
Abstract
Purpose
To examine the Communication Skills Attitude Scale (CSAS) framework as a way to identify factors associated with medical students’ attitudinal engagement with communication skills training (CST) at the University of Tabuk, Saudi Arabia. To assess positive attitudes (Positive Attitude Scale; PAS) and negative attitudes (Negative Attitude Scale; NAS), and explore their associations with demographic and academic characteristics, compared attitudes across all six Bachelor of Medicine and Bachelor of Surgery (MBBS) years, and tested their associations with an attitudinal Engagement Index (EI).
Methods
A quantitative cross-sectional survey was conducted during the 2023-2024 academic year among undergraduate MBBS students. A convenience sample of 179 students completed the validated 26-item CSAS. The EI was calculated as PAS minus NAS and should be interpreted as an attitudinal proxy for engagement rather than a direct measure of observable learning behaviour. Descriptive statistics, reliability testing, paired and independent-samples t tests, and one-way analysis of variance (ANOVA) with Tukey post-hoc testing were used.
Results
PAS scores (mean 49.23, SD 6.89) were significantly higher than NAS scores (mean 37.42, SD 7.15; p<0.001). Female students had higher PAS and EI scores than male students. Academic-year differences were evident, with a marked decline in the fourth year. Because EI was mathematically derived from PAS and NAS (EI=PAS-NAS), PAS and NAS were not retained as independent predictors of EI in a regression model; EI was interpreted descriptively and through demographic and academic-year comparisons.
Conclusion
Negative attitudes toward CST were strongly associated with lower attitudinal engagement. The transition into clinically intensive learning, particularly the fourth year, appears to be a vulnerable period. Curriculum strategies should therefore address negative stereotypes about communication skills, explicitly connect CST to clinical reasoning and assessment, and provide visible role modelling in the clinical learning environment.
Keywords
Introduction
Effective communication is an established physician competency and is associated with diagnostic accuracy, patient adherence, patient safety, and clinician wellbeing. 1 For this reason, communication skills training (CST) is now expected within competency-based medical education frameworks and accreditation standards. 2 However, the presence of CST in a curriculum does not guarantee that students will value, practise, or internalize communication skills.
Students’ attitudes may be particularly important because they influence how learners interpret the relevance of a curricular activity. The Communication Skills Attitude Scale (CSAS), developed by Rees, Sheard and Davies, is one of the most widely used instruments for measuring medical students’ attitudes toward CST. 3 The CSAS distinguishes positive attitudes (Positive Attitude Scale; PAS) from negative attitudes (Negative Attitude Scale; NAS), treating them as related but separate constructs rather than opposite ends of a single continuum.
Engagement is often conceptualized as cognitive, emotional and behavioural investment in learning.4,5 The present study did not measure observed behavioural engagement directly, such as attendance, participation, communication-performance scores or learning analytics. Instead, it created an attitudinal Engagement Index (EI), calculated as PAS minus NAS, to summarize students’ net attitudinal inclination toward CST. Throughout this manuscript, EI is therefore interpreted as an attitudinal proxy for engagement, not as a direct measure of actual learning behaviour.
