
Abstract
Introduction:
Limited evidence exists to support optimal patient-centered management for compromised first permanent molars (cFPMs) in young people. Young people’s preferences are important when planning their health care.
Objectives:
This study aimed to elicit young people’s preferences for pathways to manage cFPMs.
Methods:
An online discrete choice experiment (DCE) was completed by young people (aged 12–16) from the United Kingdom. The design was informed by the literature, interviews with young people, and a concurrent adult-focused DCE. A statistically optimal d-efficient design generated 18 choice tasks across two blocks. Each respondent answered 1 block of 9 tasks. Choice tasks varied across four characteristics: treatment type, care provider, management decision-maker, and number of future visits avoided. An opt-out (no treatment) was included. Conditional (fixed effects) logit models were used for data analysis.
Results:
In total, 122 young people completed the DCE. Restoring a cFPM was preferred to having a partial gap, prosthetic replacement with a bridge, orthodontic closure, or a full-unit gap. Preferences ranged from no preference to a preference for spontaneous closure compared to a restoration (odds ratio = 1.40; 95% confidence interval, 0.98–1.99;
Conclusion:
Young people wished to manage cFPMs and expressed preferences for restorations rather than any other management, resulting in a gap, and for orthodontic or prosthetic closure. They want and should be included as part of a shared decision-making process for these teeth, rather than their preferences being assumed solely by parental proxies. Young people aged 12 to 16 were able to understand and complete this DCE.
Knowledge Transfer Statement:
Young people (aged 12–16) attending primary and secondary care dental clinics in the United Kingdom clearly expressed preferences on how compromised first permanent molars should be managed. They want and should be included as part of a shared decision-making process for these teeth, rather than their preferences being assumed solely by parental proxies.
Keywords
Introduction
It is important to understand children and young people’s preferences when planning their health care. Despite the common belief that young people, as a group, are not mature enough to speak for themselves, many can comprehend their health, hold preferences, and make decisions about their care (Guerriero et al 2018; Taylor et al 2025). Individual preferences inform shared decision-making while population preferences are important when considering policy changes (Brazier et al 2005). Eliciting preferences for and measuring the value placed on dental care treatments by service users supports efficient resource allocation within fixed health care budgets (Brazier et al 2005; Vernazza et al 2021). Identification of service users’ preferences supports the design of health care services, ensuring treatments are patient centered. Parents have preferences for their child’s health care, often derived from their own experiences; however, preferences of children and young people themselves should be explored and understood where possible, as they are experiencing the health condition, will undergo any treatment, and have to live with the outcomes (Powell et al 2021; Taylor et al 2025).
Discrete choice experiments (DCEs) are widely accepted to ascertain preferences for treatments and outcomes of care (de Bekker-Grob et al 2012). DCEs are survey-based tools that ask participants to make multiple choices between 2 or more hypothetical goods or services. Each good/service is described by a set of common characteristics (attributes and levels of those attributes), and each choice is between goods that differ in the levels of the characteristics. Participants answer several sequential scenarios (choice tasks). Based upon the underpinning economic theories of demand (Lancaster 1966) and random utility (McFadden 1974), it is assumed that the utility (value) of any health care good or service is equal to the sum of the utilities attached to each underlying characteristic (Lancsar and Louviere 2008). By combining participants’ answers across multiple choice tasks, the relative importance of the levels of each characteristic and level can be estimated (Lancsar and Louviere 2008).
Widely used in adult health care, including eliciting dental health care provider preferences (Kateeb et al 2016), DCEs are used infrequently to establish young people’s health care preferences (Rowen et al 2020) and even less so in dentistry (Barber et al 2018). DCEs have an advantage over simple ranking or rating methods as the decision-making process for the hypothetical scenarios in a DCE often better reflects real-life choices, capturing trade-offs between attributes and providing more reliable estimates of preferences (Michaels-Igbokwe et al 2021). Similarly, children and young people can make rational choices and are strategic in their decision-making abilities (Sutter et al 2019). In part, this balances concerns about DCEs being too cognitively demanding for children and young people (Sutter et al 2019; Michaels-Igbokwe et al 2021). There is no agreed lower age cutoff for when a DCE should not be used, although an arbitrary age cutoff of 10 years old has been suggested (Rowen et al 2020; Rogers et al 2021). Children and young people may be more susceptible, compared to adults, to social desirability bias (answering what they think is expected of them), primacy (selecting items presented first), recency (making decisions based on the most recent experience), and ordering effects (Michaels-Igbokwe et al 2021). As such, using DCEs with children and young people must be age-appropriate, suitably framed, rigorously piloted, and tailored for the target age group (Michaels-Igbokwe et al 2021; Rogers et al 2021).
