthcare resources, and insufficient multidisciplinary infrastructure, which are especially pronounced in rural China. Additionally, eligibility criteria and reimbursement structures remain skewed toward cancer diagnoses, constraining equitable access to CBPC for patients with non-cancer life-limiting conditions (Dussault et al., 2025). Collectively, these barriers have made the expansion of equitable access to CBPC a critical global health policy priority.
In a cross-disease study of end-of-life preferences among community-dwelling older adults, Kenny et al. (2024) found that patients consistently prioritized financial burden, symptom severity, and caregiver strain, findings that directly reflect the systemic gaps outlined above. Future research should prioritize the development of effective strategies for managing complex symptoms, thereby improving quality of life for patients and their caregivers, and the rigorous evaluation of policy and health system interventions aimed at reducing access inequities for this population.
Cluster 3: ACP and Decision-Making
This research cluster is anchored by the core keywords “ACP,” “communication,” “qualitative research,” “decision-making,” and “patient preferences.” As global population aging intensifies, community and home-based care have become preferred options for many older adults. ACP helps clarify individuals’ care preferences in advance, helping ensure that they receive high-quality care aligned with their wishes when their health deteriorates. Consequently, ACP has received increasing attention in recent years.
ACP is defined as a structured process designed to help individuals clarify their care values and preferences, communicate these with family members and healthcare providers, and document future care plans (Mori et al., 2025). Effective communication among stakeholders is fundamental to delivering high-quality, patient-centered ACP (Pfeifer & Head, 2018). The prominence of qualitative research in this field reflects the need to understand context-dependent and highly personal decision-making processes that quantitative methods alone cannot fully capture.
Globally, ACP research remains concentrated in North America, Europe, and Oceania, with limited empirical evidence from Asia and the Middle East. This geographic imbalance reflects cross-regional differences in policy frameworks, cultural norms, and research investment. In high-income Western countries, ACP is supported by formal legislation, clear policy guidance, and a cultural emphasis on individual autonomy. In contrast, the actual participation rate in ACP among family members in Asian societies remains low. This pattern is associated with incomplete ACP legislation, limited public education, and the influence of Confucian values or traditional beliefs (Lee et al., 2024; Zhang et al., 2021).
Future research should prioritize culturally adapted communication strategies to strengthen ACP engagement across diverse populations, along with rigorous evaluations of implementation models that integrate ACP into routine community care. Particular attention should be paid to effects of family dynamics, health literacy, and digital tools on decision-making, especially in non-Western cultural contexts where collective decision-making is normative.
Cluster 4: Barriers and Training of PC in CHWs
This cluster is centered on core keywords, including “nurses,” “physicians,” “qualitative research,” “barriers,” “knowledge,” and “education,” reflecting its twofold focus: barriers faced by frontline community health workers (CHWs) in delivering PC, and targeted training to strengthen their service competencies. Training is a well-documented strategy for improving the PC capabilities of frontline providers (Monton et al., 2024); the prominence of qualitative research within this cluster reflects the need to understand context-specific barriers to CHWs’ practice, which remain poorly understood globally.
As the primary providers of CBPC, community physicians and nurses often lack essential PC competencies. This competency gap has become a major barrier to equitable access to CBPC services. Evidence indicates that <5% of specialist PC APRNs have completed standardized specialty training (Pawlow et al., 2018); this gap is even more pronounced among non-specialist CHWs, who provide most frontline care. In China, CHWs, rather than specialists, provide most PC. Globally, standardized training systems tailored to the practice needs of CHWs in CBPC remain limited.
Systemic barriers further exacerbate these gaps and directly impede the translation of CHWs’ training outcomes into clinical practice. These barriers include underinvestment in CBPC support infrastructure, lack of formal two-way specialist referral pathways, inadequate multidisciplinary collaboration mechanisms, and absence of unified clinical standards for CBPC (Anonjarn & Matchim, 2025).
Future research should address these barriers by designing and rigorously evaluating multi-level, targeted interventions for CBPC. First, grounded in qualitative insights into CHWs’ real-world practice challenges, studies should co-develop context-specific PC training curricula for CHWs, using combined simulation and online learning models to improve training effectiveness and accessibility (Chen et al., 2021; Ellman et al., 2012). Second, multi-center empirical studies should systematically collect implementation evidence on CBPC services and translate the findings into policy-focused decision-support tools for resource allocation and service design, thereby informing health system reform and improving the sustainability and equity of CBPC services.
