
Abstract
Purpose
LGBTQ + individuals experience significant health disparities, driven in part by a lack of provider knowledge, necessitating effective interventions for medical trainees. This study examined the impact of a 1-h educational intervention for first-year medical students on 6 self-reported competency domains in LGBTQ + health and compared the magnitude of score changes for competencies specifically targeted by the lecture to those that were not.
Methods
This was a quasi-experimental study. Surveys were distributed before and after a 1-h lecture delivered by an LGBTQ+-identifying senior medical student. Respondents reported data on LGBTQ + identification and prior experience with LGBTQ + health-related topics, and they rated their ability to perform each of 6 LGBTQ + health competencies. Two faculty members with LGBTQ + health expertise blindly reviewed the material and identified which competencies were addressed.
Results
Our sample consisted of 38 matched survey response pairs. Students reported significant increases across all 6 competencies, with no significant difference in score changes between competencies that were targeted by the lecture and those that were not. Prior training in LGBTQ + health-related topics did not significantly affect competency scores. LGBTQ + identity was associated with greater score increases for targeted, but not non-targeted, competencies.
Conclusion
This study demonstrates that a 1-h, LGBTQ+-identifying student-delivered lecture can significantly increase students’ self-reported comfort with LGBTQ + patient care, regardless of LGBTQ + status or prior training. Scores improved for all competencies, regardless of whether they were targeted by the lecture. Further study is indicated to measure whether increases in competency scores are maintained throughout medical training.
Keywords
Introduction
Lesbian, gay, bisexual, transgender, queer, and other non-heterosexual, non-cisgender (LGBTQ+) individuals comprise 4.5% of the US population, with recent polls suggesting consistent increases among younger generations.1,2 This underrepresented group has been shown to experience significant health disparities—preventable differences in the burden of disease related to unequal allocation of resources—compared to their cisgender and heterosexual counterparts across multiple physical and mental health conditions.3–9 LGBTQ + individuals also have decreased access to and utilization of preventive health care services.10–12
The etiology of these disparities is multifactorial. Discrimination by healthcare workers (HCWs), operationalized as systemic actions that treat individuals unfairly based on characteristics such as one's gender or sexuality, creates barriers that limit LGBTQ + individuals’ engagement with healthcare. 13 Almost 56% of sexual minority and 70% of gender minority adults, whose attractions, behaviors, and expressions do not align with cisheteronormative societal expectations, report discrimination from HCWs in the past year. Further, 28% and 40% of transgender adults, whose gender identity differs from the sex they were assigned at birth, report delaying or avoiding necessary medical care and preventive care, respectively, in the past year due to discrimination.14–16 The minority stress model links such stigma-related stressors to adverse health outcomes for LGBTQ + individuals.17–19
The most recent Institute of Medicine identified lack of provider knowledge as a key contributor to LGBTQ + health disparities. 20 In one survey of primary care providers, 70.1% felt insufficiently informed about LGBTQ + patient health needs, and 74.8% about their clinical management. 21 These gaps extend into medical education 22 : medical students report lower confidence caring for sexual minority patients, 23 and in a multispecialty residency study, only 12% of residents felt adequately trained to care for transgender patients. 24
Educational interventions present a critical opportunity to address 2 key drivers of LGBTQ + health disparities: stigma faced by LGBTQ + individuals and lack of knowledge about their care among HCWs. Lower LGBTQ + health knowledge has been associated with more negative attitudes among nursing and medical students, 25 whereas LGBTQ + medical students report greater comfort caring for LGBTQ + patients compared to their heterosexual and cisgender peers. 26 As more medical students identify as LGBTQ + in line with population-level trends, 2 peer-led educational interventions may be particularly engaging and effective. Together, these findings suggest that increasing students’ knowledge of LGBTQ + individuals’ lived experiences could improve patient care and reduce stigma within healthcare settings.