Decision-making on the management of compromised first permanent molars (cFPMs) in children and young people is complex. Treatment options can be categorized at a high level as restoration or extraction. However, variation in clinical presentation of cFPMs, individuals’ differing priorities for their oral health, and a paucity of effectiveness studies complicate this decision (Taylor et al 2019; Lygidakis et al 2022). Taylor et al (2025) conducted the first DCE to elicit public (adult) preferences for managing cFPMs in children. However, in a preceding qualitative study, children and young people contrasted adults’ views on management of cFPMs (Taylor et al 2025). With no published DCE directly eliciting young people’s preferences for managing cFPMs, the aim of this study is to elicit UK young people’s (aged 12–16 y) preferences to manage cFPMs.
Methods
This DCE was developed, designed, and analyzed concurrently with a UK adult general public DCE (Taylor et al 2025). Best practice methods’ guidance (Reed-Johnson et al 2013; Hauber et al 2016) and reporting standards for DCEs (Ride et al 2024) were followed. Favorable ethical opinion was obtained from the North of Scotland Research Ethics Service (20/NS/0124; 22/10/2020).
Characteristic and Level Selection
Characteristics and their levels (Table 1) were identified using initial analyses of semi-structured interviews with the young people (aged 12–16 y) from the United Kingdom (Taylor et al 2025), focused literature searches (Appendix A), expert panel opinion (comprising clinical academic, general dentists, secondary care dental clinicians [pediatric, orthodontics, and adult restorative], patients, and policymakers) who were purposively recruited from across the United Kingdom to provide a divergent range of stakeholder views (Taylor 2023), and research team discussions. An advisory group panel, including four young people aged 12 to 16 y (two of whom had experienced cFPMs) identified prestudy from Newcastle Dental Hospital (United Kingdom), validated the chosen characteristics/levels as being the most relevant and important for managing cFPMs. They agreed that no key characteristics were omitted and confirmed the face validity of the DCE. They suggested including photographs in the information/choice tasks for the treatment characteristic (Appendix B). This was incorporated.
Final List of Characteristics (and Levels) Included in the Discrete Choice Experiment.
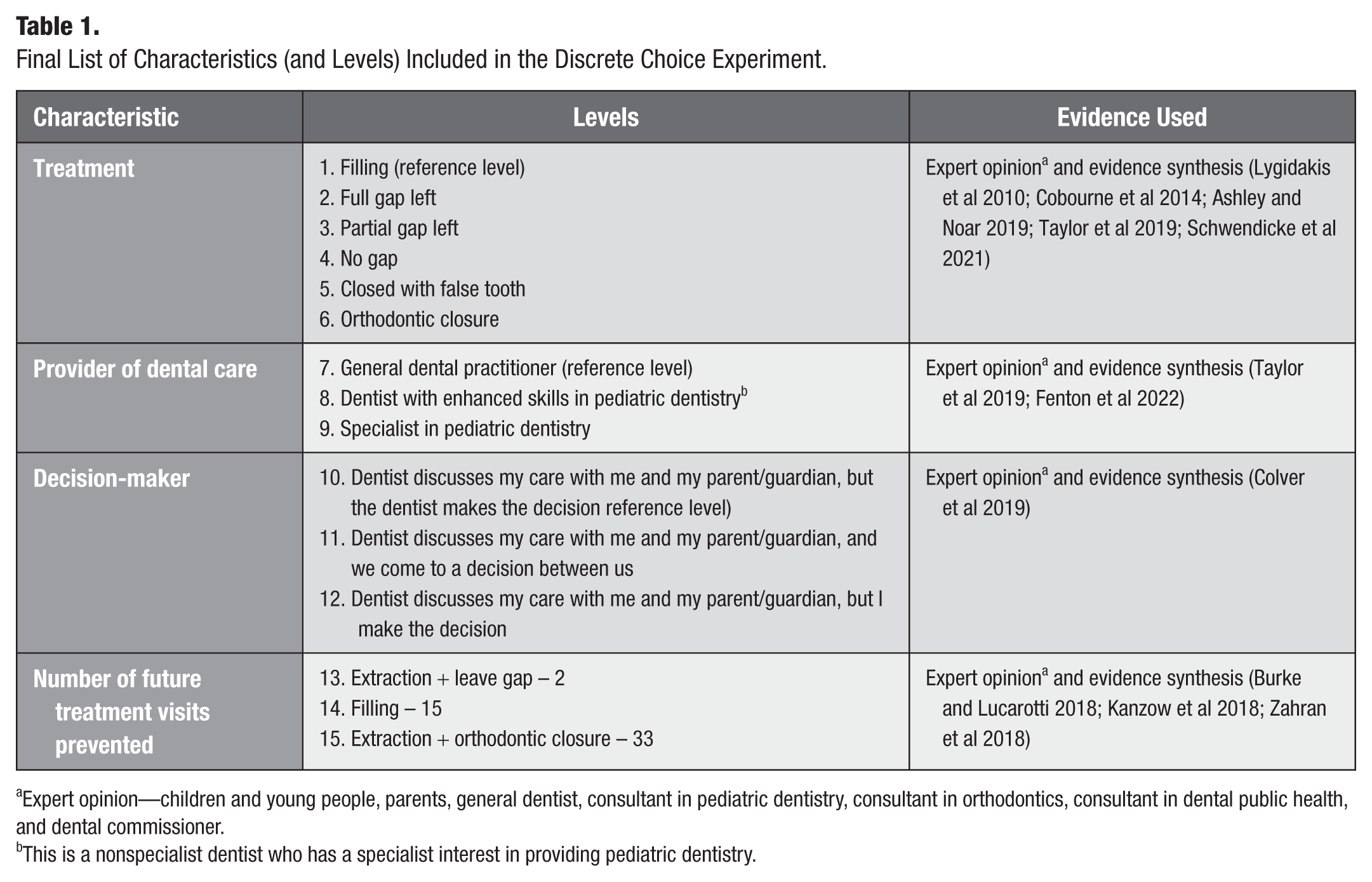
Expert opinion—children and young people, parents, general dentist, consultant in pediatric dentistry, consultant in orthodontics, consultant in dental public health, and dental commissioner.