CST may be especially vulnerable to de-prioritization in clinical environments where biomedical knowledge, workload, assessment pressure, and hidden-curriculum messages can make communication appear secondary or intuitive rather than a teachable clinical skill.6-10 In some cohorts, patient-centred or communication-related attitudes decline during clinical clerkships. 7 Understanding when such shifts occur may help educators design timely and developmentally appropriate interventions.11,12
This study aimed to examine factors associated with medical students’ attitudinal engagement with CST at the University of Tabuk. The specific objectives were to: (1) describe PAS and NAS scores; (2) examine associations with gender, academic year and parental healthcare background; (3) compare PAS, NAS and EI across all six MBBS years; and (4) interpret EI as a derived attitudinal index rather than modelling PAS and NAS as predictors of a score constructed from them.13,14
Materials and Methods
Study Design and Setting
A quantitative cross-sectional study was conducted at the College of Medicine, University of Tabuk, Tabuk, Saudi Arabia, during the 2023-2024 academic year. The college offers a six-year undergraduate Bachelor of Medicine and Bachelor of Surgery (MBBS) program. Communication skills are introduced through curriculum modules and reinforced within clinical clerkships. The study is reported in line with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidance for cross-sectional studies. 11
Participants, Inclusion and Exclusion Criteria, and Sampling
The target population was all undergraduate medical students enrolled in Years 1-6 of the MBBS program during the study period. Inclusion criteria were: (1) active enrolment as a University of Tabuk MBBS student in Year 1, 2, 3, 4, 5 or 6; (2) age 18 years or older; (3) ability to understand the Arabic or English survey text; and (4) provision of electronic informed consent before starting the questionnaire. Exclusion criteria were: (1) students on leave of absence or not actively enrolled during data collection; (2) interns, postgraduate trainees, graduates or students from other colleges; (3) refusal or withdrawal of consent; and (4) incomplete questionnaires with missing CSAS items or duplicate submissions, where identifiable by timestamp and response pattern.
The target population included all undergraduate medical students between Year 1 and Year 6. Convenience sampling was employed because this exploratory survey depended on voluntary student participation through online distribution. This approach is consistent with the original CSAS-based study by Rees et al (2002), which used the Communication Skills Attitude Scale in a medical-student sample and is cited here as the methodological precedent. 3 The final analysed sample was 179 students. The achieved sample was smaller because participation was voluntary and convenience-based. Therefore, the study is interpreted as an exploratory cross-sectional analysis rather than a fully powered prevalence survey.
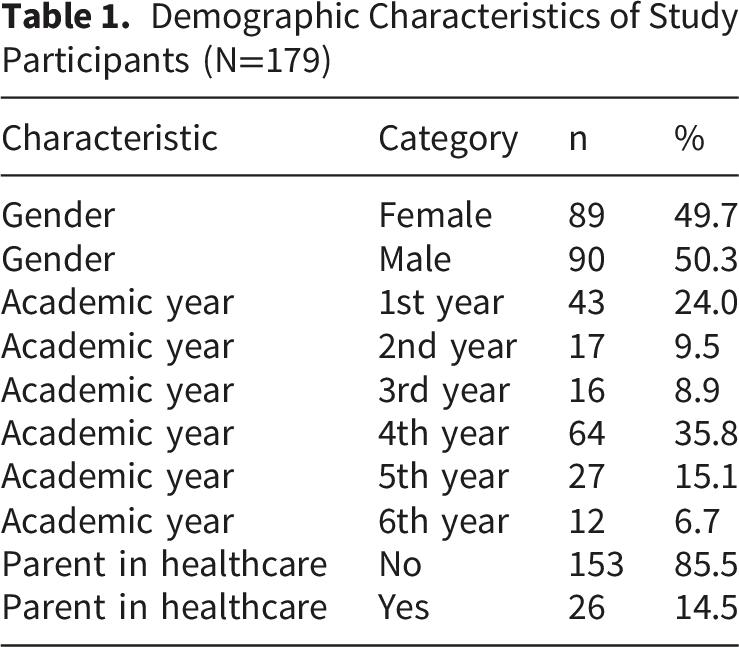
Demographic Characteristics of Study Participants (N=179)
Data Collection Instrument
The main instrument was the 26-item Communication Skills Attitude Scale (CSAS). 3 The CSAS includes two 13-item subscales: the Positive Attitude Scale (PAS), which measures favourable perceptions of CST, and the Negative Attitude Scale (NAS), which measures unfavourable perceptions of CST. Each item is rated on a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree), giving each subscale a possible score range of 13-65. Higher PAS scores indicate more positive attitudes; higher NAS scores indicate more negative attitudes. Negatively worded items were scored according to the standard CSAS approach before calculating subscale totals. The questionnaire was administered in bilingual English-Arabic format to support comprehension. Demographic items asked about gender, academic year, and whether either parent had education or employment in a healthcare field.