Data on effective methods for incorporating LGBTQ + health into undergraduate medical education (UME) remain limited. Reviews have demonstrated the efficacy of multiple techniques, including faculty-led didactics, community participatory panels, and small-group case-based vignettes, in which students apply knowledge to clinical scenarios to enhance problem-solving.27,28 However, most published studies are faculty-led and multi-session, with little evidence supporting brief, student-led formats. 27 Given increasing curricular constraints as medical knowledge expands and preclinical time contracts, efficient educational models are needed. 26 Moreover, given the central role of identity in LGBTQ + issues and because many working HCWs report little comfort with or training on LGBTQ + health, engaging students as teachers of LGBTQ + content may help address these gaps. Research on student-led interventions, where educational sessions are facilitated by peers rather than faculty, is sparse: existing examples include a 2-h first-year session with a patient panel and small-group discussion and a student-designed intervention ultimately led by faculty.29,30 Our approach sought to extend this limited literature by testing a brief, student-led, and LGBTQ+-led intervention for medical students and its effect on LGBTQ+-health-related competencies.
With this context, we designed a 1-h lecture for first-year medical students, delivered by an LGBTQ + identifying senior student. Two independent, blinded medical education experts reviewed the session to determine which of 6 core LGBTQ + health competencies—observable abilities that learners are expected to demonstrate—were addressed. A pre–post survey assessed whether the intervention improved confidence across all competencies or only those targeted by the lecture. This study design allowed us to uniquely assess (1) the magnitude of impact of a LGBTQ+-identifying student-delivered 1-h lecture, (2) whether competencies increased globally or were specific to the content targeted, and (3) whether LGBTQ + students or those with prior training in LGBTQ + health topics exhibited a different pattern of competency changes.
Materials and Methods
Refer to Table S1 (Supplemental File 1) for definitions of terminology in this manuscript. This is a quasi-experimental study design using surveys to measure the impact of an educational intervention.
Study Design, Setting, and Participants
This study consisted of pre-intervention and post-intervention surveys distributed to first-year medical students before and after a foundational lecture on LGBTQ + health and was conducted in March 2024 at the study site's School of Medicine. The reporting of this study conforms to the CONsolidated Standards Of Reporting Trials (CONSORT) statement 31 (Supplemental File 2). This study was granted exemption from the study site's Institutional Review Board (IRB, #230933); thus, completion of surveys constituted implied consent to the research study. It was made clear to all students before study initiation that participation was anonymous, voluntary, and uncoupled from graded assessments and course evaluation. Inclusion criteria for the study were current first-year students actively enrolled in the MD Program at the study site's School of Medicine, and exclusion criteria were anyone other than those groups as listed above; accordingly, a convenience sampling strategy was employed. All eligible participants (ie, first-year medical students; N = 96) were provided on site with an Information Sheet that described the purpose, procedures, risks, benefits, and confidentiality protections of the study. Surveys were made available via email and QR codes before and after the lecture to all students in the first-year medical school class. Pre-intervention and post-intervention survey responses were matched via non-identifiable participant-selected codes. Responses were collected in March 2024, and all data were collected and stored in REDCap. 32
Study Main Outcomes and Survey Tools
The main outcomes of our study were students’ self-reported confidence in each of 6 core “Competencies in LGBTQ + Health for Undergraduate Medical Education,” which we assessed via pre-intervention and post-intervention surveys administered before and after the educational intervention, respectively. Specifically, a 9-item pre-intervention survey (see Figure S1, Supplement) and a 13-item post-intervention survey (see Figure S2, Supplement) were provided to all first-year medical students. The survey items were locally developed for this study and have not undergone prior psychometric validation or been used in previously published research. Survey items were informed by national and institutional guidelines related to LGBTQ + health education and were developed in collaboration with content experts in medical education and LGBTQ + health. Prior to implementation, the questionnaires underwent informal pilot review by medical students and faculty to assess clarity, relevance, and face validity. Demographic data were collected on LGBTQ + identification and prior experience with LGBTQ + health-related topics. Six core “Competencies of LGBTQ + Health for Undergraduate Medical Education” were crafted in collaboration with faculty and students using guidelines from both the Association of American Medical Colleges (AAMC) and Tufts University's Biomedical Queer Alliance.33,34 These finalized competencies included (1) collecting a sexual history, (2) performing a physical exam, (3) using appropriate terminology, (4) choosing health maintenance and screening tests, (5) providing appropriate counseling, and (6) understanding LGBTQ + specific health disparities and biases (see Figure 1).