This is a nonspecialist dentist who has a specialist interest in providing pediatric dentistry.
Experimental Design
The experiment included four characteristics. Three had three possible levels, and one had six possible levels. Together, these attributes could be combined in 162 unique profiles (6 × 3³). When these profiles were paired to form choice tasks, this resulted in 13,041 possible unique choice tasks in the full factorial design. Presenting all possible choice tasks to participants is not feasible; Ngene (ChoiceMetrics) created a dummy-coded D-optimal experimental design, selecting a subset of 18 choice tasks that efficiently represented the full set of possible combinations while maintaining statistical efficiency.
The design ensured that the number of choice tasks exceeded the number of dummy-coded parameters in the utility function (12 parameters) and was sufficient to ensure level balance across characteristics with three and six levels. Prior coefficient values were not readily available, so they were assumed to be zero. This meant there was no assumption about which characteristic was more likely to be valued, and the characteristics were considered equally important when designing the questions. Asking each respondent to answer 18 choice tasks would likely lead to survey fatigue and poor data quality. To mitigate against this, participants were randomized into one of two blocks of nine choice tasks. While the design in each individual block of choices is not orthogonal, the design as a whole is. Blocking may reduce level balance (Jaynes et al 2016). This was not the case in this DCE, as a good level of balance across the blocks was observed. Characteristic and level balance checks confirmed that each characteristic level appeared with the same frequency in choice tasks across each block. Each choice task included two different treatment scenarios and an opt-out alternative (described below).
Questionnaire Layout
The survey had two sections. Section 1 elicited participant demographic characteristics, dental anxiety (adapted from the Modified Child Dental Anxiety Scale [MCDAS]; Howard and Freeman 2007), and previous oral health experiences, including details related to first molars (with a clinical photograph to support).
Section two explained the problem, a 9-y-old child with a cFPM that was not painful but did cause occasional sensitivity. Participants were
told that a local anesthetic injection would be given to numb the mouth for all treatment options and to assume the level of discomfort would be equal across all treatment options,
introduced to the hypothetical choice tasks and given detailed information about each characteristic and level, and
advised that choosing to opt out of treatment would mean this tooth’s health would worsen and become painful and/or infected over time, potentially causing swelling or an abscess within 5 y. Furthermore, any future treatment would have less certain results.
Prior to completing the choice tasks, participants were given an example of a completed choice task and detailed preparatory information on what each characteristic and its levels meant. During the choice tasks, participants were able to refer to an age-appropriate help sheet (Appendix B), designed by members of the young person’s advisory panel. The final questionnaire was pretested using ‘think-aloud’ interviews with 15 children and young people, ensuring that the choice tasks were clear, that each characteristic and its levels were clearly described and understood as the research team intended. There were no amendments required after piloting.
Data Collection: Sample and Setting
Using the sample size calculation,
The DCE was a self-administered online survey for participants aged 12 to 16 y in the United Kingdom. Participants were recruited over ten weeks between September and November 2022 from
three primary care general dental practices and three emergency clinics in the northeast of England and
five UK specialist pediatric and orthodontic dental units (Newcastle, Leeds, Sheffield, Cardiff, and London).
Participants and their parents/guardians were given separate age-appropriate participant information leaflets prior to taking part. Consent/assent was included in the questionnaire, with confirmation required to continue completion of the survey. Participants were entered into a prize draw for their participation. Timers (minimum 45 seconds per page) were built in to prevent progression through the survey that would be too rapid to reasonably allow the presented material to be read. Data collection was conducted using Jisc Online Surveys software.
Data Analysis
Data were analyzed in Stata (2021) using a conditional (fixed-effects) logistic regression model, within a random utility framework, where the observable component of utility for each individual (i) in the choice task (j), (Vij), is described by a linear additive function, described in equation (1):

α is the alternative specific constant term, representing the additional utility of opting into treatment as opposed to not (choosing the opt-out), with all other characteristics held at their reference levels.