The attitudinal Engagement Index (EI) was calculated as PAS minus NAS. A higher EI indicates that favourable attitudes toward CST outweighed unfavourable attitudes. Because EI was derived from attitude scores only, it was not treated as a direct measure of behavioural or cognitive engagement.15,16
Data Collection Procedure
An anonymous online questionnaire was developed using Google Forms. Following ethical approval, the survey link was distributed through university email lists and student online social media groups. The landing page included participant information and an electronic informed-consent statement. Data collection continued for eight weeks, with periodic reminders. Participation was voluntary and no incentive was provided.
Data Analysis
Data were analyzed using IBM SPSS Statistics version 28.0 (IBM Corp., Armonk, NY, USA). Frequencies and percentages described categorical variables, while means and standard deviations summarized CSAS subscale scores and EI. Cronbach’s alpha assessed the internal consistency of PAS and NAS in the study sample. PAS and NAS scores were compared using a paired-samples t test. Independent-samples t tests examined score differences by gender and parental healthcare background. One-way ANOVA with Tukey honestly significant difference post-hoc testing compared PAS, NAS and EI across academic years. Statistical significance was set at p<0.05.
Ethical Considerations
The study protocol was approved by the Local Research Ethics Committee, University of Tabuk (Approval Reference No: UT-333-168-2023). All procedures complied with the ethical principles of the Declaration of Helsinki. Written informed consent was obtained electronically before survey completion. No personally identifying information was collected, and data were stored on a password-protected server accessible only to the research team.
Results
Participants
A total of 179 valid responses were included. The sample was almost gender balanced, with 90 male students (50.3%) and 89 female students (49.7%). Students from all six MBBS years participated; the largest subgroup was fourth-year students (n=64, 35.8%) and the smallest was sixth-year students (n=12, 6.7%). Because the denominator for each class year could not be verified from the distribution process, these values should be interpreted as respondent distribution rather than formal class response rates. Most respondents (n=153, 85.5%) reported that neither parent had education or employment in healthcare (Table 1).
Descriptive Statistics and Reliability
Descriptive Statistics for CSAS Subscales and Attitudinal Engagement Index
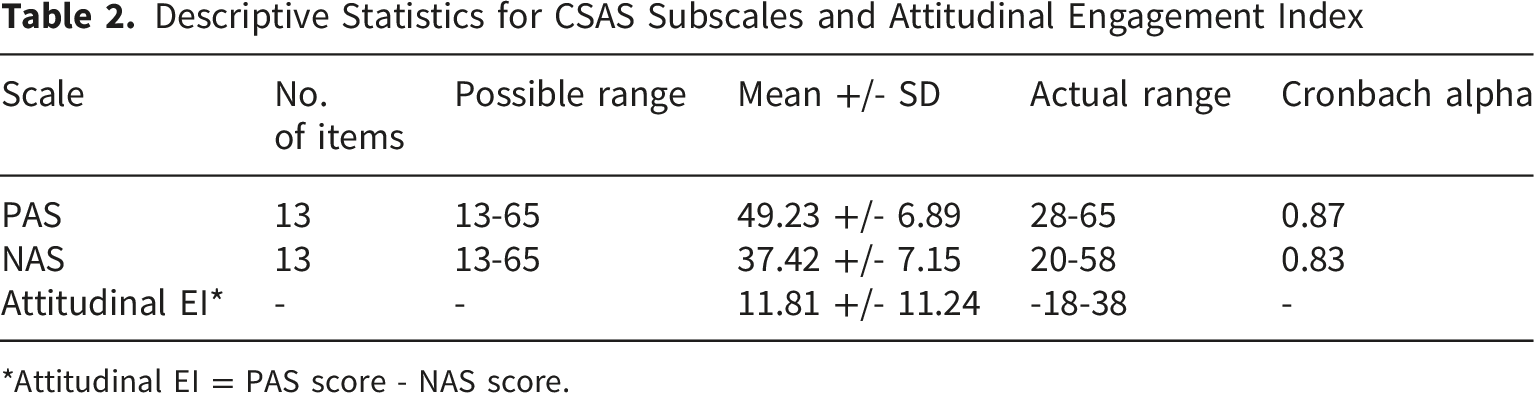
*Attitudinal EI = PAS score - NAS score.
