
Abstract
Background
Collaboration between doctors and midwives is critical for safe healthcare, and interprofessional education (IPE) can help ensure this. Despite emphasis on IPE, evidence on interventions specifically targeting medical and midwifery students has not been systematically synthesized. This review examined the effectiveness of IPE interventions between these professional groups and explored their educational experiences.
Methods
MEDLINE, Scopus, CINAHL, Maternity and Infant Care, and PsycINFO were searched for studies (2015-2025) involving interventions targeting interprofessional communication between undergraduate medical and midwifery students. Quantitative, qualitative, and mixed-methods studies were included. Two reviewers independently screened, extracted, and appraised studies using the Mixed Methods Appraisal Tool (2018). Quantitative results were narratively synthesized and qualitative data underwent thematic analysis.
Results
Sixteen studies (1,399 participants; eight countries) met inclusion criteria: five quantitative, six qualitative, and five mixed-methods studies. Interventions included simulation (most common), problem- and case-based learning, community placements, and anatomy sessions, lasting 3 hours to 3 years, delivered in-person, online, or hybrid. Quantitative findings demonstrated improvements across all six IPE domains (teamwork, roles/responsibilities, communication, learning/reflection, patient-centeredness, ethics/attitudes) with small to moderate effect sizes (standardized mean differences: 0.04-0.50). Validated instruments showed gains in collaborative attitudes, role understanding, and interprofessional skills. Qualitative synthesis revealed two main themes: facilitators of effective IPE, including enhanced collaborative learning, identity negotiation, experiential learning, and communication development, and implementation barriers such as hierarchies, scheduling, role confusion, and online delivery challenges.
Discussion
This first systematic review of IPE interventions between medical and midwifery students demonstrates that structured simulation-based IPE improves collaborative competencies. Effectiveness depends on addressing professional hierarchies, and careful curriculum integration. Early IPE implementation can foster collaboration, and reduce communication-related harm in maternal care.
Systematic review registration
PROSPERO CRD420251070277.
Keywords
Background
Healthcare education faces a persistent challenge: despite regulatory mandates for interprofessional education (IPE), medical and midwifery students often graduate with limited experience practicing together. 1 In medical education, professional competency extends beyond clinical knowledge to include collaborative practice skills. Although IPE is widely advocated by the World Health Organization (WHO) and required by professional regulators, undergraduate curricula often provide limited opportunities for structured interaction between medical and midwifery students. 2 Medical and midwifery programs often continue to operate in parallel rather than synergistically, resulting in few opportunities for students to learn with, from and about one another.3,4
This gap is significant because failures in interprofessional communication and collaboration continue to undermine care quality and safety.5-9 In maternal and newborn care, collaboration between doctors and midwives is vital for optimal outcomes. This professional dyad is especially critical in maternity services, where midwives and doctors must collaborate in the management of both uncomplicated pregnancy and birth and complications requiring escalation of care. 10 Reports into the Shrewsbury and Telford, 11 and East Kent maternity services 12 found that lack of empathy between practitioners and service users, and between different healthcare professionals, was a cause of avoidable harm. These findings have prompted calls for educational reform, making systematic evaluation of existing IPE approaches between medical and midwifery students both timely and essential for curriculum developers. Improving IPE between medical and midwifery students is therefore contribute to improved patient safety.
Educational theory supports early interprofessional contact to prevent stereotype formation and professional tribalism. Allport’s contact hypothesis suggests that structured interaction between professional groups under optimal conditions can reduce prejudice and improve collaboration. 13 Applied to healthcare education, this supports bringing medical and midwifery students together early in training. Conversely, when students train largely in isolation, professional silos may be reinforced, potentially compromising patient safety and high-quality care. 1 Although some scholars argue IPE may be more effective after qualification, once roles are established, this approach risks reinforcing rather than addressing entrenched stereotypes. 5
Key facilitators of interprofessional communication and collaboration include education and training, professional autonomy, role clarity, supportive environments, and shared goals. 14 IPE is widely recognized as an effective approach to preparing healthcare professionals for teamwork, fostering mutual respect, and improving patient safety and quality of care. 15 It is defined as the process by which two or more professional groups learn from, with, and about each other to enhance collaboration and improve health outcomes. 16 A range of curricular models have been implemented, including didactic programs, community-based experiences, and interprofessional simulations.17-19 IPE has also been classified as integrated or partially integrated depending on whether activities are embedded in the formal curriculum or delivered as extracurricular experiences. Regardless of format, the literature highlights the need for curriculum restructuring, flexibility in professional identity formation, and additional patient-centered approaches. 20
Previous systematic reviews have explored IPE between various healthcare students and professionals.21-25 However, despite this theoretical foundation and practical need, limited evidence investigates the effects and experiences of IPE interventions between medical and midwifery students specifically. To allow structured comparison of outcomes across studies, this review employs the established six-domain framework for interprofessional learning outcomes: teamwork, roles/responsibilities, communication, reflection, patient-centeredness, and ethics/attitudes. 26 A mixed-methods systematic review is therefore warranted. Quantitative evidence is needed to assess the effects of IPE interventions on interprofessional learning outcomes while qualitative evidence can explore how students experience these interventions, what barriers and enablers shape participation, and which features support meaningful learning. Synthesizing both forms of evidence will provide a more comprehensive basis for informing curriculum design and strengthening preparation for collaborative maternity care.
Objectives
1. To synthesize quantitative evidence on the effectiveness of interventions designed to enhance interprofessional communication between undergraduate medical and midwifery students. 2. To synthesize qualitative evidence on the experiences of medical and midwifery students who have undertaken IPE.
Methods
Study Design and Reporting Guidelines
This systematic review protocol was registered in PROSPERO on 10th June 2025 (Prospero registration ID: CRD420251070277). We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidance for reporting 27 and the Synthesis Without Meta-analysis (SWiM) reporting guideline for narrative synthesis. 28 The PRISMA checklist is presented in Appendix 1. No protocol deviations occurred during the review process. No patients or members of the public were involved in the design, conduct, or reporting of this systematic review because the review synthesized data from previously published studies and did not involve primary data collection. Ethical approval was not required for this systematic review.