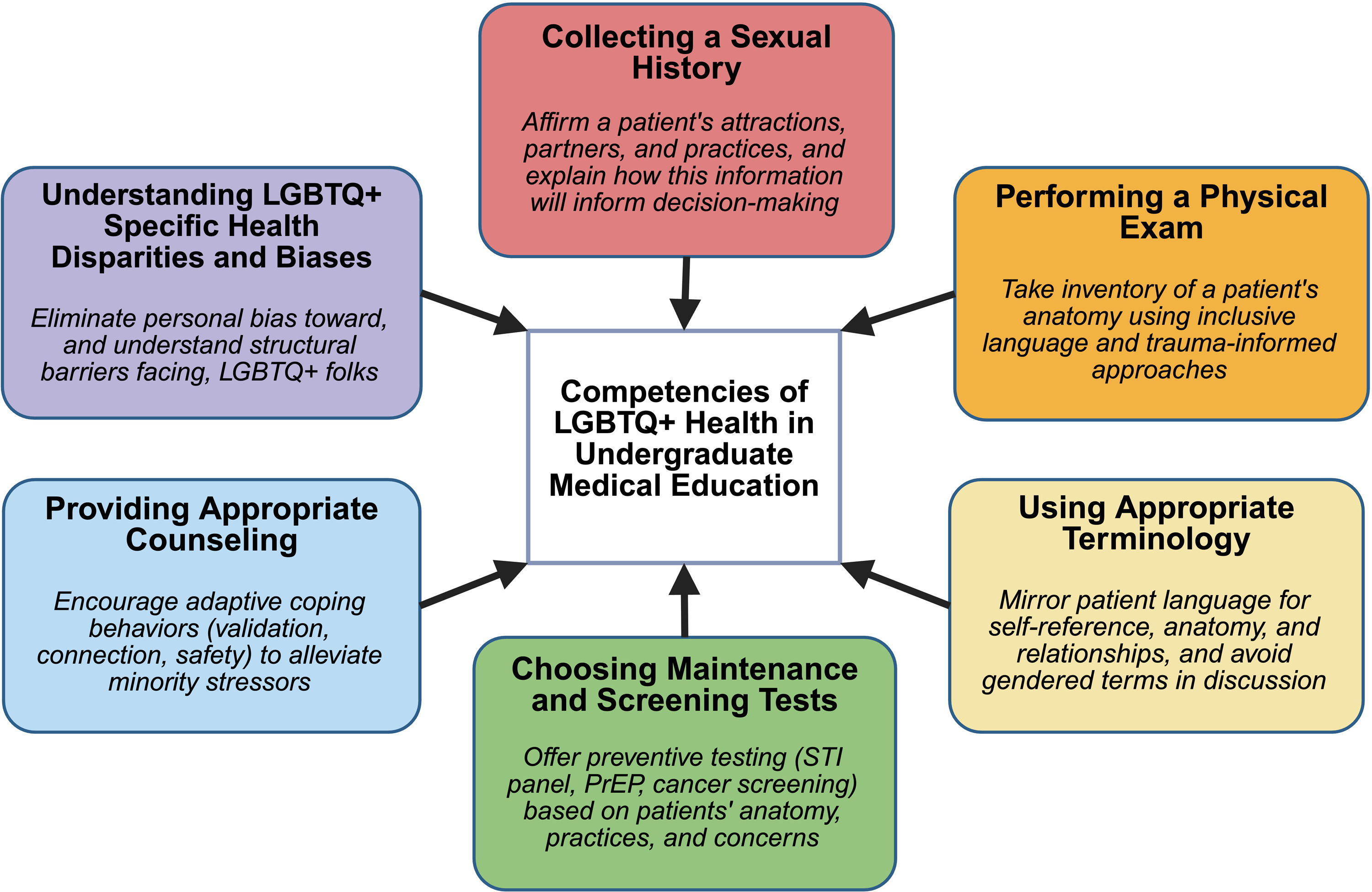
Six competencies of LGBTQ+ health for undergraduate medical education were defined to capture medical students’ comfort with, and knowledge of, interacting with LGBTQ+ patients. A short description or example of each competency is shown, and all competencies are conceptualized to demonstrably contribute to a medical student's overall comfort with and knowledge about caring for LGBTQ+ patients.