Data Quality
To assess the validity and rationality of responses, two additional choice tasks were added to each block (a consistency and dominance test). Following best practice, all participants’ responses to these validity tests were not included in the final estimation sample analysis; however, those who ‘failed’ these tests were not excluded from the sample (Johnson et al 2019). ‘Pass’ rates are reported to permit comparison to other studies (Tervonen et al 2018). Additional quality checks, including no straight-line responses (participant chooses the same option across multiple choice tasks, regardless of the characteristics or variations presented) and serial nonparticipation (participant consistently chooses the ‘no treatment’ opt-out alternative), were undertaken. A simple probit model was used to check if younger participants in the group were more likely to pass/fail the data quality checks.
Results
In total, 122 participants completed all choice tasks presented and were included in the analysis. There were no partial responses. Internal validity was good, with 82.8% (n = 101) and 86.1% (n = 105) passing the consistency and dominance tests, respectively. There was no evidence of straight-line responses or serial non-participation. The opt-out choice of ‘no treatment’ was chosen in 1.28% (n = 14/1,098) of all completed choice tasks. There was no evidence to suggest that younger children (β = 0.02; P = 0.145) were more likely to fail the validity tests.
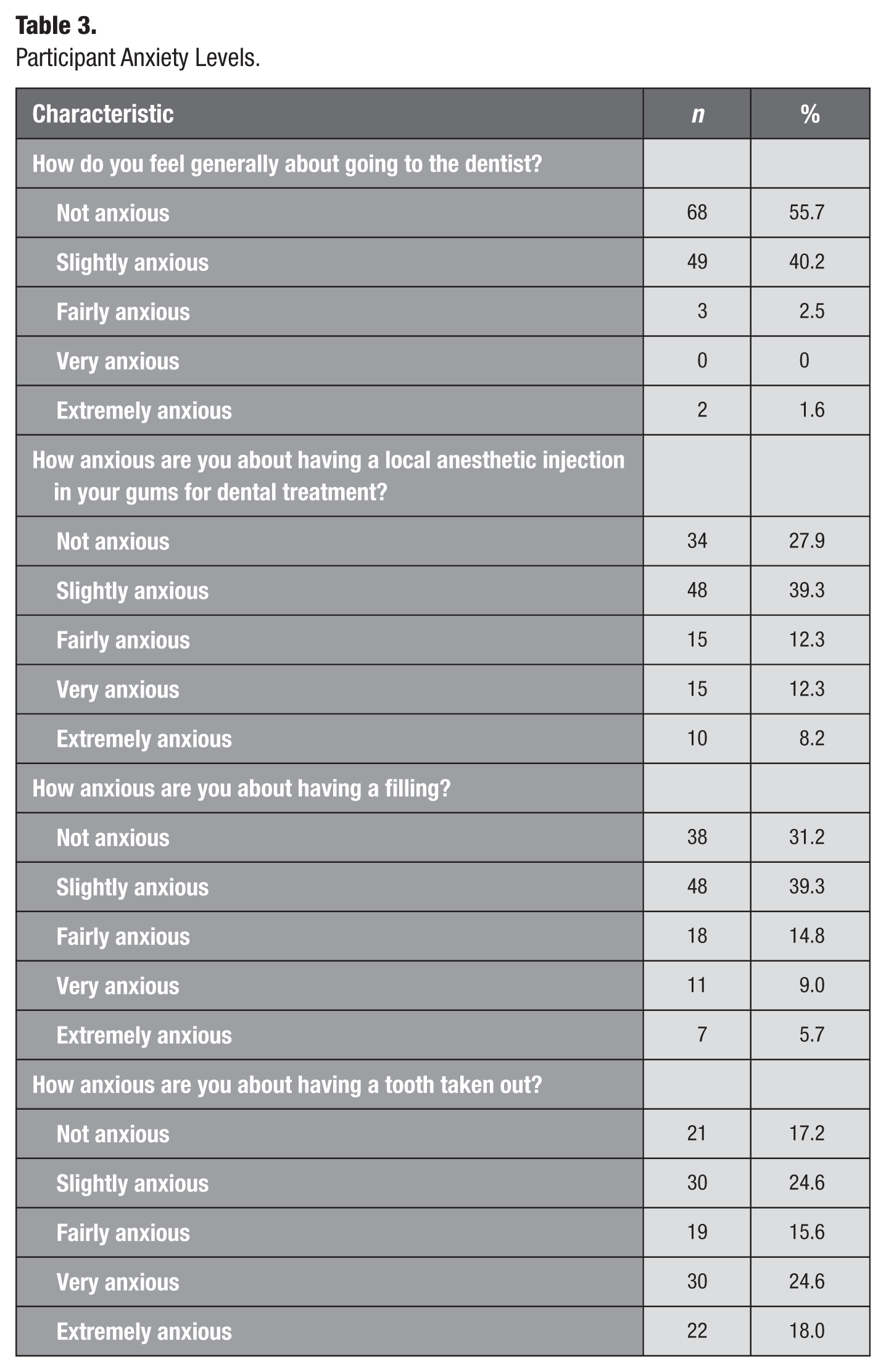
Participant demographics, oral health experiences, and dental anxiety are shown in Tables 2 and 3, respectively. The sample broadly represented the UK population, as gender and socioeconomic status (based on conversion of postcode to Index of Multiple Deprivation (IMD)) were comparable to recent UK census data (Office for National Statistics 2021). Participants appear to have similar levels of dental anxiety compared to the most recent UK Child Dental Health Survey (CDHS) (Tsakos et al 2015). In contrast, participants had greater experiences of fixed orthodontic treatment (59%) compared to the 9% of 12-y-olds and 18% of 15-y-olds in the UK CDHS (Rolland et al 2016). Most participants (78.7% [n = 96]) agree it was important to keep their first permanent adult molar teeth, while 17.2% (n = 21) were unequivocal in their opinion, with only 4.1% (n = 5) feeling it was not important to keep them. This is comparable to those reported in the UK adult general public DCE (Taylor et al 2025).