Eligibility Criteria
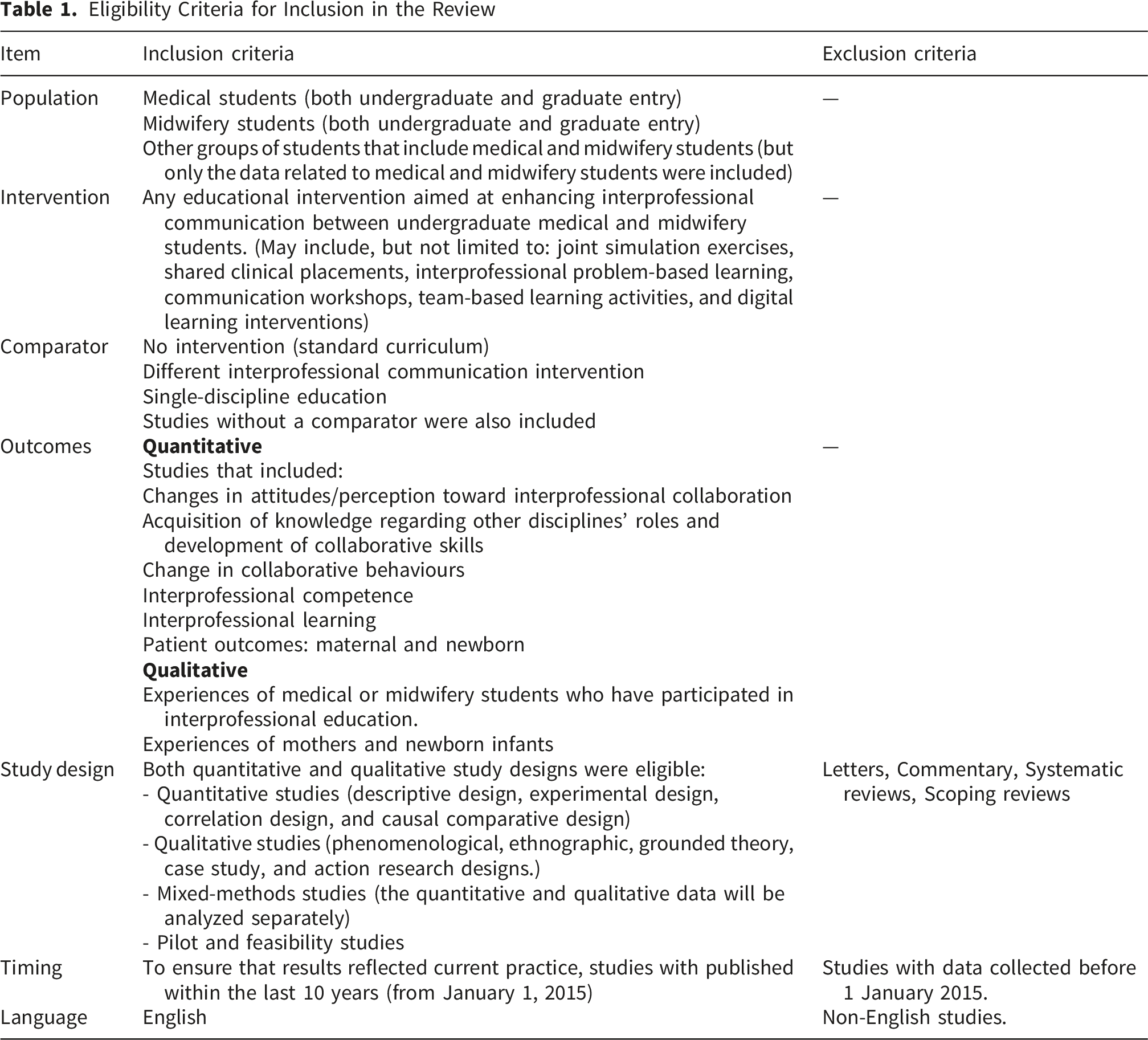
Search Strategy and Study Selection
The search strategy was developed in collaboration with an experienced information specialist (KN) with expertise in healthcare databases and systematic review methodology. Search terms were validated by testing against a sample of known relevant studies identified through preliminary scoping. The strategy combined controlled vocabulary (MeSH terms) and free-text terms related to medical students, midwifery students, and interprofessional education.
We searched five electronic databases: MEDLINE (via Ovid), Scopus, CINAHL Plus, APA PsycINFO, and the Maternity and Infant Care Database. The MEDLINE strategy (Appendix 2) was adapted for other databases, accounting for differences in indexing terms and search functionalities. The final search was conducted on May 29, 2025.
To identify additional relevant studies, we hand-searched reference lists of included studies and relevant systematic reviews. We also searched conference proceedings from key IPE conferences (2020-2025), key IPE journals and contacted experts in the field to identify unpublished studies.
Search results from all databases were imported into EndNote 30 version 20 for initial deduplication. Remaining records were uploaded to Rayyan 31 for screening. Two reviewers (NA and SOS) independently conducted pilot screening on 50 records to calibrate their approach and ensure consistent application of inclusion criteria. Following satisfactory agreement (κ > 0.8), the reviewers independently screened all titles and abstracts.
Full-text screening was conducted independently by the same two reviewers for all potentially eligible studies. Disagreements at both screening stages were resolved through discussion, with a third reviewer (JH) consulted when consensus could not be reached. Inter-rater reliability was calculated using Cohen’s kappa, a measure of agreement between two raters, for both title/abstract screening (κ = 0.85) and full-text screening (κ = 0.89).
Data Extraction and Quality Assessment
A standardized data extraction form was developed based on the Cochrane data collection form and piloted on three included studies. The form was refined following pilot testing to ensure clarity and completeness. Data was extracted from all included studies by two reviewers (NA and SOS) independently, with discrepancies resolved through discussion.
Extracted data included: study characteristics (author, year, country, setting, study design, duration); participant characteristics (sample size, demographics, educational level, recruitment method); intervention details (type, duration, delivery mode, theoretical framework); comparator details (where applicable); outcome measures and results; risk of bias indicators; and funding sources.
For studies with insufficient reported data, we contacted corresponding authors via email (maximum three attempts over four weeks) to request additional information. Inter-rater reliability for data extraction was assessed using percentage agreement for categorical variables and intraclass correlation coefficients for continuous variables (overall agreement: 94%).
The risk of bias in the included studies was independently assessed by NA and SOS using the Mixed Methods Appraisal Tool (MMAT), version 2018. 32 The MMAT is designed for reviews combining qualitative, quantitative, and mixed-methods studies. Each study was assessed with the relevant criteria; mixed studies were evaluated across all applicable domains. Disagreements were resolved by consensus or by a third reviewer (JH). Following MMAT guidance, an overall score wasn’t calculated; instead, strengths and limitations were reported against appraisal criteria in a summary table.
Data Synthesis
Quantitative and qualitative outcomes were synthesized using the six-domain framework for IPE learning outcomes: teamwork, roles/responsibilities, communication, learning/reflection, patient-centeredness, and ethics/attitudes. 26 This framework provided a comprehensive structure for understanding IPE effectiveness across multiple domains, and supported mapping both quantitative and qualitative findings to a common conceptual model.
Due to substantial heterogeneity in study populations, interventions, outcome measures, and study designs, statistical meta-analysis was not appropriate. We followed guidance from the Cochrane Handbook 33 and conducted a structured narrative synthesis. For studies reporting pre-post comparisons with sufficient data, we calculated standardized mean differences (SMDs) with 95% confidence intervals using Cohen’s d, where possible. When studies reported different outcome scales measuring the same construct, we converted scores to a common 0-1 scale to enable comparison. For studies reporting only summary statistics (medians, ranges), we described results narratively.
We conducted vote counting based on direction of effect, categorizing results as showing improvement (effect size > 0), no change (effect size ≈ 0), or deterioration (effect size < 0). While acknowledging the limitations of vote counting, this approach provided a systematic method for summarizing findings across diverse outcome measures. Effect size interpretation followed established conventions: small (d = 0.2), medium (d = 0.5), and large (d = 0.8) effects. Results were tabulated by outcome domain to facilitate comparison across studies.