These competencies were chosen to cover a range of abilities important for medical training, including foundational medical knowledge, familiarity with sociocultural determinants of health, and comfort with patient care interactions. In the pre-intervention and post-intervention surveys, respondents were asked about their agreement to statements regarding comfort in performing each of the 6 competencies with an LGBTQ + patient on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). In the post-intervention survey, students were additionally asked which of the competencies, if any, they felt the lecture helped them develop. Therefore, for each of the 6 competencies, each participant rated their confidence from 1 to 5 before and after the intervention. These scores were averaged to produce means and standard deviations that are reported in Table 1.
Modeling Results for Changes in Scores Across Each of 6 Core Competencies in LGBTQ + Health.

Mean pre-intervention and post-intervention survey scores across all matched participant responses (N = 38) for each competency of LGBTQ + health in undergraduate medical education (scores range from 1 to 5). Change scores represent the mean change in competency scores from pre-intervention to post-intervention. Paired t-tests were used to determine whether post-intervention changes were statistically significant for each competency. Scores are shown as mean ± standard deviations; change scores include 95% confidence intervals (CI).
Abbreviation: UME, undergraduate medical education.
Educational Intervention
A 1-h lecture on foundational concepts in LGBTQ + health was delivered within the 13-month preclinical curricular phase, during a block covering reproductive and endocrine organ-based pathophysiology. Specifically, the lecture PowerPoint slides were made available for all students to download and reference afterwards to study. The 45-min didactic lecture covered several faculty-approved learning objectives that (1) highlighted legislation affecting LGBTQ + health care, (2) described health disparities faced by LGBTQ + patients, (3) advocated for inclusive language when talking to gender-minority patients, and (4) defined gender-related medical misattribution and invasive questioning and its negative consequences for the health of LGBTQ + patients. The final 15 min allowed students to discuss cases related to the learning objectives with each other and to ask the lecturer questions. Attendance at this lecture, as with all other preclinical didactic lectures, was not strictly required (ie, attendance was not taken); however, content from the lecture was assessed on weekly and end-of-block examinations about which students were informed beforehand. The intervention was led by an upper-year student who openly identified as LGBTQ+, making it uniquely student-led within the preclinical curriculum, and included educational content that was shaped collaboratively by students and clinicians with expertise in LGBTQ + health. No other lecture in the preclinical curriculum is delivered entirely by a student. Preceding this educational intervention within the preclinical curriculum, first-year students had only been exposed to a few instances of devoted LGBTQ + health topics, including a case-based learning vignette and faculty-led lecture, totaling 3 h.
To determine which of the 6 competencies of LGBTQ + health for UME were most directly targeted in the lecture and assess the specificity of improvements in LGBTQ + health as a result of the intervention, 2 faculty members with subject matter expertise who were uninvolved in the design of the lecture independently reviewed the lecture material and categorized which of the 6 competencies designated above were addressed. These blinded faculty reviewers identified 2 targeted competencies: “using appropriate terminology” and “understanding LGBTQ+-specific health disparities and biases.”
Statistical Methods
All statistical analyses were performed in RStudio (Version 2023.9.1.494). 35 Descriptive statistics were used to characterize the sample of respondents and determine group mean scores across survey items. Paired t-tests were used to compare pre-intervention and post-intervention survey data. To test whether self-reported competencies changed as a result of the educational intervention, we constructed linear mixed-effects models to predict competency score changes as a result of the educational intervention, including LGBTQ + identity, prior training in LGBTQ + health-related topics, and time (pre-intervention or post-intervention) as fixed effects and participant as a random effect.36–38 We also separately fit models to investigate potential differences in pre-intervention and post-intervention scores for competencies that were targeted versus non-targeted in the intervention. Detailed explanations of rationale, assumptions, and model specification for these analyses can be found in Supplemental Methods: Statistical Analysis (Supplement).
We also tested the internal consistency of the competency scales using Cronbach's alpha. The 6 overall competencies demonstrated acceptable to good reliability at both pre-intervention (α = 0.78) and post-intervention (α = 0.73). More specifically, the 4 non-targeted competencies demonstrated stable internal consistency (α = 0.72 at both time points), while the 2 targeted competencies demonstrated lower internal consistency pre-intervention (α = 0.50) and acceptable internal consistency post-intervention (α = 0.71). Given the small number of items for these targeted competencies (n = 2), α values should be interpreted cautiously.