Associations With Demographic Variables
Comparison of CSAS Scores by Gender and Parental Healthcare Background
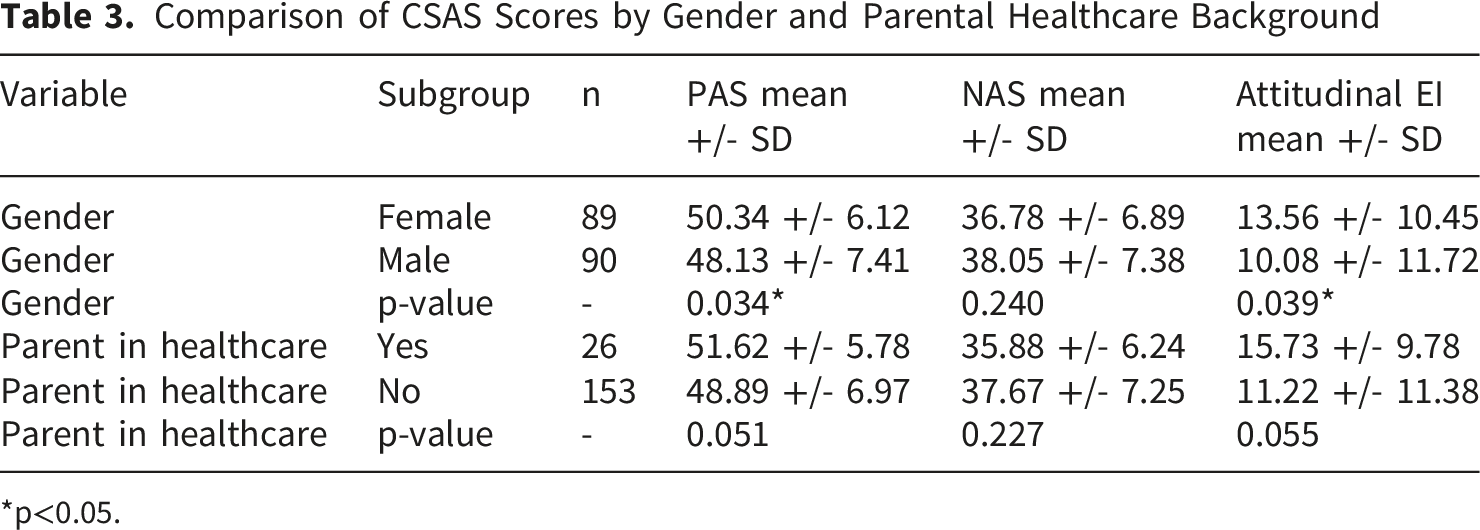
*p<0.05.