Qualitative data underwent inductive thematic analysis following Braun and Clarke’s six-phase framework. 34 Qualitative data was coded by two reviewers (NA and SOS) independently, with regular discussions to compare emerging codes. Initial codes were grouped into potential themes, which were reviewed and refined through an iterative process. Theme development involved both inductive identification of patterns within the data and deductive application of the six IPE learning domains framework. Inter-rater reliability for final theme assignment was assessed using Cohen’s kappa (κ = 0.82).
For mixed-methods studies, quantitative and qualitative components were analyzed separately using the respective approaches described above, then integrated during interpretation. Quantitative and qualitative findings were integrated using a convergent synthesis approach, with results compared and contrasted to identify areas of convergence, complementarity, and divergence. This integration was conducted through team discussion involving all authors.
Data management was conducted using Microsoft Excel 2021. Statistical calculations for effect sizes were performed using RevMan 5.4 where appropriate. Qualitative analysis was supported by NVivo 12 for data organization and coding.
Certainty of Evidence
The certainty of evidence for quantitative outcomes was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. 35 Certainty was assessed by two reviewers independently across five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Disagreements were resolved through discussion. Evidence certainty was rated as high, moderate, low, or very low. Summary of findings tables incorporating GRADE assessments were prepared for all primary outcomes.
Results
The search identified 1,981 studies. After de-duplication and screening, 16 studies (1,399 participants; 914 medical students and 485 midwifery students) were included in the review (Appendix 3). The identification and selection process, along with the reasons for excluding studies, are detailed in the PRISMA flow diagram (Figure 1). The list of excluded studies is presented in Appendix 4. This section describes the characteristics of included studies and types of interventions evaluated, followed by the risk of bias assessment, certainty of evidence, quantitative findings across the six IPE domains, and qualitative themes relating to facilitators and barriers to effective IPE. PRISMA flow diagram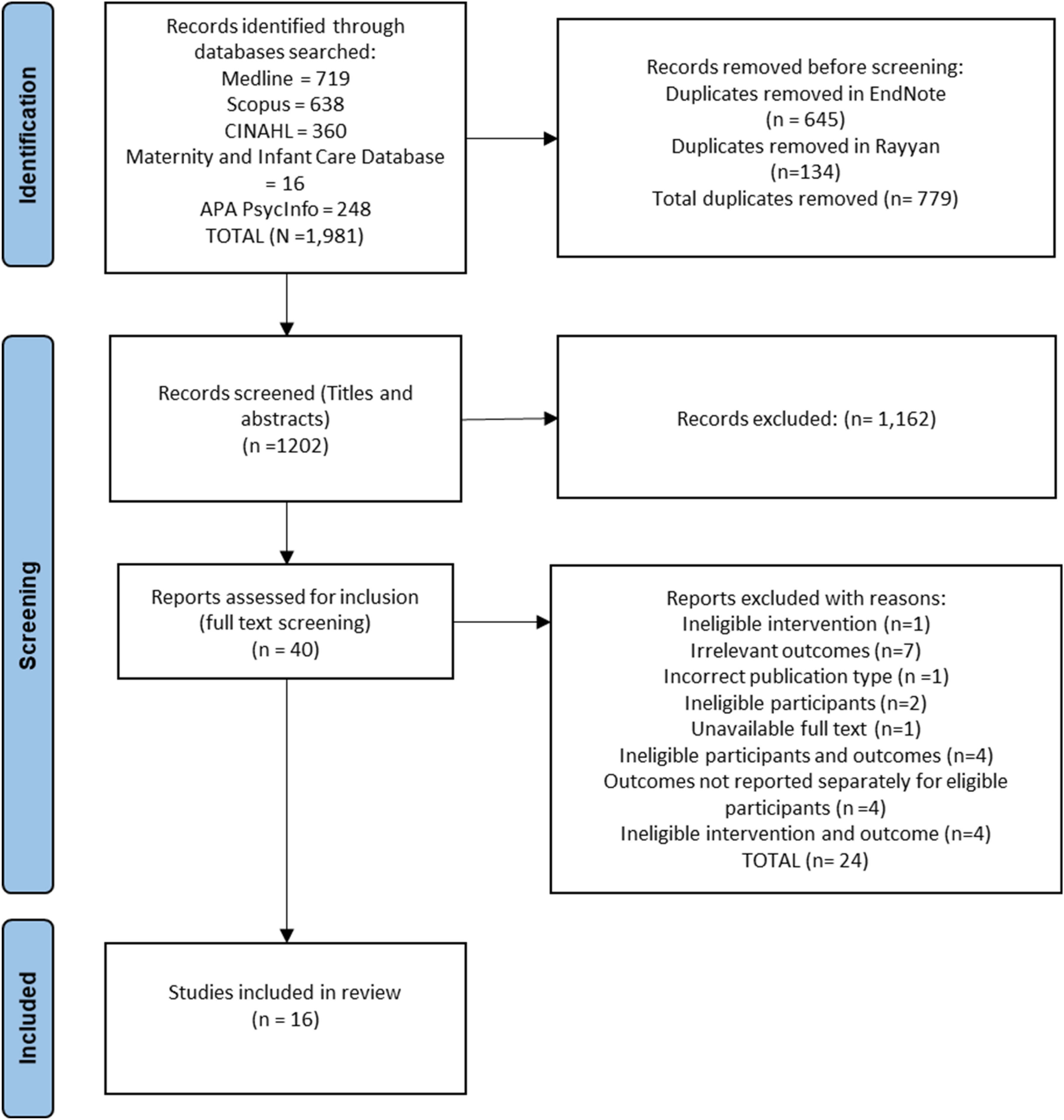
Characteristics of Included Studies
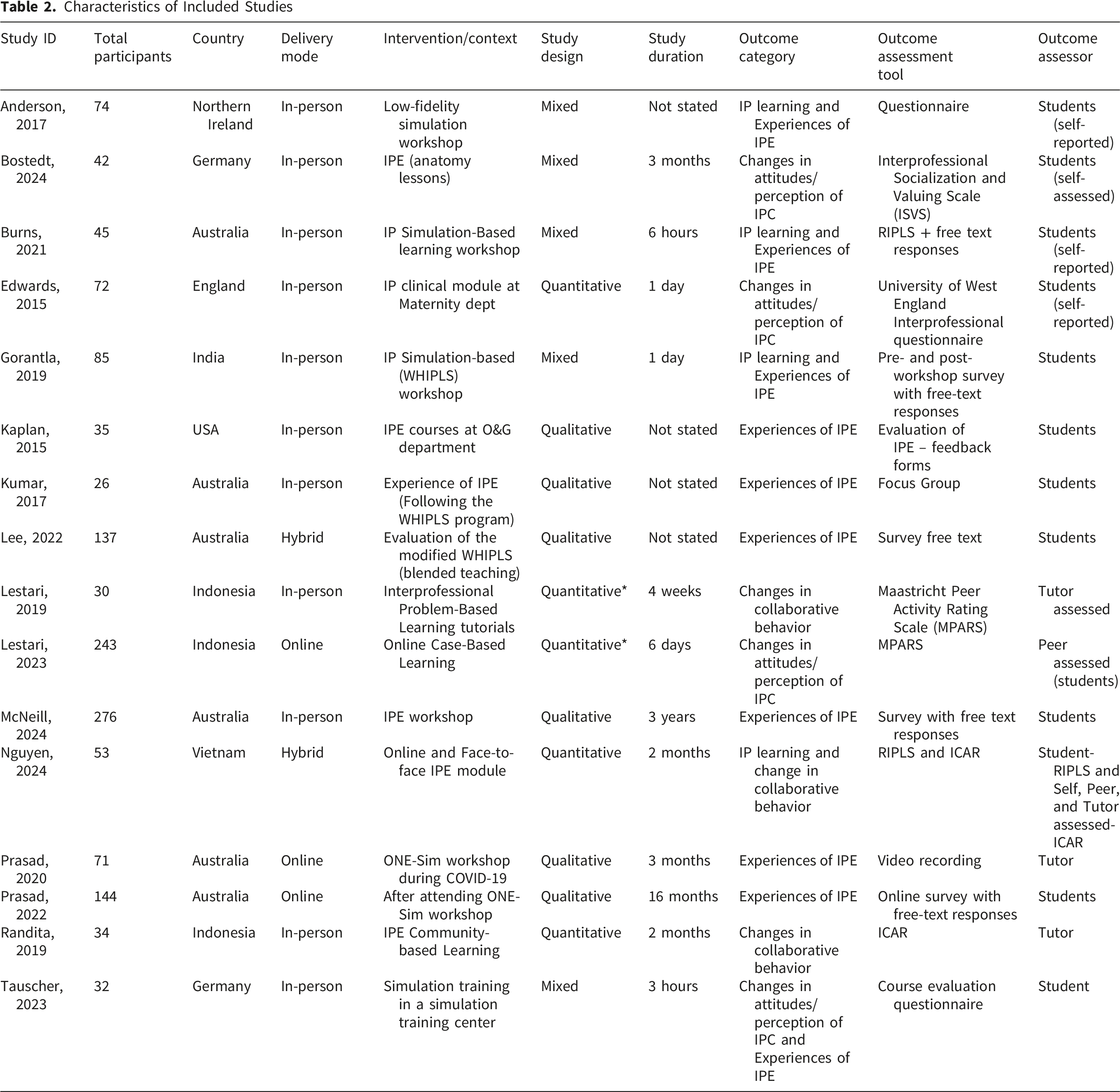
Of the included studies, five were quantitative, six were qualitative, and five were mixed study designs. Two of the studies classified as purely quantitative were mixed-methods but only the quantitative components met the inclusion criteria and were deemed eligible for this review.36,37