Results
Study Demographics
Fifty-one (53% of the first-year class) completed the pre-intervention survey, and 41 (43%) completed the post-intervention survey. Thirteen records across pre-intervention and post-intervention surveys could not be matched due to omitted information in the identifier code section or due to completion of one but not both surveys, resulting in 38 matched surveys, which were used in subsequent analyses. Of the students whose surveys were matched, 23 (61%) reported prior exposure to or training in LGBTQ + health outside of medical school, and 13 students (34%) identified as LGBTQ+.
Pre-Intervention Self-Reported Competencies in LGBTQ + Health
Mean pre-intervention and post-intervention scores for each competency in LGBTQ + health for UME, and the average changes in each competency from pre-intervention to post-intervention are quantified in Table 1 and visualized in Figure 2. Self-reported competency scores at baseline were not significantly different in those participants who identified as LGBTQ + or in those who reported prior training in LGBTQ + health-related topics.
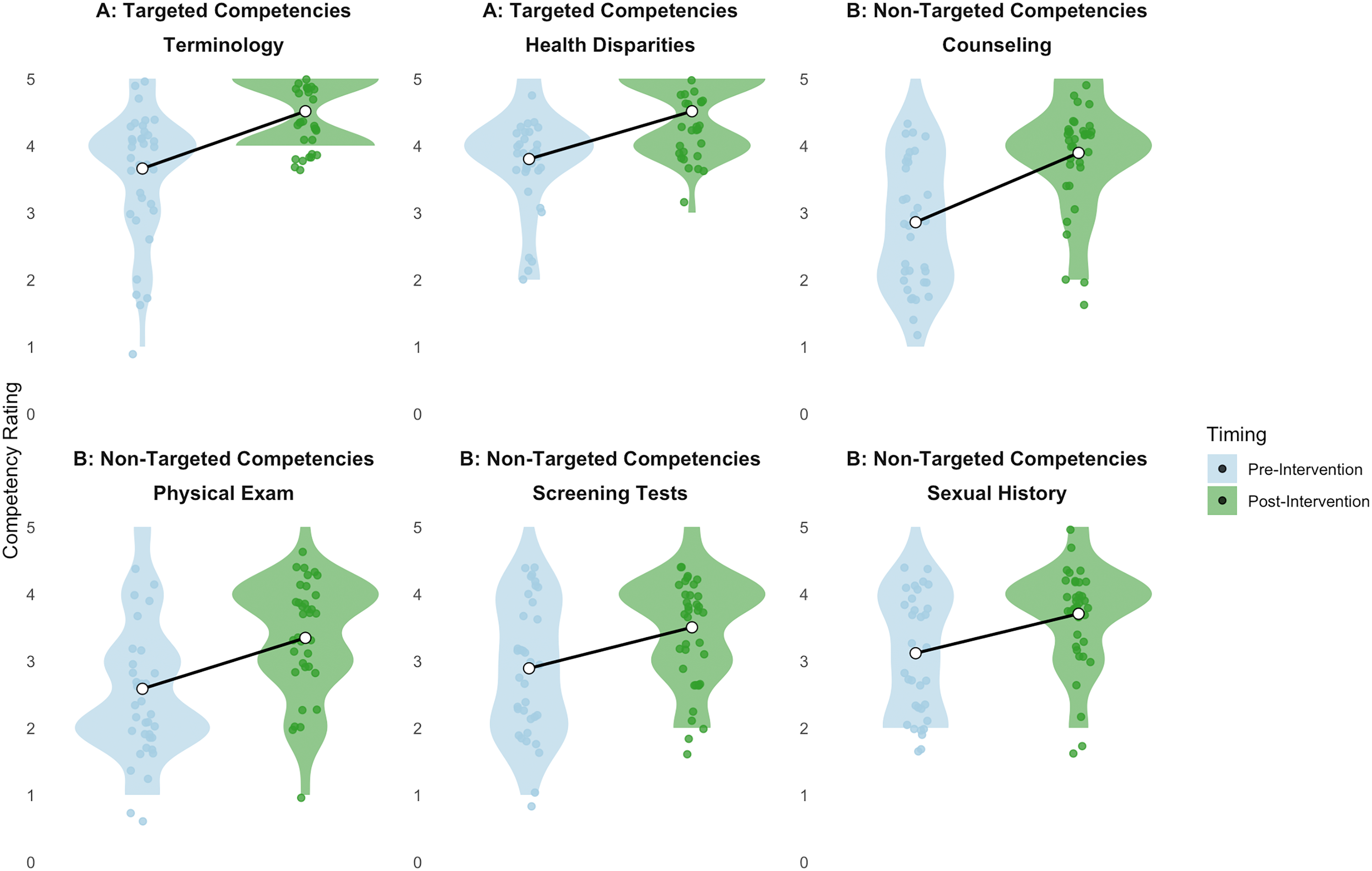
All self-reported competencies significantly increased following the educational intervention, with competencies that were targeted in the training (“using appropriate terminology” and “understanding LGBTQ+-specific health disparities and biases” (A)) yielding the highest post-intervention competency scores compared to competencies that were not explicitly targeted (B). Significant improvements in self-reported competencies were observed across all competencies (all P < .05) after the educational intervention.