Differences by Academic Year
CSAS Scores and Attitudinal Engagement Index Across Academic Years
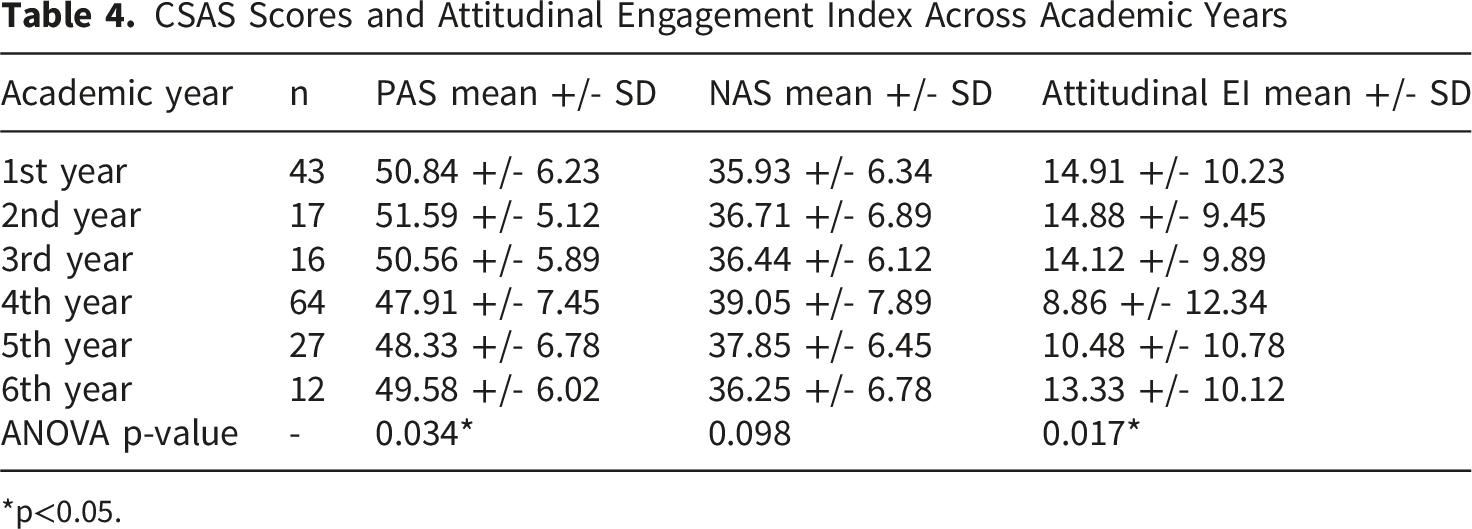
*p<0.05.
Discussion
Principal Findings
This cross-sectional CSAS-based study found that medical students reported stronger positive than negative attitudes toward CST. Female students reported higher PAS and EI scores than male students, and EI showed an academic-year pattern with a marked fourth-year decline. Importantly, following reviewer feedback, EI is now interpreted as a derived attitudinal index rather than as an outcome independently predicted by its component scores.
Interpretation and Educational Implications
The attitudinal Engagement Index is a helpful index that summarizes the relationship between positive and negative attitudes towards communication skills training among students. There is some empirical evidence indicating that overall, students are more likely to express positive rather than negative attitudes towards training, but a decreased EI in some samples, especially fourth-year students, could indicate a lower overall attitudinal orientation toward teaching of communication skills. These negative perceptions include: perceiving communication skills as monotonous, not clinically valuable or meaningful, poorly connected to assessment, or less important than biomedical education.
The fourth-year decline may reflect specific features of the clinical learning environment. Fourth-year students often encounter greater workload, new assessment pressures, early clerkship responsibilities, variable supervisor role modelling, and hidden-curriculum messages that can implicitly place technical knowledge above patient-centred communication.6-10,12 These pressures may make communication skills seem secondary to passing examinations or managing clinical tasks. The finding therefore supports integrating CST into clinical reasoning, ward-based feedback, objective structured clinical examinations and workplace-based assessment, rather than teaching it only as a preclinical or stand-alone topic.
The small gender difference, with higher PAS and EI among female students, is consistent with previous reports of more favourable communication or patient-centred attitudes among female learners.13,14 However, the effect was modest and should not be overinterpreted in this cross-sectional sample. Parental healthcare background showed a positive but non-significant trend, suggesting that exposure to healthcare culture may be relevant but should not be overinterpreted in this sample.15,16
Comparison With Previous Studies
The findings align with the original CSAS framework, which treats positive and negative attitudes as distinct dimensions. 3 They also agree with research indicating that communication and patient-centred attitudes can decline during clinical training and may be influenced by hidden-curriculum messages, assessment priorities and role-modelling.6,8,13,14 The revised analysis avoids overinterpreting a derived EI score and instead uses EI to summarize the balance between favourable and unfavourable attitudes.