One included study was conducted in England, six in Australia, three in Indonesia, two in Germany, and one each in India, Northern Ireland, Vietnam, and the United States. All studies were conducted between 2015 and 2024, with reported study durations ranging from 3 hours to 3 years.
Characteristics of Included Studies
Overview of Study Findings Across IPE Outcomes Domains
CI=confidence interval; ISVS= Interprofessional Socialization and Valuing Scale; UWES= University of West England interprofessional questionnaire; RIPLS= Readiness for Interprofessional Learning Scale; ICAR= Interprofessional Collaborator Assessment Rubric instrument; MPARS= Maastricht Peer-Activity Rating Scale; MCIPS= Maclead clark professional identity scale.
Interventions
The interventions involved in-person, online, or hybrid interprofessional learning among medical and midwifery students. Three studies included other health professional students, but only the data separately reported for medical and midwifery students were included in this review.36,37,44 Most participants were senior students (Years 4 -5 medical students and Year 3 or final year midwifery students). IPE interventions involved simulation-based workshops such as a low-fidelity simulation-based workshop where midwifery students taught medical students the concepts of physiological labor and birth, 17 and others using standardized patients and mannikins to simulate birth scenarios/obstetric emergencies.27,44,45 Three studies conducted simulation workshops based on the Women’s Health Interprofessional Learning through Simulation (WHIPLS). One mixed study, 38 and one qualitative study 46 evaluated the standard WHIPLS program while another qualitative study evaluated a modified hybrid version of the programme. 43 The WHIPLS is a training for medical and midwifery students on clinical skills and understanding the roles and relationships with other professional team members. 46
Educators employed various teaching techniques in the workshop, including clinical skills training, lectures, and pre-reading material. Tutor assessed 41 and student-assessed 42 versions of the Obstetric and Neonatal Emergency Simulation (ONE-Sim) workshop were also conducted. This involved teaching through simulation of obstetric emergencies to improve interprofessional communication and teamwork between medical and midwifery students. Other approaches involved Problem-Based Learning tutorials, 36 or Case-based learning discussions, 37 a community-based IPE program for students, 40 an interprofessional teaching of Anatomy lessons, 47 and an interprofessional course on clinical topics in a hospital maternity department. 48 Additionally, there was an interprofessional curriculum update to include midwifery students in two established courses (U-Teach and Life course) for medical students that involved lectures, clinical skills training, and laboratory training, 39 and an IPE workshop featuring a LEGO®-based interprofessional ice-breaker activity in which students built their “ideal birthing room”. 49