Effects of Educational Intervention on Changes Across all Competencies in LGBTQ + Health
Full results from our mixed-effects modeling can be found in Table 2. The educational intervention broadly improved self-reported competencies in LGBTQ + health (all P ≤ .001). Mean scores for each competency increased an average of 0.71 points from pre-intervention to post-intervention, with “using appropriate terminology” (+0.87 points) and “providing appropriate counseling” (+0.95 points) showed the greatest increases in self-reported competence, though changes in scores in competencies that were targeted by the lecture were not significantly larger than changes in non-targeted competency scores. Participants who completed the post-intervention survey reported being “very satisfied” with the overall lecture content (mean satisfaction was 79.0 ± 14.3 out of 100).
Linear Modeling Results of Changes in Each of 6 Core Competencies in LGBTQ + Health as a Result of Educational Intervention.

Results of linear mixed-effects models testing changes in self-reported competencies in LGBTQ + health due to student-led educational intervention, with fixed effects of LGBTQ + identity and prior training in LGBTQ + health-related topics, and a random effect of participant. Pre-intervention competency scores are reported as mean ± standard deviations. Results in
Differential Effects of Educational Intervention on Changes in Targeted Competencies in LGBTQ + Health
To test the hypothesis that targeted educational content would preferentially increase self-reported competencies in LGBTQ + health in these areas, we grouped competencies according to whether they were specifically addressed in the educational intervention. Our modeling results demonstrated significant improvements in targeted and non-targeted competencies after the educational intervention (both P < .001). We also found evidence that LGBTQ + identity had a significant effect on improving targeted competencies (P = .003), which was not seen in the non-targeted competencies (P = .60); this interaction was statistically significant (LGBTQ + identity-by-Competency Group interaction: P = .011).
We evaluated whether students could identify which competencies were targeted in the lecture. Nearly all students (95% [36/38]) reported that the intervention helped them improve in the 2 targeted competencies. This agreement was specific to the targeted areas; no other competency had more than 50% of students stating the lecture “help[ed] to develop” it.
Discussion
Our student-led lecture on LGBTQ + health topics offers evidence that even a brief intervention can significantly increase medical students’ self-reported comfort with LGBTQ + patient care, regardless of LGBTQ + identity status or prior experience.
The AAMC does not currently mandate LGBTQ + health education in UME, despite increasing recognition of LGBTQ + health disparities.39,40 Medical schools have expanded LGBTQ + content and educational interventions improve student competency and attitudes, yet formalized national competencies remain uncommon.41–47 Persistent curricular time constraints, especially in increasingly compressed preclinical programs, pose a major barrier to broader adoption. 26
Here, we sought to determine if students’ competencies in LGBTQ + health could be improved after a brief educational intervention. Similar initiatives to our intervention are reported in the medical education literature.41–44,47 However, our intervention is unique in 3 critical ways. Firstly, it is efficient, requiring only 1 h of curricular time. While research suggests medical students should have at least a total of 35 h of LGBTQ + patient contact and 35 h of LGBTQ + education to achieve LGBTQ + cultural competency, 48 this goal is increasingly challenging to meet. 49 Our intervention offers a pragmatic means of providing preclinical students with effective LGBTQ + health education. Additionally, our intervention is notable because it is facilitated by LGBTQ + senior trainees with lived experience relevant to the content, in contrast to most didactics that are facilitated by faculty members.41,42 This peer-led approach corroborates previous student-guided educational interventions for LGBTQ + health in UME29,30 and leverages previous findings that medical trainees with personal connections to LGBTQ + individuals are more likely to have greater knowledge and more accepting attitudes towards LGBTQ + patients.50,51 Finally, while attendance was not mandatory, the content was assessed on graded examinations, harnessing the concept within medical education literature that suggests “assessment drives learning.” 52 These unique strengths of our study contribute to the growing body of literature on LGBTQ + medical education and offer practical strategies that can be implemented by other institutions.