Participant Demographics and Oral Health Experiences (n = 122).
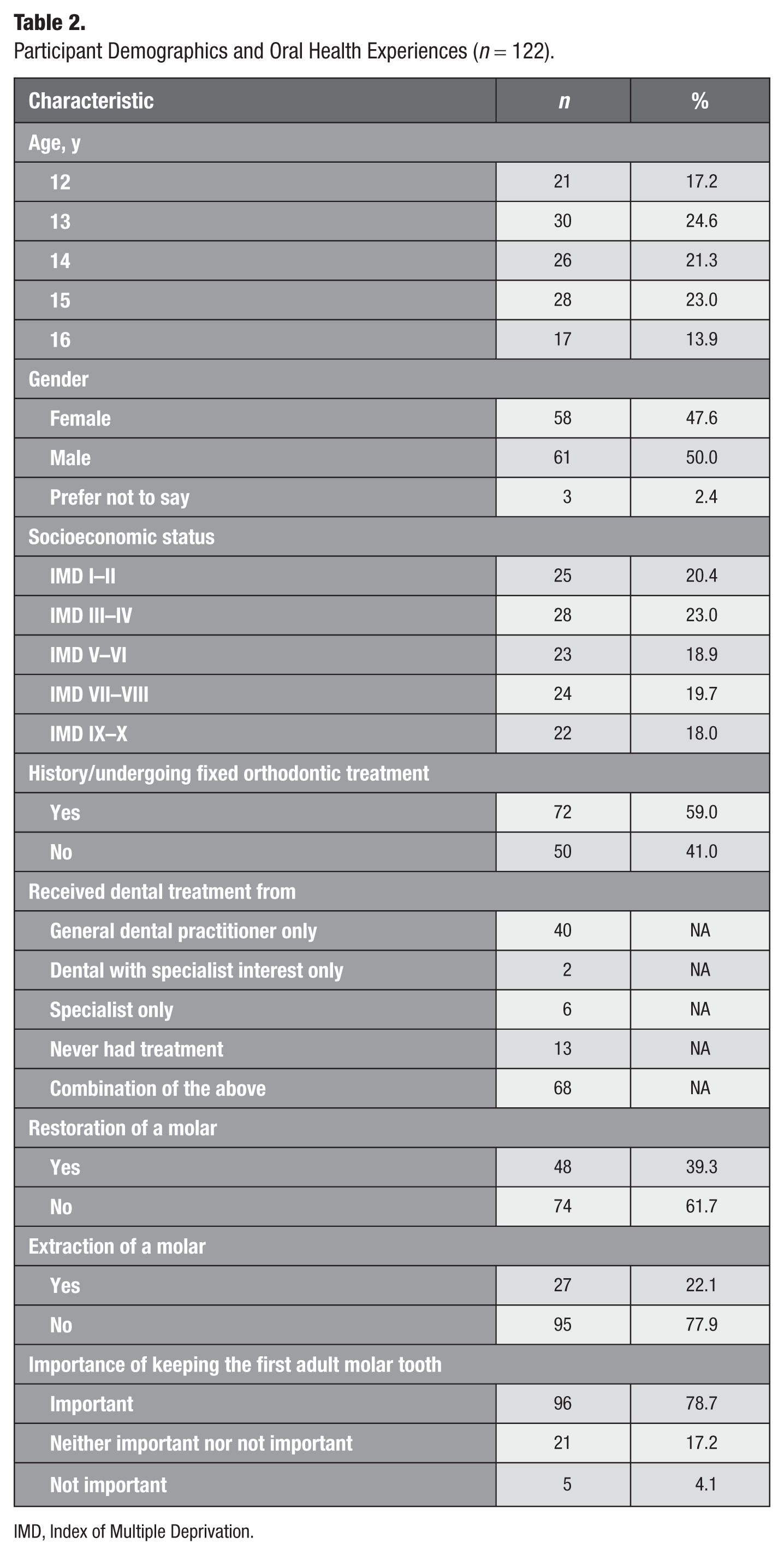
IMD, Index of Multiple Deprivation.
Participant Anxiety Levels.