Risk of Bias Assessment
The results of the assessment are presented in Figure 2 and the questions in the MMAT tool for the different study designs are presented in Appendix 5. All studies were included in the analyses irrespective of their risk of bias assessment, as no overtly biased studies were identified. Risk of bias assessment using MMAT v2018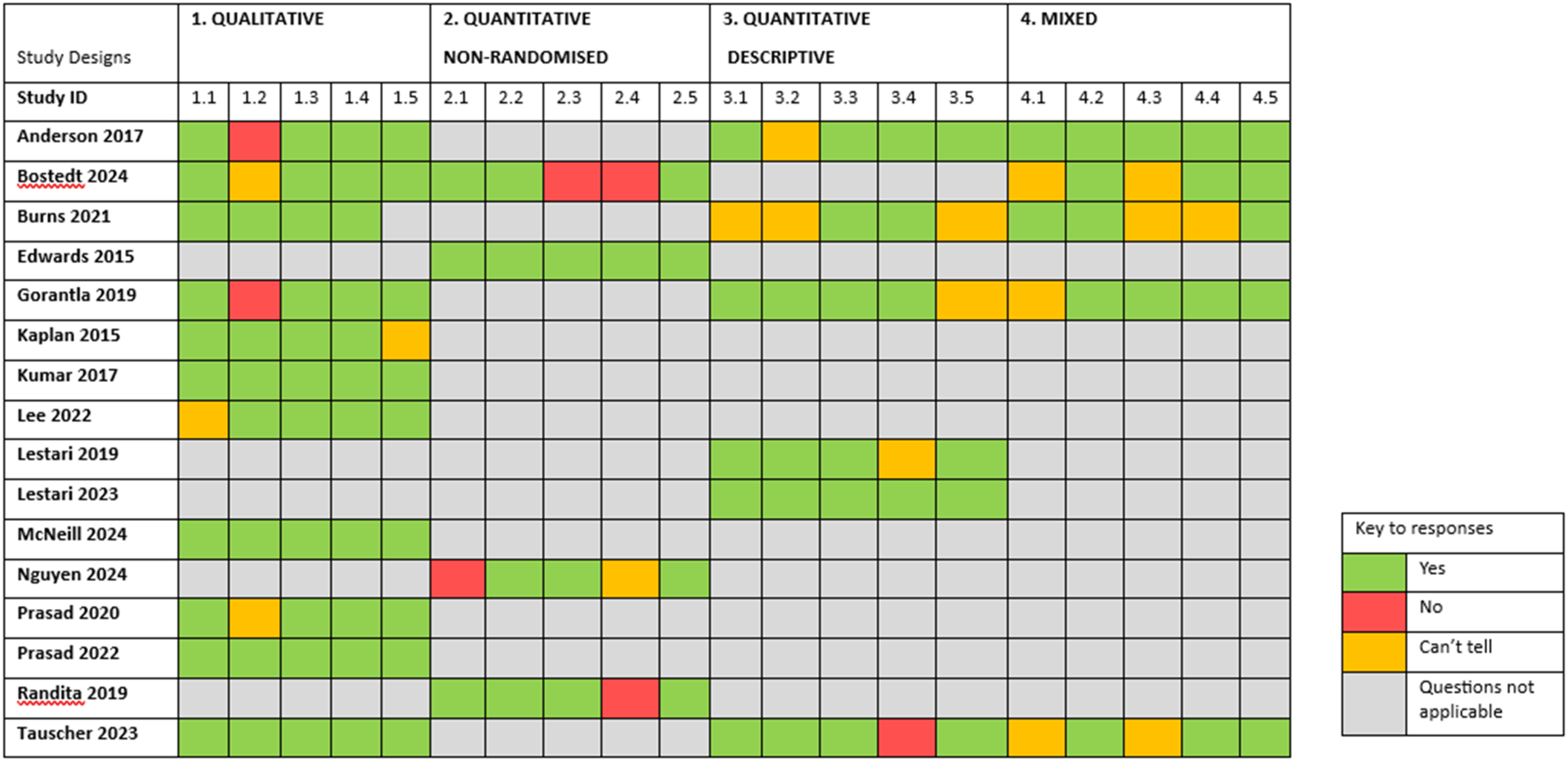
In the quantitative studies, the appropriateness of outcome measures, the evaluation of interventions, and the fidelity of intervention delivery were deemed satisfactory.40,44,47,48 However, some studies raised concerns regarding potential bias due to inadequate consideration of confounders in their design and analysis.40,44,47 Most quantitative studies used representative samples,36-38,40,45,47,48 the sampling strategy was methodologically appropriate to address the research question and the measurement approaches were aligned with the study objectives.17,27,36-38,45
Among qualitative studies, limitations were most frequently observed in the adequacy of the data collection methods to address the research questions.17,38,41,47
In the mixed-methods studies, several did not clearly justify the rationale for employing a mixed-methods design38,45,47 and the interpretation of quantitative–qualitative integration.27,45,47 However, the individual components of the studies generally adhered well to their respective methodological quality criteria.
Confidence in Evidence
The summary of findings and the GRADE assessment of the certainty in the evidence from the studies is presented in Appendix 6. The certainty of evidence for all the six quantitative outcomes was very low.
Quantitative Results and Synthesis
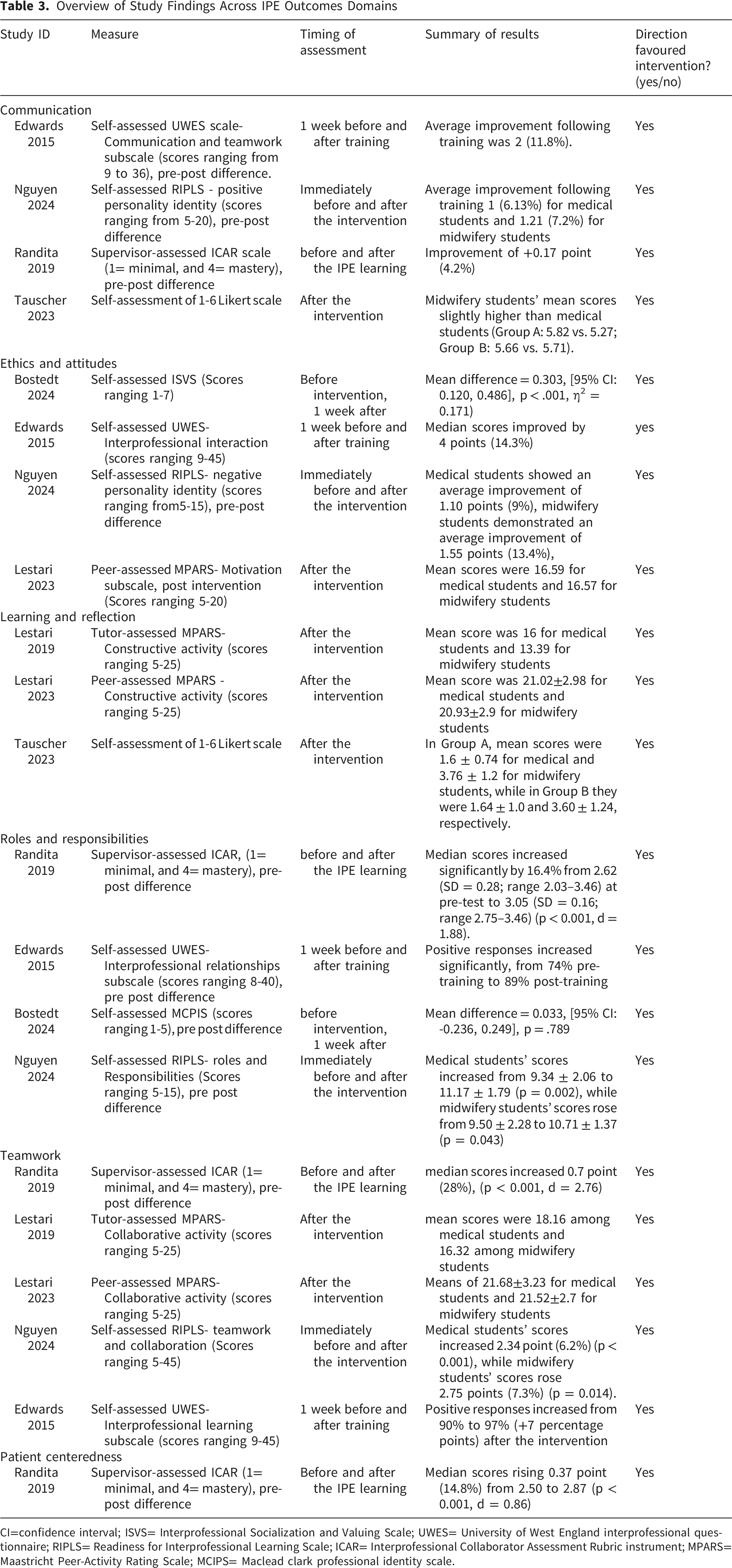
The quantitative outcomes of IPE were categorized based on the six IPE learning outcomes/themes described in a literature review: teamwork, roles/responsibilities, communication, learning/reflection, patient centeredness, and ethics/attitudes. 26 In most studies, outcomes were reported by the participating students. Quantitative measures used to assess various domains of interprofessional learning and collaboration, including the Interprofessional Socialization and Valuing Scale (ISVS), 47 the University of West England interprofessional questionnaire (UWES), 48 the Maastricht Peer-Activity Rating Scale (MPARS),36,37 the Readiness for Interprofessional Learning Scale (RIPLS), 44 and the Interprofessional Collaborator Assessment Rubric instrument (ICAR). 40 All studies revealed a positive effect of IPE (see Table 3).