To better capture medical students’ comfort with and knowledge of many common facets of caring for LGBTQ + patients, we created 6 competencies of LGBTQ + health in UME, which were defined to cover a broad variety of concepts, from the abstract (understanding how minority stress theory applies to LGBTQ + community members) to the concrete (guidelines for prescribing pre-exposure prophylaxis; Figure 1). It is worth noting that we operationalized these competencies because no LGBTQ + specific competencies currently exist at the institutional level, nor do they exist within accreditation bodies or national organizations devoted to improving medical education.45,48 Invariably, the competencies defined in this project may not encompass all aspects of caring for LGBTQ + patients; nevertheless, we believe that these 6 competencies of LGBTQ + health in UME can be extrapolated to other curricula and applied in many contexts (eg, didactic lectures, small-group cases, interactive patient encounters) to guide and evaluate medical student progress in delivering competent care to LGBTQ + patients.
Beyond the creation of these competencies, we sought to rigorously evaluate which specific competencies were addressed by our intervention. Through blinded faculty review, we identified targeted versus non-targeted competencies, a novel methodological approach not typically employed in LGBTQ + medical education interventions.42,48,49 Interestingly, we observed a global increase in all competencies rather than specific increases only in targeted competencies. While students accurately identified which competencies were taught when directly asked (95% correctly recognized targeted areas), they nonetheless reported improvements across all domains. This discrepancy likely arises from both educational and methodological factors. On one hand, foundational LGBTQ + health knowledge may genuinely enhance students’ overall professional confidence. However, we also acknowledge that assessment biases may have influenced our results. Social desirability bias may have motivated students to report improvements they believed researchers expected, though this effect is attenuated by using anonymous surveys. 53 Additionally, a halo effect could have caused positive learning experiences in targeted competencies to unconsciously enhance self-perception in unrelated competencies. 54 The apparent disconnect between content recognition and self-reported improvement demonstrates the limitations of self-assessment in educational research. Future work is warranted to incorporate objective measures of competency that are independent of self-perception bias, such as utilizing standardized patient encounters or knowledge tests, to help discern the etiology of these results. Future work should consider this methodological nuance of halo phenomena influencing content domains in self-reported assessments when working with survey data.
The significant interaction of LGBTQ + identity and competency score changes for targeted competencies may be influenced by response bias among responders in this non-mandatory lecture, as LGBTQ+-identifying students may be more likely to complete the survey than non-LGBTQ+-identifying students. Indeed, we observed that a disproportionately high number of our respondents identified as LGBTQ + (34% compared to 4.5% of the general population). 1 However, LGBTQ + respondents did not rate their competencies higher, underscoring the fact that more LGBTQ+-identifying students completing medical training does not necessarily imply that less training will be needed. Additionally, LGBTQ + students may have latent baseline knowledge that was differentially “activated” by the intervention; while baseline scores did not differ by LGBTQ + identity, they do not fully encapsulate prior familiarity with these topics. Finally, the significant interaction may be explained by a subjective validation effect, whereby the intervention additively reinforced prior experiences of LGBTQ+-identifying students.
Of note, our findings cannot be fully understood without contextualizing them within the extant literature. Prior LGBTQ + health curricula in UME have used faculty-led didactic sessions, longitudinal integrations, patient or community panels, and small-group case-based discussions.39,44,46,47 While these formats have demonstrated benefits in improving knowledge, attitudes, and comfort, they require substantial curricular time, faculty expertise, or institutional resources. 55 In contrast, we evaluated a brief, student-led, lecture that embedded within preclinical material. Our findings suggest that even a single targeted session can produce meaningful gains in self-reported competencies aligned with the content delivered, supporting the feasibility of concise, scalable models. Early placement in medical school may further promote foundational awareness and confidence prior to clinical exposure and help normalize LGBTQ + health competencies as core clinical skills.