The regression analyses are shown in Table 4. The alternative specific constant (ASC) has a positive odds ratio (OR) of 135.14 (95% confidence interval [CI], 66.02–276.63; P < 0.001), indicating that young people strongly prefer that the cFPM be managed, compared to not being managed. Preferences ranged from no preference to a preference for spontaneous closure, compared with a restoration (OR = 1.40; 95% CI, 0.98–1.99; P = 0.063). Having the cFPM restored was preferred to extractions with treatments to close the gap (orthodontics; OR = 0.61; 95% CI, 0.46–0.81; P = 0.001), having prosthetic replacement with a bridge (i.e., described in the survey as closed with a false tooth) (OR = 0.37; 95% CI, 0.24–0.45; P = 0.001), or being left with a partial gap (OR = 0.31; 95% CI, 0.22–0.43; P = 0.001) or a full gap (OR = 0.11; 95% CI, 0.08–0.17; P = 0.001).
Regression Analyses.
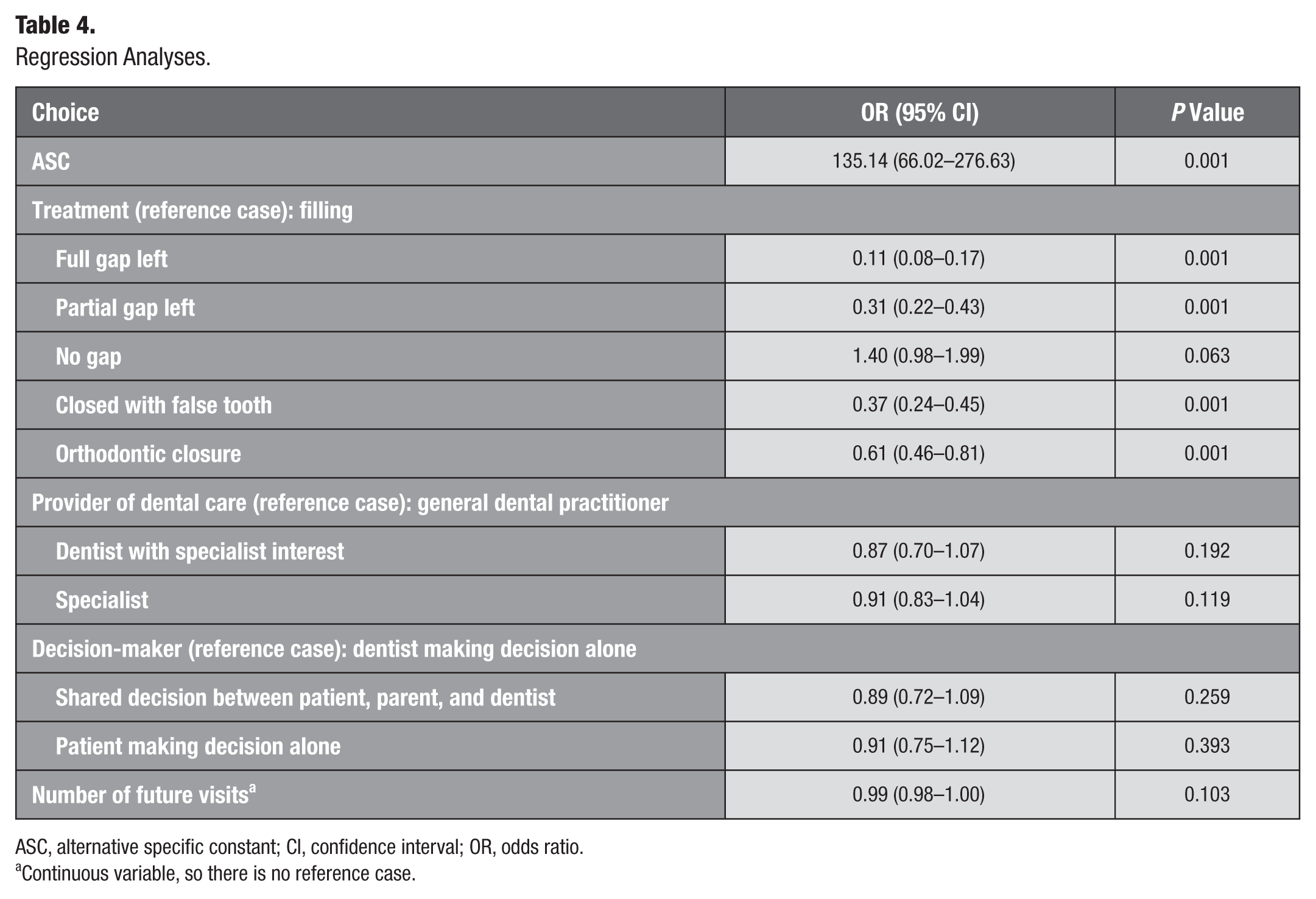
ASC, alternative specific constant; CI, confidence interval; OR, odds ratio.
Continuous variable, so there is no reference case.