Limitations
Several limitations should be considered. First, the cross-sectional design prevents causal inference; differences between academic years may reflect cohort effects rather than within-student developmental change. Second, the single-institution setting may limit generalizability. Third, convenience sampling, unequal year-group representation, and the inability to calculate class-specific response rates may limit representativeness and introduce selection bias. The small sixth-year subgroup (n=12) also reduces precision of year-level comparisons. Finally, the Engagement Index, derived from PAS and NAS, should be interpreted as an attitudinal proxy rather than evidence of actual behavioural or cognitive engagement. Future longitudinal studies should include objective engagement measures.
Generalizability
Despite these limitations, inclusion of students from all six years of an Arab undergraduate medical curriculum provides useful exploratory evidence for institutions with similar curricular structures. The findings may be most transferable to settings where CST is present in the curriculum but competes with workload, assessment pressures and clinical-culture messages.
Recommendations
Future research should use longitudinal designs to follow PAS, NAS and observed engagement outcomes over time. Future studies should also include independent indicators of engagement, such as attendance, observed participation, communication-performance assessments or learning analytics, before applying predictive models of engagement. Qualitative work with fourth-year students and clinical supervisors could clarify how workload, assessment pressure, role modelling and hidden-curriculum messages shape students’ attitudes toward CST.
Conclusion
Among medical students at the University of Tabuk, positive attitudes toward CST generally outweighed negative attitudes. EI, interpreted as PAS minus NAS, suggested less favourable net attitudinal engagement during the fourth year and among male students. Because EI is derived from PAS and NAS, it should not be modelled as an independent outcome predicted by those same subscale scores. Curriculum strategies should therefore focus on reducing negative stereotypes about CST, strengthening clinical role modelling and integrating communication skills more visibly into clinical reasoning and assessment.
Supplemental Material
Supplemental Material - What Shapes Medical Students’ Engagement With Communication Skills Learning in Tabuk- Saudi Arabia: A Cross-Sectional CSAS-Based Study
Supplemental Material for What Shapes Medical Students’ Engagement With Communication Skills Learning in Tabuk- Saudi Arabia: A Cross-Sectional CSAS-Based Study by Seham Sulieman Alhemaidi in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental Material - What Shapes Medical Students’ Engagement With Communication Skills Learning in Tabuk- Saudi Arabia: A Cross-Sectional CSAS-Based Study
Supplemental Material for What Shapes Medical Students’ Engagement With Communication Skills Learning in Tabuk- Saudi Arabia: A Cross-Sectional CSAS-Based Study by Seham Sulieman Alhemaidi in Journal of Medical Education and Curricular Development.
Footnotes
Acknowledgements
The author thanks the medical students of the University of Tabuk for their participation and the College of Medicine administration for supporting data collection.
Ethical Considerations
This study was reviewed and approved by the Local Research Ethics Committee, University of Tabuk (Approval Reference No: UT-333-168-2023).
Consent to Participate
Written informed consent was obtained electronically from each participant before survey completion.
Consent for Publication
Consent to publish aggregated findings was included in the electronic consent process.
Author Contributions
SSA contributed to conceptualization, methodology, data curation, formal analysis, validation, project administration, writing the original draft, and writing-review and editing.
Funding
The author received no financial support for the research, authorship or publication of this article.
Declaration of Conflicting Interests
The author declares no potential conflicts of interest with respect to the research, authorship or publication of this article.
Data Availability Statement
Data are available from the author upon reasonable request and subject to ethical approval requirements.
Disclosure
AI-assisted language-editing support was used during revision to improve grammar, clarity and organization. The author remains responsible for the content, data analysis, interpretation and final manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.