Strengths and Limitations
A key strength of this study is the use of established bibliometric tools, including CiteSpace and VOSviewer, to examine publication patterns, collaboration networks, and thematic development in a systematic manner. Despite its rigorous design, this bibliometric study has some inherent limitations. Our search was limited to publications in English indexed in the WoSCC. This ensured consistency in data quality and compatibility with bibliometric analysis tools. This exclusion criterion likely omitted relevant non-English publications and grey literature, thereby compromising the global representativeness of our findings—particularly in regions where English is not the primary language of scholarly communication. Future studies should consider incorporating multilingual databases (e.g., Scopus, PubMed) and grey literature Additionally, the exclusion of non-article publication types, such as reviews, conference proceedings, and books, may have resulted in omission of relevant research contributions. Future studies should incorporate diverse document types to achieve a more comprehensive understanding of the field. Although CiteSpace and VOSviewer are empirically validated, subjective parameter choices and the continuous updating of the WoSCC may introduce variability and database-related bias. Despite these limitations, the literature included herein represents the core body of research in the field and reflects current research hotspots and trends effectively.
Implications for Practice
This bibliometric analysis provides a comprehensive view of the CBPC research landscape from 2015 to 2025 and highlights several actionable directions for nursing administrators, educators, and policymakers.
A central challenge identified herein is the persistent competency gap among frontline providers, particularly CHWs and GPs. Strengthening PC training at community level is essential. Educational initiatives should extend beyond didactic instruction to include simulation-based and online learning models that build practical skills in symptom management, ACP communication, and care coordination during hospital-to-home transitions. Training should incorporate culturally sensitive communication strategies tailored to contexts in which family-centered decision-making is the norm.
The findings also underscore the value of APRN-led community care models. Nursing administrators and policymakers should pursue regulatory reforms expanding APRN scope of practice and establishing sustainable payment mechanisms for multidisciplinary CBPC. Without these structural supports, even well-designed models may struggle to achieve sustainability or scale.
Equally important is the need to address persistent inequities in care access. Patients with non-cancer chronic conditions and those living in rural areas remain significantly underserved. Policy reforms should broaden eligibility criteria and adjust reimbursement structures to move beyond a cancer-centric framework, thereby integrating PC into primary care and chronic disease management pathways.
The growing role of digital health, including telehealth, remote monitoring, and AI-based decision support, offers new opportunities to expand reach and improve care coordination. Providers should be trained to use these tools effectively, and digital infrastructure should be strengthened to prevent technology from widening existing disparities, particularly in rural and underserved communities.
Collectively, these actions support the transformation of CBPC from a cancer-focused, hospital-based service into an integrated, multidisciplinary system that meets the needs of patients with life-limiting illnesses across diverse community settings.
Conclusions
Nursing research plays a critical role in advancing CBPC and offers important opportunities for progress, particularly through strengthening primary care capacity and integrating advanced practice roles. Countries including the US, UK, and Canada have made substantial contributions to this field. Among institutions, the University of Edinburgh in the UK has the highest publication output. Recent evidence underscores the value of APRN-led models and highlights the urgent need to address competency gaps among CHWs. Advancing the field requires stronger international collaboration, especially between developed and developing countries, to enable knowledge exchange and contextual adaptation of CBPC models. Future efforts should prioritize the development of culturally sensitive communication strategies for ACP, establishment of sustainable payment mechanisms for multidisciplinary community care, and investment in training programs to strengthen the skills of frontline healthcare providers. Collectively, these measures may improve equitable access to quality PC for underserved populations.
Supplemental Material
Supplemental Material -Community-Based Palliative Care: A Bibliometric and Visual Analysis of Scientific Publications (2015–2025)
Supplemental Material for Community-Based Palliative Care: A Bibliometric and Visual Analysis of Scientific Publications (2015–2025) by Qin YU, XiaoJin Wei and XiaoJing Xue in Sage Open Nursing.
Footnotes
Acknowledgements
We thank Sage Author Services for professional language editing and formatting support.
Ethical Considerations
Ethical approval was deemed unnecessary as this study did not involve any human or animal subjects.
Author Contributions
Qin YU: paper writing, data analysis and revise manuscript. XiaoJin WEI: study design, data collection and data processing. XiaoJing XUE: data collection and data processing and revise manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Primary Health Development Research Center of Sichuan Province Program, China [grant number SWFZ25-Q-97]; and by the 2025 project of the Health Humanities Research Center, a key philosophy and social sciences research base in Zigong City, China [grant number JKRWZC25-04].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.