Regarding all other attributes, there was variation in the preferences of young people. In terms of who was to provide the treatment, preferences spanned from no preference to a preference for having care provided by a general dentist rather than a dentist with specialist interest (OR = 0.87; 95% CI, 0.70–1.07; P = 0.192) or a specialist in pediatric dentistry (OR = 0.91; 95% CI, 0.83–1.04; P = 0.119). Compared to the dentist making the decision alone, there was no clear direction of preference about whether this decision should be solely made by their parents (OR = 0.91; 95% CI, 0.75–1.12; P = 0.393) or made as part of a shared decision with the patient, their parent, and the dentist (OR = 0.89; 95% CI, 0.72–1.09; P = 0.259). Very little variation in preferences existed to avoiding future visits (OR = 0.99; 95% CI, 0.98–1.00; P = 0.103). Despite variations, no statistically significant differences were observed to demonstrate a unidirectional preference.
Discussion
This DCE shows that young people are able and want to make decisions about their health care, demonstrating the importance of directly involving and recognising young people’s preferences. To the best of our knowledge, this is the first study to use a DCE to elicit young people’s preferences for managing cFPMs.
Young people prefer that cFPMs are managed compared to not, accepting that no treatment would lead to the tooth’s health worsening over time. The avoidance of a space is valued equally, whether this is by a cFPM being restored or extracted, with the space being closed spontaneously by mesial migration of the second permanent molar. The positive odds ratio estimate (OR = 1.40; 95% CI, 0.98–1.99) suggests the sample preferred to remove the cFPM, allowing the space to close naturally; however, the confidence interval width implies a wide variation in preferences. Despite guidance advising ideal extraction timing (Noar et al 2023), it is accepted that, in reality, complete closure cannot be guaranteed (Lygidakis et al 2022).
In comparison, restoration is clearly preferred to leaving a full or partial gap. This aligns with the views of a concurrently run UK adult general public DCE sample (Taylor et al 2025). It is possible that poor aesthetics associated with having a partial or full gap in the dentition may have driven preferences, as indicated in a recent qualitative study with children on managing cFPMs (Taylor et al 2025). Young people’s persistent social media exposure to highly idealized images of a ‘perfect’ dental appearance may provide an explanation (Rana and Kelleher 2018). Alternatively, young people might perceive having a gap as a functional impairment, reducing their oral health–related quality of life; however, evidence, albeit from adults, would suggest this is only the case for anterior teeth (Tan et al 2016). Future mixed-methods studies could explore this in more detail. Similarly, the DCE found that restoring cFPMs was clearly preferred to orthodontic closure with fixed metal appliances. UK adults showed no preference for restoration over orthodontic closure for cFPMs (Taylor et al 2025), with qualitative exploration suggesting that they perceived fixed metal appliances to close the space following removal of a cFPM as socially acceptable (Taylor et al 2025). However, young people do not necessarily conform to this, indicating a preference for clear aligners (which are less visible) over fixed metal appliances (Alansari 2020).
It is expected that prior experiences would influence heuristics, as demonstrated in a concurrent public DCE (Taylor et al 2025). Previous oral health experience data, such as restoration and extraction of the first adult molar teeth, were collected. However, the subgroup samples were too small to draw meaningful conclusions. Ascertaining preference heterogeneity for subgroups of interest will likely be the basis of future research.
Young people expressed no clear preference for which dental professional provided the treatment for cFPMs. Prior experiences of participants, knowledge of the differences, and expectations regarding longer-term trusted relationships might explain the lack of evidence of a preference (Davison et al 2021; Taylor et al 2025). Evaluating which type of professional yields better clinical outcomes, and at what cost to the public health care system, is important for supporting workforce planning and ensuring more efficient use of staff mix across clinical teams. This could increase timely access to more “specialized services” closer to home by dentists with specialist interests, reducing hospital referrals and enabling earlier treatments, thereby reducing potential complications (NHS England 2015).
Participants expressed a desire to be involved in the decision-making for cFPMs. Compared to dentistry’s historically paternalistic model of decision-making, young people clearly want their opinions heard, rather than being told what to do. Several studies corroborate this (Barber et al 2018; Colver et al 2019; Taylor et al 2025), with UK national guidance emphasising that children and young people have agency and should be involved as active participants in a shared decision-making approach for their care (NICE 2021). Including young people’s opinions can be challenging, as competence and capacity vary between children and can fluctuate over time in the same child (Coyne et al 2014; Taylor et al 2025). Health care professionals and parents must facilitate this iterative process and embed it as standard of care, although the extent to which health care professionals (Osborne et al 2024) and parents (Taylor et al 2025) currently do so remains low. Improving engagement requires educators, particularly those responsible for undergraduate curricula, to ensure shared decision-making for children and young people is core to their teaching relating to the informed consent process and their practice in clinics with students.