Communication
Four studies assessed communication, using ICAR, 40 UWES, 48 RIPLS, 44 and a self-developed instrument. 45 Three studies relied on self-assessment,44,45,48 while another study used supervisors’ assessment. 40 Three of the studies collected pre- and post-intervention data.40,44,48
Using the UWES scale (scores ranging from 9 to 36), the average improvement following training was 2 (11.8%) from median pre- to post-training (19.0 vs. 17, p < 0.001), with positive responses significantly increased from 69% to 89% post-training (p = 0.0043). 48
On a 4-point supervisor-assessed ICAR scale (1= minimal, and 4= mastery), one study observed improvement of +0.17 point (4.2%), from a pre-test median of 2.87 (SD = 0.22; range 2.29–3.16) to a post-test median of 3.04 (SD = 0.20; range 2.79–3.33), with a large effect size (d = 1.33, p < 0.001). 40
One study reported that communication competency using RIPLS (scores ranging from 5-20) medical students’ mean scores increased 1 point (6.13%) from 16.31 ± 1.77 to 17.31 ± 1.56 (p = 0.007), while midwifery students improved 1.21 point (7.2%) from 16.67 ± 2.04 to 17.88 ± 1.51 (p = 0.009). 44 Another study compared professional groups post-intervention using self-assessed 1-6 Likert scale, with midwifery students mean scores slightly higher than medical students (Group A: 5.82 vs. 5.27; Group B: 5.66 vs. 5.71). 45
External assessment (by tutors or supervisors) tended to show slightly higher improvements than self- or peer-assessment. Certainty of evidence was very low.
Ethics and Attitudes
Four studies assessed ethics and attitudes, using self-assessment tools: ISVS; 47 UWES 48 and RIPLS 44 ) and one peer-assessment tool (MPARS). 37 Three studies collected self-assessed pre- and post- intervention data.44,47,48
Using the 5-point RIPLS (score range 5–15), medical students showed an average improvement of 1.10 points (9%), increasing from 12.21 ± 2.34 to 13.31 ± 1.48 at (p = 0.005). Similarly, midwifery students demonstrated an average improvement of 1.55 points (13.4%), from 11.58 ± 2.99 to 13.13 ± 2.36 (p = 0.041). 44 In one study, a significant immediate improvement in ethics and attitudes was observed, with a strong effect size (mean difference = 0.303, [95% CI: 0.120, 0.486], p < .001, η2 = 0.171), though scores had declined to nearly baseline levels at 12 weeks. 47 Using UWES (scores ranging from 9-45), median scores improved by 4 points (14.3%) from 32 to 28. 48 Another study, using MPARS post-intervention, reported mean scores were 16.59 for medical students and 16.57 for midwifery students. 37 The certainty of the evidence was very low.
Learning and Reflection
Learning and reflection was assessed in three studies using peer-assessed MPARS, 37 tutor-assessed MPARS, 36 and self-assessed questionnaire developed by the authors. 45 The outcome was only assessed after the intervention. One study used tutor-assessed MPARS (scores ranging 5-25) reported the mean score was 16 for medical students and 13.39 for midwifery students. 36 In contrast, when MPARS was assessed by peers, the mean score was higher 21.02±2.98 for medical students and 20.93±2.9 for midwifery students. 37 Another study compared two student groups. 45 In Group A, mean scores were 1.6 ±0.74 (medical) and 3.76 ±1.2 (midwifery), while in Group B the scores were 1.64 ±1 (medical) and 3.60 ±1.24 (midwifery). 45 In both groups, medical students scored higher than midwifery students. 45 Certainty of evidence was very low.
Roles/Responsibilities
Four studies assessed outcomes related to roles and responsibilities before and after the intervention, using ICAR, 40 UWES, 48 Maclead Clark Professional Identity Scale (MCPIS) 47 and RIPLS. 44 One study relied on supervisor ratings. 40 Three studies used self-assessments only.44,47,48
One study, used 4-point ICAR, found that role and responsibility median scores increased significantly by 16.4% from 2.62 (SD = 0.28; range 2.03–3.46) at pre-test to 3.05 (SD = 0.16; range 2.75–3.46) (p < 0.001, d = 1.88). 40 One study found Both medical and midwifery students reported significant improvements in roles and responsibilities. Medical students’ scores increased from 9.34 ± 2.06 to 11.17 ± 1.79 (p = 0.002), while midwifery students’ scores rose from 9.50 ± 2.28 to 10.71 ± 1.37 (p = 0.043). 44 Also, one study found that positive responses increased significantly, from 74% pre-training to 89% post-training. 48 In contrast, another study found no significant pre–post change in 5-point MCPIS scores (mean difference = 0.033, [95% CI: -0.236, 0.249], p = .789). 47 Certainty of evidence was very low.
Teamwork
Five studies explored teamwork using supervisor-assessed ICAR, 40 tutor-assessed MPARS, 36 peer-assessed MPARS, 37 self-assessed UWES, 48 and self-assessed RIPLS. 44 One study reported median scores increased 0.7 point (28%) from 2.50 (SD = 0.31; range 1.75–3.20) at pre-test to 3.20 (SD = 0.20; range 2.90–3.65) at post-test (p < 0.001, d = 2.76). 40 one study found self-assessed RIPLS (scores ranging 5-45) found medical students’ scores increased 2.34 point (6.2%) from 37.59 ± 3.36 to 39.93 ± 2.98 (p < 0.001), while midwifery students’ scores rose 2.75 points (7.3%) from 37.50 ± 4.75 to 40.25 ± 2.74 (p = 0.014). 44 Another study reported that positive responses which were already high at 90%, increased to 97% (+7 percentage points) after the intervention. 48
Two studies assessed teamwork only after the intervention, focusing on constructive collaboration, including willingness to share information, influence on group members and commitment to the group.36,37 A problem-based study found tutor-assessed MPARS (scores ranging 5-25) mean scores were 18.16 among medical students and 16.32 among midwifery students. 36 While a case-based learning study reported peer-assessed means of 21.68±3.23 for medical students and 21.52±2.7 for midwifery students. 37 Certainty of evidence was very low.
Patient Centeredness
Patient-centeredness outcome reflects aspects of patient-centered care, understanding patient needs, and ensuring safety in interprofessional practice. 26 One study evaluated this outcome using the supervisor-assessed 4-point ICAR tool, 40 and reported significant improvements in collaborative patient-centered approaches, with median scores rising 0.37 point (14.8%) from 2.50 to 2.87 (p < 0.001, d = 0.86). 40 Certainty of evidence was very low.
Qualitative Results and Synthesis
Eleven studies contributed qualitative data to this synthesis: six standalone qualitative studies conducted in Australia (n=5) and USA (n=1), and five mixed-methods studies from Northern Ireland, Australia, India, and Germany (n=2). Data collection methods included free-text survey responses (n=6), focus group discussions (n=2), evaluation surveys (n=2), and video recordings of student discussions (n=1). Thematic analysis was conducted using both deductive application of the six IPE learning domains framework and inductive identification of emerging patterns. Inter-rater reliability for final theme assignment was κ = 0.82, with disagreements resolved through discussion. This section presents qualitative themes relating to facilitators of effective IPE and barriers and contextual factors influencing its implementation. Additional supporting quotes are presented in Appendix 7.