A notable limitation of our study is sample size, which was influenced by our program's relatively small class size, the non-mandatory nature of the educational intervention, and the single institution included for data collection. Additionally, no formal a priori sample size calculation was performed, as this study was designed as a pilot educational evaluation. The sample size was determined by the size of the first-year medical student cohort and voluntary participation. It is important to note that the absence of an a priori sample size calculation may limit statistical power for subgroup analyses. Further, the study relied on self-reported competency measures derived from a locally developed questionnaire that was not formally validated prior to the study. Although the instrument was informed by established guidelines and underwent pilot review for clarity and face validity, the absence of formal psychometric validation limits the ability to draw conclusions about the reliability and generalizability of these measures. We were also limited by individual survey responses that could not be paired for analysis due to inconsistencies in the student-created identifier used to match pre-intervention and post-intervention surveys. Collaborative interventions across medical schools with similar curricula could enable us to draw stronger conclusions about the generalizability of our intervention. Finally, our study could be strengthened by objective measures of LGBTQ + health knowledge in addition to subjective ratings of competency increases, which would allow us to determine whether such interventions provided tangible improvements in clinical skills, as has been done previously. 46
Additional work is needed to characterize and optimize the effects of educational interventions in LGBTQ + health. Taken together, our results suggest that students feel more comfortable interacting with and providing care to LGBTQ + patients as a result of a peer-led educational intervention. The educational intervention we created and disseminated to students in this study is a robust example of the type of content needed in UME to meet the unique needs and risks of LGBTQ + patients.
A majority of the authorship team self-identifies as LGBTQ+, including both gender and sexual minority identities, and encompasses medical trainees, biostatisticians, and clinician-educators with demonstrated commitment to studying and caring for LGBTQ + populations.
Conclusion
This study demonstrates that a brief, student-led educational intervention embedded early in the preclinical curriculum can improve medical students’ self-reported LGBTQ + care competencies, with the greatest improvements in domains directly targeted by the session. By leveraging student leadership and integrating content into existing coursework, our approach offers a feasible and scalable model for addressing gaps in LGBTQ + health education and promoting inclusive clinical skills for underserved communities, including sexual and gender minority patients. Future work should examine the durability of effects, incorporate validated outcome measures, and test adaptation across diverse educational settings.
Supplemental Material
sj-docx-1-mde-10.1177_23821205261441402 - Supplemental material for Identifying and Improving LGBTQ + Health Competencies in First-Year Medical Undergraduate Education via a Targeted, Peer-Led Educational Intervention
Supplemental material, sj-docx-1-mde-10.1177_23821205261441402 for Identifying and Improving LGBTQ + Health Competencies in First-Year Medical Undergraduate Education via a Targeted, Peer-Led Educational Intervention by Andrew R. Kittleson, Casey M. Nichols, Caroline H. Castleman, Emily R. Wooder, Guanchao Wang, Jinyuan Liu, Anna Matthews, Christopher P. Terndrup and Steven Allon in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205261441402 - Supplemental material for Identifying and Improving LGBTQ + Health Competencies in First-Year Medical Undergraduate Education via a Targeted, Peer-Led Educational Intervention
Supplemental material, sj-docx-2-mde-10.1177_23821205261441402 for Identifying and Improving LGBTQ + Health Competencies in First-Year Medical Undergraduate Education via a Targeted, Peer-Led Educational Intervention by Andrew R. Kittleson, Casey M. Nichols, Caroline H. Castleman, Emily R. Wooder, Guanchao Wang, Jinyuan Liu, Anna Matthews, Christopher P. Terndrup and Steven Allon in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to thank Kaitlin McKernan, B.S., for help with collecting data; Hayden Shafer, M.D., for help with the blinded review of lecture material; and Eli Zimmerman, M.D., for contributions to the conceptualization of the project. The authors would also like to thank the participants of this research for their time and engagement.
ORCID iDs
Ethical Considerations
This study was granted exemption from the Vanderbilt University Institutional Review Board (IRB #230933); completion of surveys constituted consent to the research study. Participation was anonymous, voluntary, and uncoupled from graded assessments and course evaluation.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.