There was no evidence that young people preferred a package of care that avoided additional future treatment visits. This finding is consistent with the UK general public (Taylor et al 2025), suggesting that both cohorts are strongly influenced by immediately realised outcomes (i.e., the gap being closed or not). Individuals make choices by balancing the risks and benefits of action (Ferrer and Klein 2015), with events occurring in the present valued more highly than those occurring in the future. It appears in the context of a cFPM in a 9-years-old that future risks and benefits are not valued equally to those faced in the present; however, the impacts associated with certain decisions might only become apparent in the future (e.g., entering the restorative cycle earlier if a filling is chosen). Including future risks and benefits when deciding how to manage cFPMs could influence decisions made in the present. Alternatively, there may be a genuine disinterest in avoiding future appointments among young people, or they may lack the lived experience to conceptualise, for example, 33 future treatment visits.
It appears that concerns about cognitive burden and complexity associated with not using DCEs with young people (Colver et al 2019; Rowen et al 2020; Michaels-Igbokwe et al 2021; Rogers et al 2021) were unfounded in this study. Social desirability bias and primacy, recency, and ordering effects were not observed, suggesting young people understood the choice tasks and engaged in trading. It appears DCEs are acceptable to adolescents, with the ability to perform the DCE choice task appearing to be related to respondents’ ability to understand the concept of trading off attributes rather than the age of the respondent, a concept reported elsewhere (Colver et al 2019). These data quality assessments are of methodological importance, as they alleviate previously reported concerns raised in this patient cohort and confirm that DCEs can be used to elicit young people’s preferences for oral health care interventions. This can support future DCE designs and researchers’ use of preference elicitation tasks if it is the most suitable method for answering the research question, considering participants’ ages in a way similar to other aspects of development, rather than simply their age.
Strengths of this study included combining qualitative interviews, expert opinion, and a literature review to develop characteristics and their levels. Including ‘decision-making’ as an attribute was novel, as only one other dental study has used this (Taylor et al 2025). Validity checking and piloting the DCE gave further clarity and context. Apart from the cost characteristic being omitted from this DCE, the remaining characteristics and their levels were exactly the same as the recently published UK adult DCE (Taylor et al 2025). This permitted a narrative comparison of summary results from both, highlighting similarities and differences in preferences between adults and young people for the same clinical scenairo.
The age range (median 13; range, 12–16) of the included participants may limit generalisability as key decisions for management of cFPMs are often taken around the age of nine, so it may have been beneficial to elicit preferences from a younger cohort; however, parental proxies become unavoidable when children are too young to comprehend or complete DCE tasks (Rowen et al 2020). Ethnicity was not recorded, which means certain population groups may have been underrepresented. These data would have helped identify any systematic differences in preferences between ethnic groups (e.g., regarding the extent of acceptability of extraction and the presence of a full or partial gap in the dentition). Another limitation is how the management characteristic is presented in the choice task. Participants are informed that the outcomes are guaranteed; in reality, that is not always the case. Similarly, management characteristics may not fully reflect procedural challenges. Procedural discomfort, treatment time, risk of imperfect outcome, and postoperative sequelae were considered in the DCE design but were felt to be less of a priority. Finally, the hypothetical scenario suggested that the 9-year-old patient with the cFPM had only mild sensitivity. Patients with cFPMs often present with symptoms beyond mild sensitivity (e.g., pulpitis). However, setting up a DCE with a cFPM that was causing pain would preclude the relevant option of restoration, as existing evidence strongly supports that symptomatic teeth would almost certainly be removed (Taylor et al 2019; Lygidakis et al 2022; Taylor et al 2025). Finally, a discrepancy was noted in how the choice task was set up. The online DCE asked the participant to think about a 9-year-old child, while Appendix B (support documentation) asks the participants to imagine they have a damaged tooth. While this might subtly affect the internal validity of the study, it is unlikely to influence the results or external validity, as Appendix B was only there to provide information should the participants forget, and there is no way of measuring how many children used it.
Conclusion
Young people clearly expressed preferences on how compromised first permanent molars should be managed. They had no clear preference regarding whether a cFPM was restored or extracted, provided the resulting space spontaneously closed completely. They expressed a preference to be included in a shared decision-making process for these teeth, rather than having their preferences assumed solely by parental proxies. Young people were able to understand and complete this DCE.
Author Contributions
G.D. Taylor, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; D. Boyers, N. Innes, L. Vale, C.R. Vernazza, contributed to conception and design, data analysis and interpretation, drafted and critically revised the manuscript; C. Exley, contributed to conception, data analysis and interpretation, drafted and critically revised the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844261452554 – Supplemental material for Young People’s Valuations of Managing Compromised Molars: A Discrete Choice Experiment
Supplemental material, sj-docx-1-jct-10.1177_23800844261452554 for Young People’s Valuations of Managing Compromised Molars: A Discrete Choice Experiment by G.D. Taylor, D. Boyers, C. Exley, N. Innes, L. Vale and C.R. Vernazza in JDR Clinical & Translational Research
Footnotes
Acknowledgements
We thank the participants for taking the time to complete the DCE and the recruiting centers for supporting the project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: G.D. Taylor was funded by an NIHR Doctoral Research Fellowship (NIHR300251) during this research study. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Data Availability
Data supporting this study are included within the article and/or its supporting materials. Transcripts are held with Newcastle University Repository and are available from the corresponding author upon request.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.