Core Theme: Facilitators of Effective IPE
Students consistently valued interprofessional learning opportunities that enabled knowledge sharing and mutual skill development. Ice-breaker activities emerged as particularly effective for establishing collaborative relationships, with one study demonstrating how structured introductory exercises promoted teamwork, communication, and delegation skills from the outset. 49 Post-simulation debriefing sessions were identified across multiple studies as crucial for consolidating learning and processing challenging interprofessional dynamics.41,45 One midwifery student reflected, “Really enjoyed it and it allowed us to show our knowledge of labor and birth… working as a group we were able to utilize each other’s skills.” 17
The collaborative learning environment enabled students to develop shared goals focused on patient benefit, transcending professional boundaries. As one midwifery student noted, “I believe we all have roles and contributions to care for a patient - today’s communication and interaction demonstrated we are all there for a shared goal: to provide the best care for a woman, her baby, and her family.” 27
A related theme was professional identity negotiation. Students often began with hierarchical assumptions, but these were challenged through interprofessional contact. Medical students often began with perceived superiority but discovered significant knowledge gaps, particularly regarding physiological birth processes. Conversely, midwifery students demonstrated clinical expertise while initially feeling intimidated by medical students’ perceived status. As one midwifery student commented, “I enjoy having the interprofessional workshops, provides an opportunity for midwifery and medical students to understand the role of each other more clearly.” 42 Despite initial imbalances, sustained interaction fostered mutual respect and appreciation for complementary professional strengths. Studies reported that students learned to value each other’s perspectives and developed supportive relationships.17,46
Experiential learning in safe environments was also consistently valued. Simulation-based IPE was consistently praised for providing hands-on learning opportunities without patient risk. Students valued the ability to practice procedures repeatedly, make mistakes safely, and receive immediate feedback. The ‘low-pressure’ nature of simulation environments, characterized by absence of time constraints and real patient consequences, facilitated confident skill development.38,43,46 For example, one midwifery student noted, “Simulation workshop is very effective as compared to clinical session or tutorial. During tutorial we only get theoretical knowledge and during clinical sessions we do not get much opportunity,” 38 while a medical student reported, “Able to do things more than once. Easier to practice techniques and get immediate feedback.” 43
IPE interventions consistently improved students’ interprofessional communication abilities and perspective-taking skills. Structured interprofessional activities, including anatomy lessons and case discussions, facilitated meaningful dialogue and mutual understanding.47,49 One medical student said, “The exchange allowed us to have meaningful discussions and share common interests,” 47 while a midwifery student reported, “It was good to compare ideas and discuss values when it comes to care and priorities with birthing women.” 49
Core Theme: Implementation Barriers and Challenges
Despite positive learning outcomes, entrenched professional hierarchies created significant challenges. Medical students sometimes received preferential learning opportunities, while midwifery students experienced marginalization during demonstrations and procedures. 38
Some interactions revealed deep-seated professional tensions, with both groups displaying defensive attitudes. For example, a medical student reflected, “We see the midwifery students being of equal standing, however they radiate a sense of superiority and dislike to medical profession.” 27 In online environments, these tensions could become more pronounced, with some sessions deteriorating into professional tribalism. 42
Logistical and structural constraints were also common. Scheduling emerged as the most frequently cited implementation barrier. When IPE programs were added to existing medical curricula without corresponding adjustments to midwifery schedules, midwifery students struggled to participate fully, missing sessions due to competing clinical commitments. 39 Role confusion represented another significant barrier, with midwifery students uncertain whether they were co-learners or teaching assistants in sessions originally designed for medical students, as one midwifery student reflected, “I think it was really confusing what our role as midwifery students was. We were never introduced. Then we knew most of the content really well, so I felt like a teaching assistant.” 39
Technology-mediated learning introduced additional challenges. The COVID-19 pandemic necessitated online IPE delivery, revealing both opportunities and significant constraints. While students acknowledged the value of continued interprofessional contact during restrictions, they identified substantial limitations affecting learning quality.42,43 One medical student reported, “It was hard to concentrate… since the online workshop was held on a day of many other lectures… many of us would have zoomed out due to Zoom fatigue.” 43 Despite limitations, some students appreciated online learning’s accessibility and flexibility. 42
Several contextual factors also shaped IPE experiences. Across multiple studies, medical students were characterized as more task-oriented, focusing on clinical procedures and diagnostic processes, while midwifery students demonstrated greater relationship-orientation, emphasizing holistic, woman-centered care.27,42 These philosophical differences, rather than representing barriers, often provided valuable learning opportunities for students to understand alternative approaches to healthcare delivery. While some medical students felt overwhelmed by midwifery students’ superior obstetric knowledge, others appreciated learning from more experienced peers. Midwifery students valued opportunities to share their expertise while learning about medical perspectives on maternity care.
Discussion
Summary of Findings
This systematic review of 16 studies involving 1,399 participants across eight countries demonstrate three principal findings. First, simulation-based IPE interventions consistently improve collaborative competencies between medical and midwifery students across all six learning domains (teamwork, roles/responsibilities, communication, learning/reflection, patient-centeredness, and ethics/attitudes), with effect sizes ranging from small to moderate. Second, while initial professional hierarchies and role confusion present significant implementation barriers, these can be overcome through structured, early intervention approaches with clear learning objectives and facilitated reflection. Third, successful IPE implementation depends critically on curriculum integration rather than add-on approaches, with scheduling conflicts and regulatory constraints identified as primary barriers requiring systematic institutional solutions.
Comparison With Existing Literature
To our knowledge, this review provides the first comprehensive synthesis of evidence specifically examining IPE interventions between medical and midwifery students. Previous systematic reviews have examined IPE broadly across healthcare disciplines,23-25 but none have focused on this critical professional dyad in maternal care. This review contributes novel insights into the understanding of professional identity formation in this context, revealing that traditional healthcare hierarchies manifest even at the student level. In several studies, medical students displayed perceived superiority, despite sometimes less clinical knowledge in obstetric settings than their midwifery counterparts. This finding challenges assumptions about the timing and nature of interprofessional relationships. 50 Our findings align with broader IPE systematic reviews demonstrating positive attitude and knowledge changes among healthcare students, 24 but extend this evidence by identifying unique challenges in the medical-midwifery dyad not previously documented. The hierarchical tensions we identified reflect broader literature on doctor-midwife relationships in clinical practice, 14 suggesting that educational interventions may need to explicitly address these dynamics.
The consistent effectiveness of simulation-based approaches supports recent calls for increased simulation integration in medical education, while highlighting regulatory barriers specific to midwifery education not addressed in general IPE literature. Our finding that external assessment yields higher improvement scores than self-assessment aligns with educational measurement literature emphasizing the importance of objective evaluation. Unlike previous reviews focusing on established healthcare professionals or broader student populations, our analysis reveals the formative nature of interprofessional relationships during undergraduate education. Midwifery students often possessed superior clinical knowledge in obstetric settings, from their intensive studies compared with medical students. The identification of specific implementation barriers—particularly scheduling conflicts and regulatory constraints—offers practical insights missing from broader IPE reviews. Our detailed analysis of online versus in-person delivery modes, accelerated by COVID-19 adaptations, contributes to emerging literature on remote IPE.
These findings advance several theoretical frameworks relevant to medical education. From a professional identity formation perspective, the results support early IPE intervention to shape collaborative identities before hierarchical attitudes become entrenched. The observation that medical students initially displayed superiority despite clinical knowledge gaps suggests that professional identity formation occurs rapidly and may be influenced more by societal perceptions than actual competence. Social contact theory receives support from our findings, with structured interprofessional interaction under optimal conditions reducing prejudice and improving collaboration.
However, the identification of hierarchical tensions suggests that contact alone is insufficient; facilitation and reflection are essential components for positive outcomes. The educational effectiveness demonstrated across multiple learning domains supports constructivist learning principles, with students actively building understanding through collaborative problem-solving in authentic contexts. The superior outcomes observed with simulation-based approaches align with experiential learning theory, emphasizing the importance of hands-on practice in safe environments.
Strengths and Limitations
The review demonstrates several methodological strengths that enhance confidence in findings. The comprehensive search strategy across five databases with no geographical restrictions resulted in international representation from eight countries, supporting generalizability across different healthcare systems and educational contexts. The rigorous dual-reviewer process for all selection, extraction, and quality assessment stages, with high inter-rater reliability (κ > 0.80 for all processes), minimizes bias and increases reliability of findings. The use of established frameworks enhances analytical rigor. Application of the six-domain IPE learning outcomes framework 26 provides structured analysis enabling comparison across diverse interventions, while the Mixed Methods Appraisal Tool offers systematic quality evaluation appropriate for the heterogeneous study designs included. The mixed-methods synthesis approach represents a particular strength, combining quantitative effect size analysis with rich qualitative insights about student experiences. This integration provides both evidence of effectiveness and understanding of implementation factors crucial for practical application.
Several limitations constrain the strength of conclusions. The very low certainty of evidence across all quantitative outcomes, primarily due to study heterogeneity and reliance on self-reported measures, limits definitive statements about intervention effectiveness. The inability to conduct meta-analysis due to diverse outcome measures and study designs prevents precise effect size estimation. Geographical bias may affect generalizability, with six of 16 studies conducted in Australia and only one in England, potentially limiting applicability to UK healthcare and educational contexts. The predominance of short-term outcome assessment (most studies measured immediate post-intervention effects) provides limited evidence about sustained behavioral change or long-term impact on professional practice. Relatedly, our study focused on studies conducted in the last 10 years. Previous studies may have provided relevant data. On the other hand, our aim was to identify current practice, and in the context of rapidly changing healthcare environment, introducing older studies could have confounded the results. Risk of bias assessment also revealed concerns about confounding variables and data collection methods in several studies, while publication bias cannot be ruled out as studies with null or negative findings may be less likely to be published.
Implications for Practice and Policy
The evidence supports integrating IPE into core medical and midwifery curricula rather than treating it as optional enhancement. Early implementation during Years 1-2, when professional identities are more malleable, appears optimal for challenging stereotypes and building collaborative relationships. The graduated approach suggested by our findings—beginning with low-stakes socialization activities and progressing to high-fidelity simulation—provides a practical framework for curriculum development. Assessment strategies should incorporate validated instruments (ISVS, RIPLS, ICAR) to demonstrate educational value and support continuous improvement. The superior outcomes observed with external assessment emphasize the importance of skilled facilitation rather than student-led activities.
Accreditation standards for both medical and midwifery programs should include specific IPE requirements to drive implementation and ensure systematic attention to collaborative competency development. Investment in faculty development for interprofessional teaching represents a crucial infrastructure need requiring institutional and policy-level support. The evidence suggests that healthcare organizations should extend IPE initiatives beyond undergraduate education into workplace-based learning and continuing professional development. 11 The professional tensions identified at the student level likely persist into practice, making organizational attention to collaborative relationships essential for patient safety. Following high-profile maternity service failures highlighting communication breakdowns,11,12 healthcare organizations should prioritize collaborative training as a patient safety initiative rather than merely an educational enhancement.
Implications for Future Research
A critical research gap is identifying the components of effective IPE education that has the greatest effect on student learning (and likely effect on patient safety). Future studies should track participants through training completion into clinical practice, using objective behavioral measures rather than self-reported attitudes. This longitudinal research should examine whether early IPE intervention influences subsequent interprofessional relationships and patient safety outcomes. Comparative effectiveness studies directly comparing different IPE modalities (simulation versus problem-based learning versus community placement) would inform resource allocation decisions. The timing question requires further investigation. While our findings suggest early intervention benefits, controlled studies comparing IPE delivery at different educational stages could provide definitive guidance for curriculum sequencing.
Significant research gaps exist regarding successful IPE implementation specifically aimed at midwifery and medical students. Future studies should examine organizational factors supporting successful IPE integration in this context, including faculty development models, resource requirements, and sustainability strategies. Cost-effectiveness analyses comparing different implementation approaches would support evidence-based resource allocation. Future research should move beyond educational outcomes to examine patient safety and care quality impacts. Studies linking IPE participation to subsequent collaborative behavior in clinical settings and, ultimately, to patient outcomes would provide the most compelling evidence for continued investment in IPE. The specific context of maternal care, where doctor-midwife collaboration directly impacts safety outcomes, offers an ideal setting for examining patient centeredness-level benefits of educational interventions targeting interprofessional relationships.
Conclusion
This systematic review demonstrates that IPE interventions between medical and midwifery students effectively improve collaborative competencies across multiple learning domains, with simulation-based approaches showing particular promise. While implementation barriers exist, including scheduling challenges, the evidence supports early, structured IPE integration as both educationally beneficial and essential for patient safety. The unique hierarchical dynamics identified in this professional dyad highlight the importance of carefully designed interventions that address power imbalances while capitalizing on complementary expertise.
Supplemental Material
Supplemental Material - Interprofessional Education Between Undergraduate Medical and Midwifery Students: A Mixed-Methods Systematic Review
Supplemental Material for Interprofessional Education Between Undergraduate Medical and Midwifery Students: A Mixed-Methods Systematic Review by Nermin Abulibda, Shukrat O. Salisu-Olatunji, Clare L. Gillies, Lisa Jesson, Kerri Eilertsen-Feeney, Jonathan Corne, Jayne E. Marshall, Keith Nockels, Elizabeth Susan Anderson, Jeremy Howick in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors acknowledge the research team at the Stoneygate Centre for Empathic Healthcare for their continued support and guidance.
Ethical Considerations
This systematic review synthesized data from previously published studies and did not involve primary data collection with human participants. Therefore, ethical approval was not required.
Author Contributions
JH developed the idea for the study. JH conceptualized the project and methodology. KN developed the search strategy. NA and SOS contributed to screening and data extraction. JH, NA and SOS carried out data analysis and wrote the first manuscript. All authors contributed to the review and editing of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Health Service England (NHSE). NA and JH are also supported by the Stoneygate Trust. The funders had no role in developing the protocol, or in collecting or analyzing data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.